Electrical safety
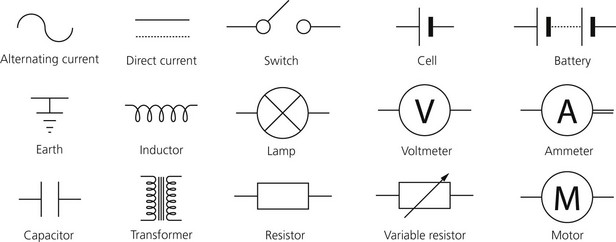
Principles of electricity (Fig. 14.1)
Identification of medical electrical equipment












Drip Proof, Splash Proof, Water Tight

Depending on the nature and use of the equipment, some are drip proof, splash proof or water proof.



Hazards of electrical shock
Damage caused by electrical shock can occur in two ways:
1. Disruption of the normal electrical function of cells. This can cause contraction of muscles, alteration of the cerebral function, paralysis of respiration and disruption of normal cardiac function resulting in ventricular fibrillation.
2. Dissipation of electrical energy throughout all the tissues of the body. This leads to a rise in temperature due to the flow of electrons, and can result in burns.
The severity of the shock depends on:
1. The size of current (number of amperes) per unit of area.
2. Current pathway (where it flows). A current passing through the chest may cause ventricular fibrillation or tetany of the respiratory muscles leading to asphyxia. A current passing vertically through the body may cause loss of consciousness and spinal cord damage.
3. The duration of contact. The shorter the contact, the less damage caused.
4. The type of current (AC or DC) and its frequency. The higher the frequency, the less risk to the patient. A 50-Hz current is almost the most lethal frequency. The myocardium is most susceptible to the arrthymogenic effects of electric currents at this frequency and muscle spasm prevents the victim letting go of the source. As the frequencies increase to >1 kHz, the risks decrease dramatically.
Diathermy
Mechanism of action
1. Heat is generated when a current passes through a resistor depending on the current density (current per unit area). The amount of heat generated (H) is proportional to the square of current (I2) divided by the area (A) (H = I2/A). So the smaller the area, the greater the heat generated. The current density around the active electrode can be as much as 10 A/cm2 generating a heating power of about 200 W.
2. A large amount of heat is produced at the tip of the diathermy forceps because of its small size (high current density). Whereas at the site of the patient’s plate, because of its large surface area, no heat or burning is produced (low current density).
3. A high-frequency current (in the radiofrequency range) of 500 000 to more than 1 000 000 Hz is used. This high-frequency current behaves differently from the standard 50-Hz current. It passes directly across the precordium without causing ventricular fibrillation. This is because high-frequency currents have a low tissue penetration without exciting the contractile cells.
4. The isolating capacitor has low impedance to a high-frequency current, i.e. diathermy current. The capacitor has a high impedance to 50-Hz current thus protecting the patient against electrical shock.
5. Earth-free circuit diathermy can be used. The patient, the tip of the diathermy forceps and the patient plate are not connected to earth. This reduces the risk of burns to the patient. This type of circuit is known as a floating patient circuit.
6. Cutting diathermy uses a continuous sine waveform at a voltage of 250–3000 V. Coagulation diathermy uses a modulated waveform. Coagulation can be achieved by fulguration or desiccation. Blended modes (cutting and coagulation) can be used with a variable mixture of both cutting and coagulation.
7. Bipolar diathermy does not require a patient plate. The current flows through one side of the forceps, through the patient and then back through the other side of the forceps. The current density and heating effect are the same at both electrodes. Usually low power can be achieved from a bipolar diathermy with good coagulation effect but less cutting ability. Bipolar diathermy is frequently used during neurosurgery or ophthalmic surgery.
Problems in practice and safety features
1. If the area of contact between the plate and patient is reduced, the patient is at risk of being burned at the site of the plate. If the plate is completely detached, current might flow through any point of contact between patient and earth, for example earthed ECG electrodes or temperature probes. Modern diathermy machines do not function with any of the above.
2. Electrical interference with other electrical monitoring devices. The use of electrical filters can solve this problem.
3. Interference with the function of cardiac pacemakers. Damage to the electrical circuits or changes in the programming can occur. This is more of a hazard with cutting diathermy than with coagulation diathermy. Modern pacemakers are protected against diathermy.
4. Fires and explosions may be caused by sparks igniting flammable material such as skin cleansing solutions or bowel gas.
Static electricity
Some of the measures used to prevent the build-up of static electricity are:
1. Tubings, reservoir bags and face masks are made of carbon-containing rubber; they are black in colour with yellow labels.
2. Staff wear anti-static footwear.
3. Trolleys have conducting wheels.
4. The relative humidity in the operating theatre is kept at more than 50% with a room temperature of more than 20°C.
Lasers
Problems in practice and safety features
1. Permanent damage to the eye retina or the head of the optic nerve can be caused by laser beams in the visible portion. Infrared light can cause damage to cornea, lens and aqueous and vitreous humours. All staff should wear eye protection appropriate for the type of laser and within the laser-controlled area. This should offer adequate protection against accidental exposure to the main beam. Spectacles do not give reliable peripheral visual field protection.
2. Burning can be caused if the laser hits the skin.
3. A non-water-based fire extinguisher should be used immediately.
4. All doors should be locked and all windows covered in order to protect those outside the operating theatre.
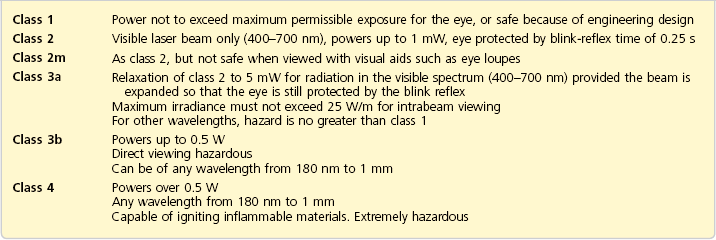
Table 14.1 shows the different classes of laser products.
Boumphrey S., Langton J.A. Electrical safety in the operating theatre. BJA CPED Reviews. 2003;3:10–14.
ebme.co.uk, no date. Safety testing of medical and electrical equipment. Online. Available at: http://www.ebme.co.uk/arts/safety/index.htm.
Kitching A.J., Edge C.E. Laser and surgery. BJA CPED Reviews. 2003;8:143–146.
MHRA. DB 2008(03): guidance on the safe use of lasers, IPL systems and LEDs. Online. Available at http://www.mhra.gov.uk/Publications/Safetyguidance/DeviceBulletins/CON014775, 2008.
MHRA. Electrosurgery. Online. Available at http://mhra.gov.uk/learningcentre/ESUGenericModuleCertificate/player.html, 2012.
In the following lists, which of the statements (a) to (e) are true?
1. Concerning electric current:
a) Inductance is a measure of the ability to store a charge.
b) Mains current in the UK is at a frequency of 50 Hz.
c) The leakage current of a central venous pressure monitoring device should be less than 10 mA.
d) Current density is the current flow per unit of area.
e) In alternating current, the flow of electrons is in one direction.
a) When current flow depends on the frequency, impedance is used in preference to resistance.
b) The impedance of an inductor to low-frequency current is high.
c) Isolating capacitors in surgical diathermy are used because of their low impedance to high-frequency current.
d) With ECG, skin electrodes need a good contact to reduce impedance.
3. Which of the following statements are correct?
a) With equipotentiality, all metal work is normally at or near zero voltage.
b) Functional earth found on medical devices acts as a safety feature.
c) Ohm’s law states that electric resistance = current × potential difference.
d) Type CF equipment can be safely used with direct connection to the heart.
a) It does not happen with direct current.
b) The main impedance is in the muscles.
c) A current of 50 Hz is lethal.
d) A current of 100 mA applied to the surface of the body can cause ventricular fibrillation.
1. Concerning electric current:
a) False. Inductance occurs when a magnetic field is induced as electrons flow in a wire. The ability to store a charge is known as capacitance. In an inductor, the impedance is proportional to the frequency of the current. In a capacitor, impedance is inversely proportional to the current frequency.
b) True. The frequency of the mains supply in the UK is 50 Hz. At this relatively low frequency, the danger of electric shock is high.
c) True. A central venous pressure monitoring device can be in direct contact with the heart. Ventricular fibrillation can occur with very small current, between 50 and 100 mA, as the current is applied directly to the myocardium (microshock). Such devices should have a leakage current of less than 10 mA to prevent microshock.
d) True. The amount of current flow per unit of area is known as the current density. This is important in the function of diathermy. At the tip of the diathermy forceps, the current density is high so heat is generated. At the patient plate, the current density is low and no heat is generated.
e) False. In alternating current, the flow of electrons reverses direction at regular intervals. In the UK, the AC is 50 cycles per second (Hz). In direct current, the flow of electrons is in one direction only.
a) True. Impedance is the sum of the forces that oppose the movement of electrons in an AC circuit. In capacitors, the impedance is low to high-frequency current and vice versa. The opposite is correct in inductors.
b) False. Inductors have low impedance to low-frequency current and vice versa.
c) True. Capacitors have low impedance to high-frequency current and high impedance to low-frequency current. The latter is of most importance in protecting the patient from low-frequency current. High-frequency currents have low tissue penetration without exciting the contractile cells, allowing the current to pass directly across the heart without causing ventricular fibrillation.
d) True. The skin forms the main impedance against the conduction of the ECG signal. In order to reduce the skin impedance, there should be good contact between the skin and the electrodes.
e) True. Ohms are used to measure both impedance and electrical resistance. Ohm = volt/ampere.
3. Which of the following statements are correct?
a) True. Equipotentiality is a safety feature when, under fault conditions, all metalwork increases to the same potential. Current will not flow during simultaneous contact between two such metal appliances as they are both at the same potential and no shock results.
b) False. Functional earth is not a safety feature. It is necessary for the proper functioning of the device. It is part of the main circuit where the current, via the neutral wire, is returned to the substation and so to earth.
c) False. Ohm’s law states that the potential difference (volts) = current (ampere) × resistance (ohms).
d) True. Type CF equipment can be used safely in direct contact with the heart. The leakage current is less than 50 µA in class I and less than 10 µA in class II, providing a high degree of protection against electrical shock.
e) False. Type B equipment can be provided with defibrillator protection. The same applies to type BF and type CF equipment.
a) False. Electric shock can happen with direct current although the amount of current required to cause ventricular fibrillation is much higher than that of alternating current.
b) False. The main impedance is in the skin and not the muscles. Skin impedance is variable and can be from 100 000 to 1 000 000 Ω depending on the area of contact and whether or not the skin is wet.
c) True. The severity of the electric shock depends on the frequency of the current. The lower the frequency, the higher the risk. A current of 50 Hz is almost the most lethal frequency.
d) True. A current of 100 mA, when applied to the surface of the body, can cause ventricular fibrillation. Most of the current is lost as the current travels through the body and only 50–100 µA are required to cause ventricular fibrillation.
e) True. The electrical energy is dissipated throughout the tissues of the body leading to a rise in temperature and resulting in burns.
a) False. In order to protect the patient from burns, the current density at the plate should be low. The same current is passed through the tip of the diathermy forceps where the current density is high, thus producing heat. The current density at the plate is low because of its large surface area.
b) True. The isolating capacitor protects the patient from low-frequency current (50 Hz) shock because of its high impedance to low-frequency currents. It has low impedance to high-frequency (diathermy) currents.
c) True. A floating patient circuit can be used to reduce the risk of burns. The diathermy circuit is earth free. The patient, the tip of the diathermy forceps and the patient’s plate are not connected to earth.
d) True. Diathermy can cause electrical interference with ECG and other monitoring devices. The use of electrical filters can solve this.
e) False. Very-high-frequency current (in the radiofrequency range) of 500 000 to 1 000 000 Hz is used. This high-frequency current behaves differently from the standard 50-Hz current; because of its low tissue penetration, it passes directly through the heart without causing ventricular fibrillation.