ELBOW
SELECTED MOVEMENTS

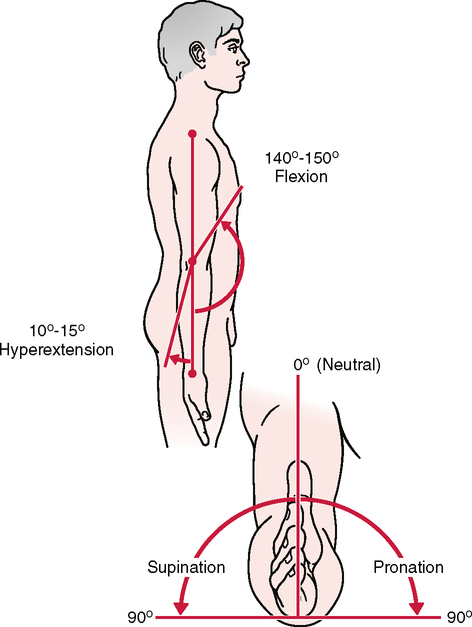
• The examiner should test active flexion in a neutral position as well as in the fully pronated and supinated positions. Differences in flexion ROM should be noted.
• Terminal flexion loss is more disabling than the same degree of terminal extension loss, because flexion is needed for so many activities of daily living. Loss of either motion affects the reach of the hand, which in turn affects function.
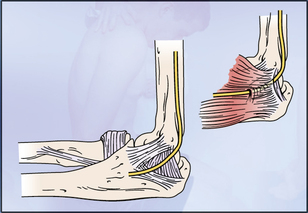
• Normally, the extension movement is arrested by the locking of the olecranon process of the ulna into the olecranon fossa of the humerus. Loss of elbow extension is a sensitive indicator of an intra-articular pathological condition. It is the first movement lost after injury to the elbow and the first regained with healing.
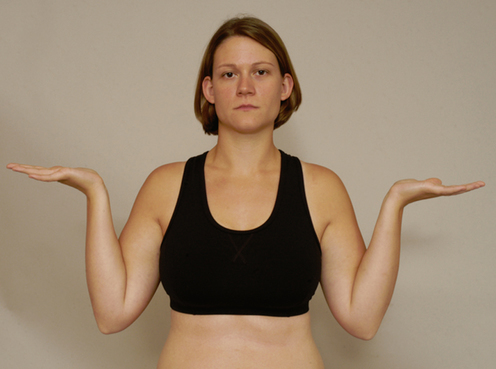
• The examiner should make sure the patient does not abduct the shoulder in an attempt to increase the amount of pronation or to compensate for a lack of sufficient pronation.
• For both supination and pronation, only about 75° of movement occurs in the forearm articulations; the remaining 15° is the result of wrist action.
• The examiner should make sure the patient’s shoulder does not adduct further in an attempt to give the appearance of increased supination or to compensate for a lack of sufficient supination.
• Loss of ROM with supination often is the result of wrist injuries or fracture. Therefore, loss of motion or symptom reproduction with supination does not always imply a pathological condition of the elbow.
• If the patient history includes a complaint that combined movements, repetitive movements, or sustained positions cause pain, these specific movements should be included in the active movement assessment.

• Passive movements should be carried out carefully to test the end feel and to test for a capsular pattern. Tissue approximation is the normal end feel of elbow flexion; in thin patients, the end feel may be bone to bone as a result of the coronoid process of the ulna hitting in the coronoid fossa of the humerus. Pronation also may be bone to bone in thin individuals. The examiner should note whether a capsular pattern is present.
• The capsular pattern for the elbow complex as a whole is more limitation of flexion than extension.
RESISTED ISOMETRIC MOVEMENTS3,4 

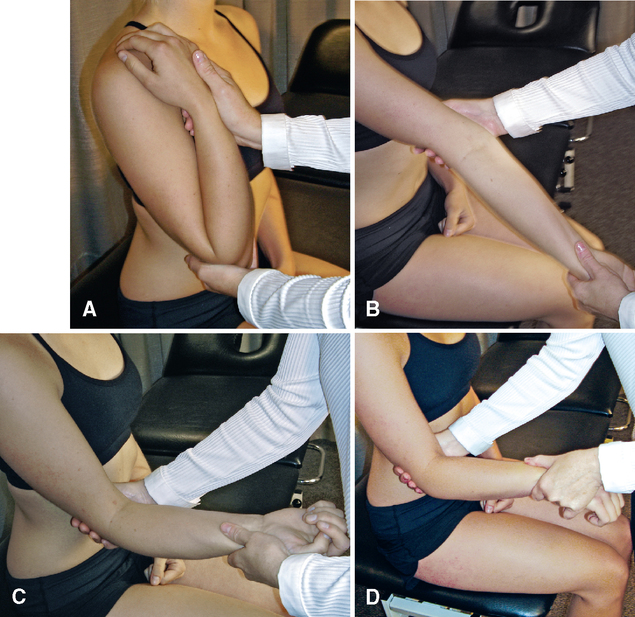
Elbow flexion. The examiner places the palm of his or her hand on the superior aspect of the patient’s forearm to provide resistance.
Elbow extension. The examiner places the palm of his or her hand on the inferior aspect of the patient’s forearm to provide resistance.
Pronation. The examiner grasps the patient’s forearm to provide resistance.
Supination. The examiner grasps the patient’s forearm to provide resistance.
Wrist flexion. The examiner holds the patient’s palm with one hand to provide resistance while stabilizing the forearm with the other.
Wrist extension. The examiner holds the dorsum of the patient’s hand with one hand to provide resistance while stabilizing the forearm with the other.
• If the patient has complained that combined movements under load, repetitive movements under load, or sustained positions under load cause pain, the examiner should carefully examine these resisted isometric movements and positions as well, but only after the basic movements have been tested isometrically.
• Muscle flexion power around the elbow is greatest in the range of 90° to 110° with the forearm supinated. At 45° and 135°, flexion power is only 75% of maximum.
• Research shows that men isometrically are two times stronger than women when testing elbow strength. In both men and women, extension is 60% of flexion and pronation is about 85% of supination.
• If the history indicates that concentric, eccentric, or econcentric movements have caused symptoms, these movements should also be tested with load or no load as required.
SPECIAL TESTS FOR LIGAMENTOUS INSTABILITY
Relevant Special Tests
Ligamentous valgus instability test
Ligamentous varus instability test
Relevant History
Patients may or may not have a prior history of damage to the elbow. Lateral instability occurs after elbow dislocation in 75% of cases.13 Athletes who participate in overhead sports may have a history of lower extremity or back pain that does not allow normal throwing mechanics. This can lead to excessive stress in the elbow, especially on the medial collateral ligament.
Mechanism of Injury
Dislocation/Subluxation
Repetitive Stress Injuries
LIGAMENTOUS VALGUS INSTABILITY TEST14,15 

• Regan and Morrey15 recommend doing the valgus stress test with the humerus in full lateral rotation.
• Because the medial collateral ligament is multipennated and is designed to resist stress in multiple directions, the examiner should test the elbow in varying degrees of extension and flexion to test the various fibers of the ligament.
LIGAMENTOUS VARUS INSTABILITY TEST16 

• Regan and Morrey15 recommend doing the varus stress test with the humerus in full medial rotation.
• Posterolateral elbow instability is the most common pattern of elbow instability in which there is displacement of the ulna (accompanied by the radius) on the humerus so that the ulna supinates or laterally rotates away from or off the trochlea.


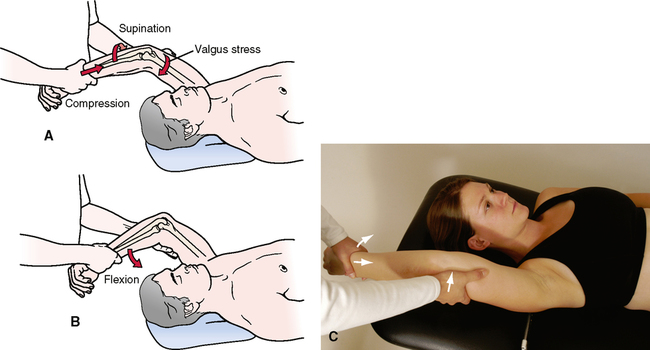
MOVING VALGUS STRESS TEST14,17 
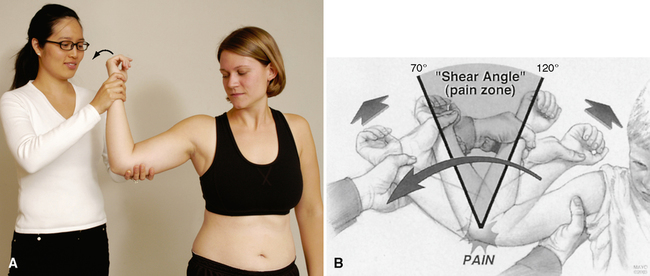

• If the patient is unconscious, subluxation and a clunk on reduction when the elbow is extended also may occur; however, these symptoms seldom are seen in a conscious patient.
• Care must be taken to ensure that the hand delivering the valgus force is on the humerus and not on the radius, which would block the radius’ ability to sublux laterally.




SPECIAL TEST FOR EPICONDYLITIS
Relevant Special Test
Lateral epicondylitis test (tennis elbow or Cozen’s test)
Relevant Signs and Symptoms
Medial Epicondylitis/Epicondylosis
• Grasp/grip strength is weak, and pain occurs with repetitive wrist flexion and pronation.
• Elbow flexion contracture is uncommon but can occur in a throwing athlete.
• Pain may be described as a dull ache immediately after activity and at rest or as a sharp or achy pain that radiates down the medial forearm.
Lateral Epicondylitis/Epicondylosis
• Local tenderness is present directly over the lateral epicondyle, and occasional forearm referral symptoms occur.
• Pain is aggravated by strong gripping.
• Grip strength is diminished because extensor muscles stabilize the wrist during grip.
• Pain occurs with passive stretching of the palmar forearm muscles.
• Radiography reveals tendon calcification in 20% of patients.
Specificity/Sensitivity Comparison
LATERAL EPICONDYLITIS TEST (TENNIS ELBOW OR COZEN’S TEST)26 
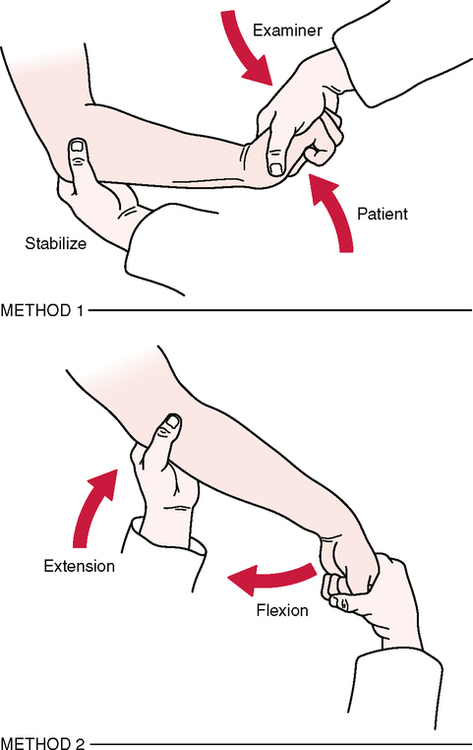
• Although classically designed to test for lateral epicondylitis, this technique can be used to test for any pathological condition of the lateral epicondyle.
• The examiner should be aware that the passive test stretches the radial nerve, which may lead to symptoms that may be similar to those seen with tennis elbow.
SPECIAL TESTS FOR NEUROLOGICAL SYMPTOMS
Relevant Special Tests
Mechanism of Injury
Cubital Tunnel Syndrome
Pronator Teres Syndrome


JOINT PLAY MOVEMENTS
RADIAL DEVIATION OF THE ULNA AND RADIUS ON THE HUMERUS 

• Radial deviation of the ulna and radius on the humerus is performed in a fashion similar to that used for the radial collateral ligament test but with less elbow flexion.
• When examining the joint play movements, the examiner must compare the injured side with the unaffected side.
• When the patient’s elbow is almost straight (extended) during the movement, the end feel should be bone to bone.
ULNAR DEVIATION OF THE ULNA AND RADIUS ON THE HUMERUS 

• Ulnar deviation of the ulna and radius on the humerus is performed in a fashion similar to that used for the ulnar collateral ligament test but with less elbow flexion.
• When examining the joint play movements, the examiner must compare the injured side with the unaffected side.
• When the patient’s elbow is almost straight (extended) during the movement, the end feel should be bone to bone.


ANTERIOR-POSTERIOR GLIDE OF THE RADIUS ON THE HUMERUS 
• Commonly, posterior gliding movement is easier to obtain than anterior glide (see the next test).
• This movement must be performed with care, because it can be very painful as a result of pinching of the skin between the examiner’s digits and the bone.
• Pain may result from application of the force even in the normal arm; therefore, the two sides must be compared for differences in symptoms.