• Lymphoma: Bulky submucosal mass without obstruction
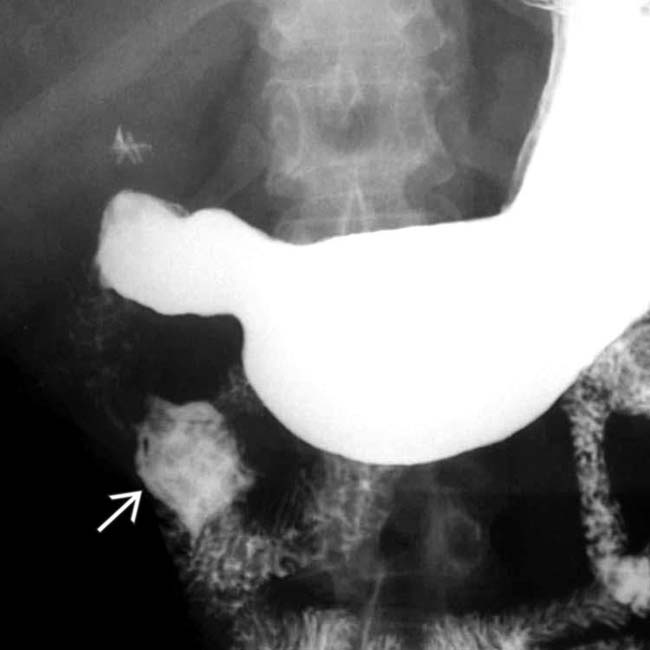
(Left) Spot film from from an upper GI series shows an ulcerated mass arising from the 2nd portion of the duodenum. There is a persistent pooling of barium within the lesion after the remainder of the duodenum has cleared.
(Right) Axial CECT in the same patient reveals a high-attenuation mass within the wall of the 2nd duodenum. A metastatic tumor was confirmed at surgery with the same histology as the primary colon cancer.
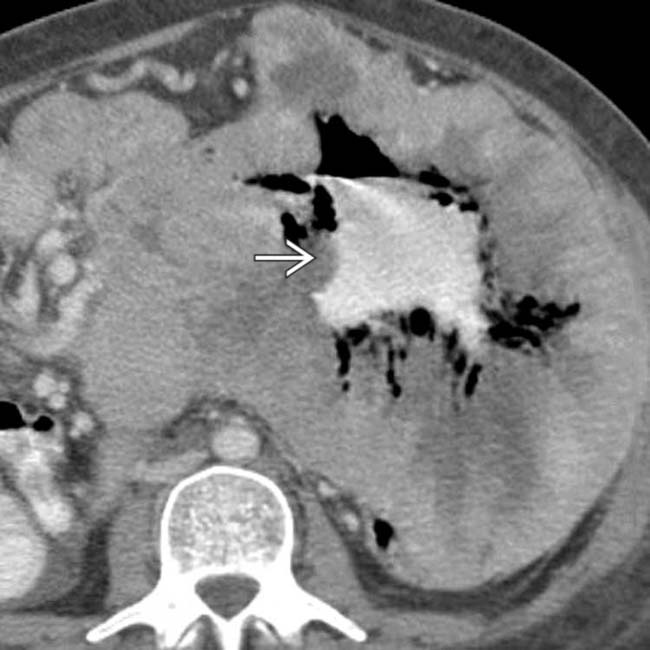
(Left) Small bowel follow-through in a liver transplant recipient, who presented with upper gastrointestinal pain and bleeding, shows a large amorphous collection of barium apparently arising from, and in continuity with, the distal duodenum. There is no evidence of bowel obstruction.
(Right) Axial CECT in the same patient shows a large soft tissue density mass arising from the distal duodenum. This is a good example of aneurysmal dilation of the bowel lumen caused by lymphoma.
TERMINOLOGY
Definitions
• Involvement of duodenum with malignant lymphoma or metastatic disease
IMAGING
General Features
• Best diagnostic clue
Metastases: Bull’s-eye or “target” lesion; submucosal or polypoid mass
Lymphoma: Bulky submucosal mass without obstruction of lumen
• Location
Submucosal lesion in any portion of duodenum
• Size
1-5 cm
• Morphology
Lymphoma: Smooth submucosal, often bulky mass
Fluoroscopic Findings
• Upper GI
Metastases: “Target” or bull’s-eye lesion with rounded submucosal mass; luminal obstruction and ulceration are common
–
Lymphoma: Large smooth or lobulated submucosal mass; aneurysmal dilation of lumen without obstruction
–
CT Findings
• CECT
Hematogenous metastasis appears as rounded submucosal mass
Direct invasion from primary tumor of pancreas, colon, kidney, gallbladder, or retroperitoneal node
Lymphoma: Bulky hypovascular soft tissue mass
– Stomach and duodenum may be involved contiguously
MR Findings
• T1WI
Low signal duodenal mass
• T2WI
Intermediate signal mass
• T1WI C+
Variable enhancement: Adenocarcinoma typically hypovascular; melanoma may be hypervascular
Imaging Recommendations
• Best imaging tool
Upper GI series, CECT
DIFFERENTIAL DIAGNOSIS
Villous Adenoma
• Bulky mucosal polypoid mass (3-9 cm); rarely causes obstruction
• Risk of cancer increases with size; 30-60% of tumors have malignant changes
Duodenal Carcinoma
• More likely to appear as an “apple core,” annular, obstructing lesion
Localized lymphoma: Surgery best option, to avoid bleeding and perforation
DIAGNOSTIC CHECKLIST
Consider
• Duodenal carcinoma
Image Interpretation Pearls
• Lymphoma: Bulky submucosal mass without obstruction
Axial CECT shows a submucosal soft tissue infiltrating mass due to lymphoma.
Axial CECT demonstrates a bulky soft tissue mass involving the duodenum . Biopsy revealed lymphoma.
Axial CECT of duodenal lymphoma shows extensive infiltration of the duodenum by a soft tissue mass .
Axial CECT of duodenal lymphoma demonstrates that a bulky mass infiltrates the duodenum, invades the mesentery, and extends into the superior mesenteric vein .
CT shows no sign of gastric outlet obstruction in this patient with massive small bowel lymphoma
CT in the same case shows a huge tumor mass enveloping the duodenum and jejunum. The center of the mass is cavitated and oral contrast media and gas flow through the mass into distal small bowel. The “lumen” of the bowel appears to be dilated, but the bowel wall has been completely replaced by tumor.
CT in the same case shows “aneurysmal dilation” of the bowel lumen.
CT shows the huge tumor mass enveloping the duodenum and jejunum. The center of the mass is cavitated and oral contrast media and gas flow through the mass into distal small bowel. The “lumen” of the bowel appears to be dilated (aneurysmal dilation), but the bowel wall has been completely replaced by tumor.
In the same case, a section through the pelvis shows peritoneal metastases .
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Metastases: Bull’s-eye or “target” lesion; submucosal or polypoid mass
Lymphoma: Bulky submucosal mass without obstruction
• Best imaging tool: Upper GI series, CECT
• Metastases: “Target” or bull’s-eye lesion with rounded submucosal mass
Luminal obstruction and ulceration are common
• Lymphoma: Large smooth or lobulated submucosal mass
Aneurysmal dilation of lumen without obstruction
• Direct invasion: From primary cancer of pancreas, colon, kidney, gallbladder
• Lymphoma: Bulky submucosal mass without obstruction
(Left) Spot film from from an upper GI series shows an ulcerated mass arising from the 2nd portion of the duodenum. There is a persistent pooling of barium within the lesion after the remainder of the duodenum has cleared.
(Right) Axial CECT in the same patient reveals a high-attenuation mass within the wall of the 2nd duodenum. A metastatic tumor was confirmed at surgery with the same histology as the primary colon cancer.
(Left) Small bowel follow-through in a liver transplant recipient, who presented with upper gastrointestinal pain and bleeding, shows a large amorphous collection of barium apparently arising from, and in continuity with, the distal duodenum. There is no evidence of bowel obstruction.
(Right) Axial CECT in the same patient shows a large soft tissue density mass arising from the distal duodenum. This is a good example of aneurysmal dilation of the bowel lumen caused by lymphoma.
TERMINOLOGY
Definitions
• Involvement of duodenum with malignant lymphoma or metastatic disease
IMAGING
General Features
• Best diagnostic clue
Metastases: Bull’s-eye or “target” lesion; submucosal or polypoid mass
Lymphoma: Bulky submucosal mass without obstruction of lumen
• Location
Submucosal lesion in any portion of duodenum
• Size
1-5 cm
• Morphology
Lymphoma: Smooth submucosal, often bulky mass
Fluoroscopic Findings
• Upper GI
Metastases: “Target” or bull’s-eye lesion with rounded submucosal mass; luminal obstruction and ulceration are common
–
Buy Membership for Radiology Category to continue reading. Learn more here







 arising from the 2nd portion of the duodenum. There is a persistent pooling of barium within the lesion after the remainder of the duodenum has cleared.
arising from the 2nd portion of the duodenum. There is a persistent pooling of barium within the lesion after the remainder of the duodenum has cleared.
 within the wall of the 2nd duodenum. A metastatic tumor was confirmed at surgery with the same histology as the primary colon cancer.
within the wall of the 2nd duodenum. A metastatic tumor was confirmed at surgery with the same histology as the primary colon cancer.
 apparently arising from, and in continuity with, the distal duodenum. There is no evidence of bowel obstruction.
apparently arising from, and in continuity with, the distal duodenum. There is no evidence of bowel obstruction.
 arising from the distal duodenum. This is a good example of aneurysmal dilation of the bowel lumen caused by lymphoma.
arising from the distal duodenum. This is a good example of aneurysmal dilation of the bowel lumen caused by lymphoma.

























 due to lymphoma.
due to lymphoma.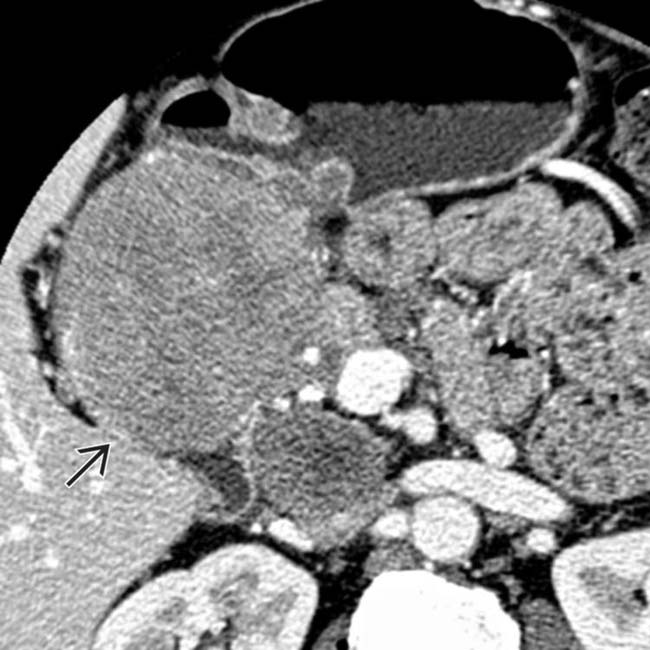
 . Biopsy revealed lymphoma.
. Biopsy revealed lymphoma.
 .
.
 .
.


 appears to be dilated (aneurysmal dilation), but the bowel wall has been completely replaced by tumor.
appears to be dilated (aneurysmal dilation), but the bowel wall has been completely replaced by tumor.
 .
. Metastases: “Target” or bull’s-eye lesion with rounded submucosal mass; luminal obstruction and ulceration are common
Metastases: “Target” or bull’s-eye lesion with rounded submucosal mass; luminal obstruction and ulceration are common
