Chapter 44 Double-Spike Plate
Cortical Fixation Device Enabling Graft Fixation Under Optional Tension
Background and Basic Concept
The pullout technique by tying sutures around a screw post or over a button is commonly used as a stand-alone fixation or as an augmentation for interference screw fixation into a tibial bone tunnel in the final stage of anterior cruciate ligament (ACL) or other ligament reconstruction. As the step of tensioning cannot be separated from that of fixation in this technique, the following problems have remained unsolved: loosening or breakage of the sutures while tying sutures around a post1 and difficulty in correctly controlling the tension to the graft.2 In order to solve these problems, a fixation device, the double-spike plate (DSP) (Ref. 020A-004, MEIRA Corp., Nagoya, Aichi, Japan) was developed to separate the step of tensioning from that of fixation.1 This device is currently commercially-sold only in Japan by Smith & Nephew Japan but will be shortly launched into the world market.
Specifications and Instruments for Use
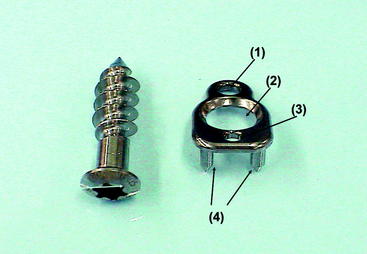
The DSP is a small plate made of titanium alloy with three holes and two spikes on the reverse side (Fig. 44-1). There are two sizes available: the standard DSP for big knee or single tunnel reconstruction (11 mm wide × 18 mm long × 1.5 mm thick with two spikes of 5.5 mm length) to be used with a 6.5-mm screw and the small DSP for a small knee or double-bundle procedure (8.5 mm wide × 13.8 mm long × 1.5 mm thick with spikes of 4.2 mm length) to be used with a 5-mm screw (see Fig. 44-1). The impactor is available for securely hammering base spikes into the cortical bone (Fig. 44-2). The centering drill guide is also available for creating a screw hole.

Rationale for Maintaining the Tension During Graft Fixation to the Tibia
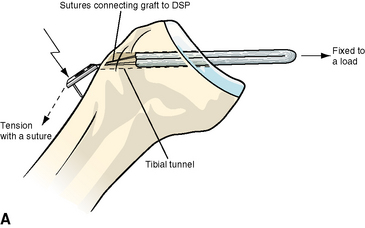
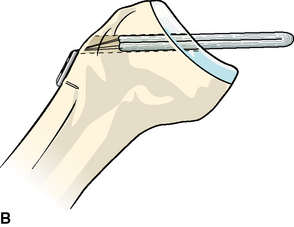
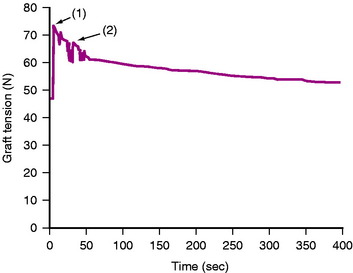
If the top end of the DSP closely keeps in close contact with the tibial cortex without movement, the DSP should show hinge motion around its top in the sagittal plain while its spikes are hammered into the tibia (Fig. 44-3). Thus the prehammering tension of the graft suture that has already been tied to the top hole could be assumed to be equal to its post-hammering tension. Although there is an instant increase of the tension due to minimal distal movement of the plate when the base spikes are hammered into the cortex, the tension goes down almost to the predetermined level after load relaxation for a minute or two (Fig. 44-4).
In Vitro Biomechanical Data Using Porcine Tibiae and Bovine Flexor Tendons
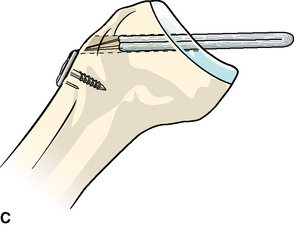
Ten fresh frozen porcine tibias, in which 8-mm drill holes had been created from just medial to the tibial tubercle to the attachment of the ACL, were rigidly fixed to an Instron tension analyzer. Using bovine tendons, a quadrupled graft consisting of two double-looped tendons of 7 cm in length and 8 mm in diameter were prepared with baseball glove stitching using #3 braided polyester sutures at the distal end of the graft. The graft was passed through the drill hole, and its proximal loop ends were connected to a load cell for monitoring tension (see Fig. 44-3, A). The graft sutures were tied to a standard-sized DSP through its top hole, pretensioned at 49N or 98N for 5 minutes, and temporarily fixed to the tibia by hammering the spikes on its reverse side to the anterior surface of the tibia (see Fig. 44-3, B). Permanent fixation was achieved by inserting a 6.5-mm cancellous screw (see Fig. 44-3, C). Although the graft tension instantly increased to 69N ± 11N (mean ± standard deviation) (range 53–80N) or 133N ± 14N (range 121–157N) during hammering of the spikes, it settled to 49N ± 1N (range 37–63N) or 100N ± 7N (range 88–107N) at 5 minutes after completing the fixation.
The same experiment on four porcine tibias was performed with a small-sized DSP under the initial tension of 49N, followed by final fixation using a 5.0-mm cancellous screw. Although the graft tension instantly increased to 53N ± 6N (range 48–63N) during hammering of the spikes, it settled to 45N ± 7N (range 37–53N) after completing the fixation (see Fig. 44-4).
Easy, Secure, and Consistent Pullout Anterior Cruciate Ligament Graft Fixation with Double-Spike Plates
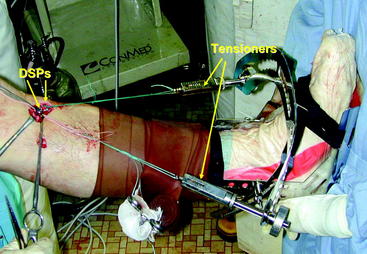
After femoral side fixation is completed, the sutures placed to the graft’s distal end are tied to the top hole of DSP. The tensioning sutures distally connected to the DSP are tied to the tensioners mounted to a metal shell boot that has already been fixed to the tibia with bandage (Fig. 44-5). It is our current choice to apply a total amount of 20N as the graft initial tension: 10N for the anterior two bundles and 10N for the posterior doubled graft in the triple-bundle ACL reconstruction,2 and 20N for the bone–patellar tendon–bone graft in the rectangular tunnel ACL reconstruction.3 After the intended amount of the tension is applied, the knee undergoes passive flexion-extension movement for several times, and the tensioning sutures are retightened by repetitive strong manual pull. After the tension stops to drop following load relaxation, the knee is maintained at 15 to 20 degrees under the tension for an additional 2 minutes. Finally, the graft is fixed with a DSP and cancellous screw (Fig. 44-6). Use of a metal rather than plastic hammer of higher mass makes it possible to gently strike the base spikes into the tibial cortex and to avoid breakage of the cortex by overstriking.

1 Shino K, Mae T, Maeda A, et al. Graft fixation with predetermined tension using a new device, the double spike plate. Arthroscopy. 2002;18:908-911.
2 Shino K, Nakata K, Nakamura N, et al. Anatomic ACL reconstruction using two double-looped hamstring tendon grafts via twin femoral and triple tibial tunnels. Oper Tech Orthop. 2005;15:130-134.
3 Shino K, Nakata K, Nakamura N, et al. Anatomically-oriented ACL reconstruction with a bone-patellar tendon graft via rectangular socket/tunnels: a snug-fit and impingement-free grafting technique. Arthroscopy. 2005;21:1402.e1-1402.e5.






