Chapter 149 Dorsal Thoracic and Lumbar Simple Hook-Rod, Wire, and Wire-Rod Techniques
The first internal fixation device was designed by Harrington in 1947, a period in which the number of patients with poliomyelitis-induced scoliosis was growing, and there was dissatisfaction with the current management of corrective casting. The device was designed to correct scoliotic curvatures and halt progression of cardiopulmonary compromise in affected patients. Initial attempts consisted of screw fixation of facet joints in the corrected position. The results appeared promising, but early beneficial results were short-lived. Facet screw failure led to the development of a hook-and-rod construct, in which hooks were attached to the dorsal elements and held in place with a combination of distraction and compression forces. The clinical results of Harrington’s new system were published in 1962.1–3
The Harrington system offered the first internal fixation device for the correction of scoliotic deformities. The system was quickly adopted by spine surgeons and applied to various conditions, including trauma, neoplastic disease, fixed deformities, and degenerative disorders.2,4,5
The Harrington system, although versatile, was plagued with inherent problems. The system was limited in its design, which allowed for only two points of fixation. Failure at any single hook site led to failure of the entire system.6 However, the system has been modified over the years.
In the early 1970s, Luque was faced with an impoverished community in which postoperative bracing was impossible. From these circumstances arose the concept of segmental spinal instruumentation. The Luque system consisted of straight, L-shaped, or rectangular rods attached to lamina via sublaminar wires.7 The advent of segmental spinal instrumentation addressed the main problem associated with the Harrington system that had only two points of fixation. Initially, sublaminar wires were used to supplement the Harrington system.4–6 This innovation was followed by interspinous wiring techniques, such as Wisconsin wires and Dummond buttons. The original Harrington rod was rigid and difficult to contour, and the rounded caudal rigid tip failed to prevent rotation. This shortcoming led to the development of the square-ended Moe rod, which allowed rod contouring. The three-pointed bending force, which a contured rod provides, was enhanced further by the development of the Edward sleeve.6,8 The Harrington system, although often replaced by newer universal spinal instrumentation systems, can be used to stabilize thoracic and lumbar fractures that result from axial loading and in which the anterior longitudinal ligament is intact.
Harrington Distraction Fixation
Technique
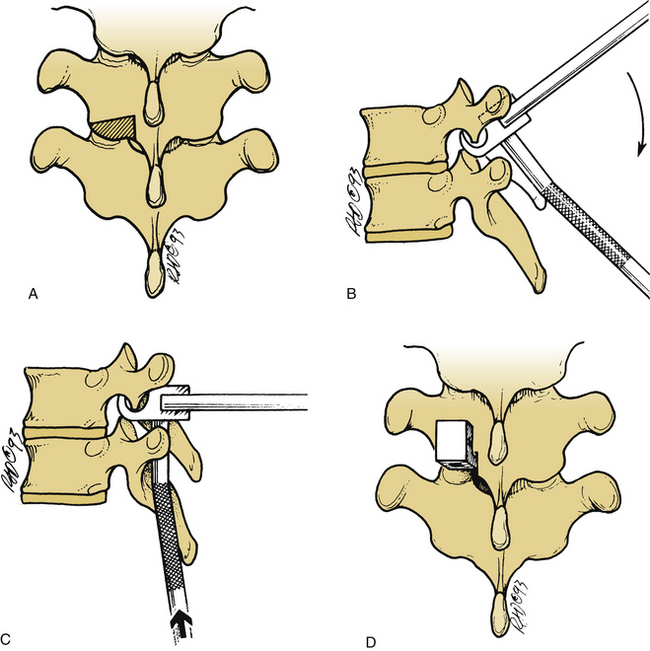
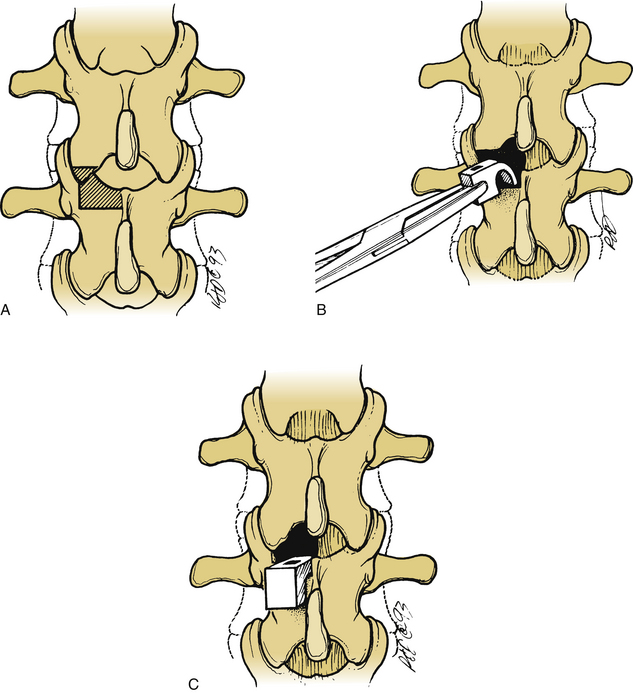
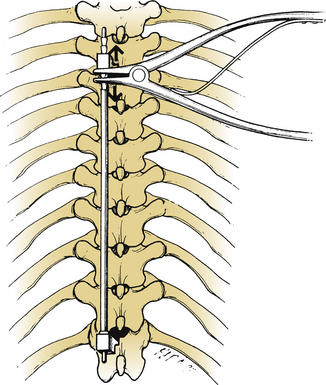
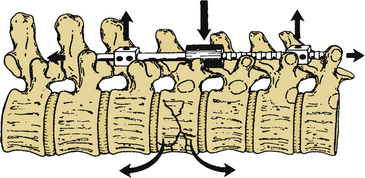
The lamina is conformed to allow seating of the rostral ratcheted hook, typically a no. 1253 hook. A no. 1251 hook can be used as a starter hook, which can be replaced by a no. 1253 hook, a keeled hook, or a bifid no. 1262 hook. The hook is inserted to follow the angle of the facet joint and is gently tapped into position. A well-seated hook should lie orthogonal to the spine (Fig. 149-1). The caudal hook site is generally located two levels below the level of the injury. The interlaminar region at this level is enlarged with a Kerrison rongeur. The ligamentum flavum is excised, and the rostral margin of the lamina is conformed to accommodate the caudal hook, usually a no. 1254 round-hole hook or a no. 1201 square-hole hook (Fig. 149-2). Square-hole caudal hooks are most commonly used because they allow contouring of the rods and minimize rotation. A construct undergoing distraction is depicted in Figure 149-3.
Segmental Fixation
Segmental fixation of the Harrington system has been shown to increase stability.5,6 Segmental fixation can be achieved with either sublaminar wires or cables or interspinous techniques.5,9 When sublaminar fixation is chosen as a means of segmental fixation, use of the cables should be considered because they are stronger and more flexible, and the incidence of neurologic complications may be decreased. Placement of a sublaminar wire or cable can be accomplished by removing the interspinous ligament and performing an interlaminar laminotomy along the midline at each level that is to be instrumented. The ligamentum flavum is removed with a Kerrison rongeur, and the dura mater or epidural fat is visualized. Adequate removal of the ligamentum flavum ensures easy passage of the sublaminar wire or cable.
Interspinous Segmental Instrumentation
Interspinous segmental instrumentation can also be used to supplement the strength of the construct.3 A single hole is made at the base of each spinous process to be instrumented, with a curved awl, a bone tenaculum, or a drill. Beaded Wisconsin wires, with attached Drummond buttons, are passed through the base of the spinous process from each side. Once it is through the base of the spinous process, the beaded Wisconsin wire is passed through the contralateral Drummond button. The Wisconsin wires are pulled tight until the Drummond bottom fits snugly against the base of the spinous process. The beads are then cut. When the rods are in place, the wires are tightly secured to the rods, and the excess wire is removed. The free wire ends are bent to provide a low profile (Fig. 149-4).
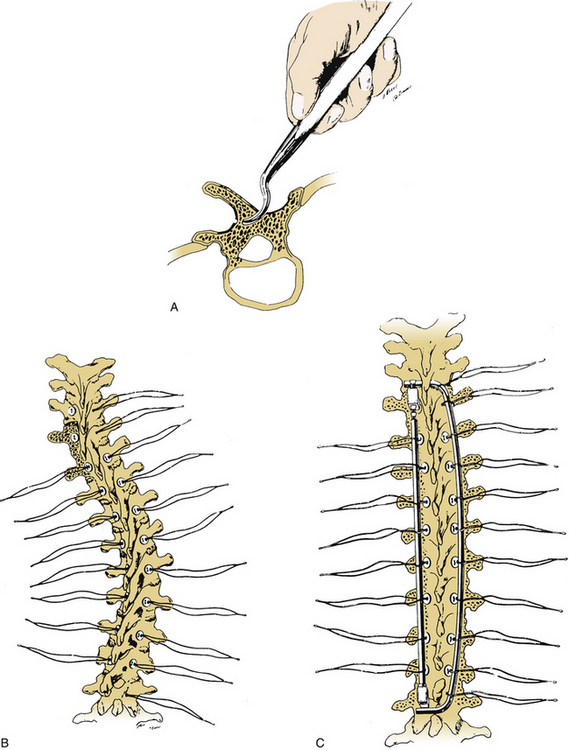
FIGURE 149-4 A–C, Placement of interspinous segmental instrumentation using Wisconsin wires and Drummond buttons.
A square-ended rod is chosen, with an appropriate length of rod that allows one ratchet to be visible beneath the rostral hook. The rod is contoured to maintain normal spinal alignment. Edward sleeves can also be used to enhance reduction of kyphotic deformities.
Rod Sleeves
Rod sleeves are designed to provide reduction of kyphotic deformities.5,6,8 They are made of high-density polyethylene with barium sulfate for radiodensity. Rod sleeves are made in various sizes: small 2-mm sleeves for use in the thoracic spine, medium 4-mm sleeves for use between T12 and L2, and elliptical sleeves for use in the lumbar region (Fig. 149-5). The rod is inserted into the rostral hook, and the rod sleeve is advanced along the rod until it overlies the apex of the deformity. The caudal end is grasped with a hook holder, and the distal rod is held with a rod holder. The deformity is reduced by applying constant ventral pressure. The rod is moved caudally until the distal tip engages the caudal hook, and distraction is applied with the rod distractor.
Luque Segmental Wire Fixation
Luque instrumentation has been largely replaced by universal spinal instrumentation. Although the Luque system offers good stability against rotational and transitional forces, it provides less resistance to flexion-extension and little or no resistance to axial loading. The Luque system may still be used to treat slice fracture, in which the middle column fails because of shearing forces. It may also be useful in cases in which long fixation is required for correction of paralytic scoliotic deformities or in traumatic or neoplastic lesions that lead to flexion-compression fractures. The Luque system may be beneficial in patients with poor bone quality who require spinal stabilization.4–7
Technique
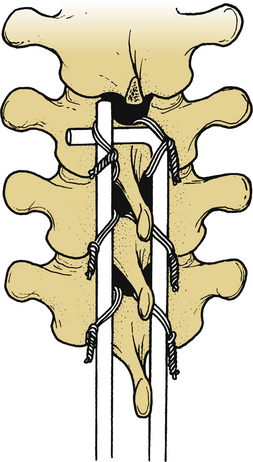
Luque rectangles confer rotational and migrational stability to the construct. Sublaminar wires or cables are secured to the appropriately contoured Luque rod or rectangle (Figs. 149-6 to 149-8). The short limb of the L-shaped Luque rod should be secured beneath the long limb of the contralateral Luque L-rod (Fig. 149-9). Interspinous wiring techniques described for Harrington instrumentation can also be used with Luque L-rods. The interspinous wiring technique, although safer to perform than placement of sublaminar wires or cables, creates a weaker construct; also, it cannot be used with Luque rectangles, because the Luque rectangle cannot be adequately approximated to the spinous process.
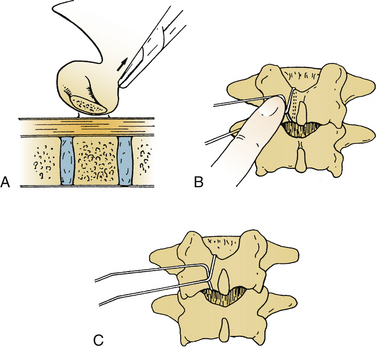
FIGURE 149-6 A, Placement of sublaminar wires via midline laminotomy. B and C, Crimping prevents spinal cord encroachment.
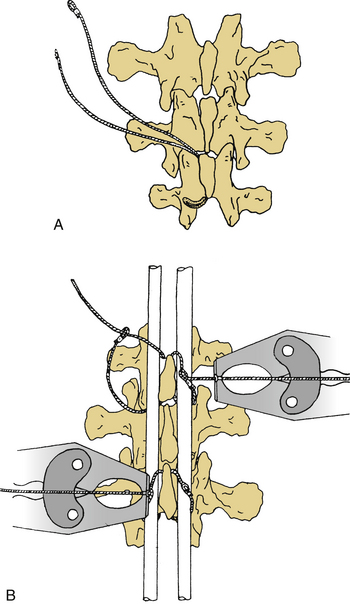
FIGURE 149-7 A and B, Placement of sublaminar multistrand cable via a midline laminotomy.
(From Songer MN, Spencer DL, Meter PR, et al: The use of sublaminar cables to replace Luque wires. Spine [Phila Pa 1976] 16[suppl]:418–421, 1991.)
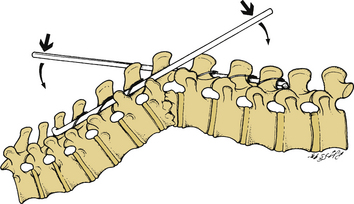
Although originally designed for neutral fixation of the spine, the Luque system can be used to reduce kyphotic deformities. In this situation, the rostral end of one Luque L-rod and the caudal end of the contralateral Luque L-rod are attached and can be used to reduce kyphotic deformities. In this situation, the rostral end of one Luque L-rod is attached via sublaminar or interspinous wires or cables. The free ends of the rods are used as levers to reduce the existing kyphotic deformity (Fig. 149-10). After reduction, the wires or cables are sequentially tightened, ensuring lasting reduction. Excess wire or cable is cut, and the free ends are contoured to allow a low-profile construct. Closure is performed as described for Harrington instrumentation; postoperative care is also identical to Harrington instrumentation.
Scott Wiring Technique
Few indications remain for the use of spinal wiring in the lumbar spine. One indication is symptomatic lumbar spondylolysis with or without grade I spondylolisthesis. This wiring technique for direct repair of spondylolysis was described by Nicol and Scott10 and later modified by Johnson and Thompson.11 The Scott wiring technique consists of wiring the transverse process to the spinous process.
Technique
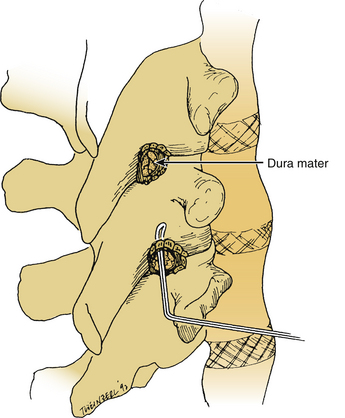
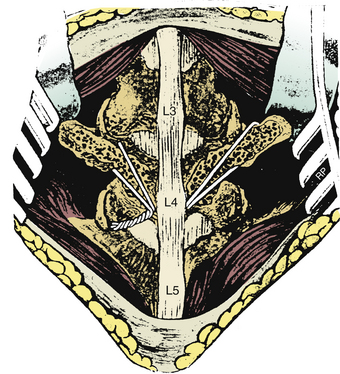
The patient is positioned prone on the operating table. A subperiosteal dissection is performed and carried laterally, extending over the transverse processes. Bilateral pars interarticularis fractures are readily identified by the increased mobility of the affected segment. The defect is freed of any overlying or intervening fibrous tissue. The bony margins of the defect, base of the transverse process, and adjacent lamina are decorticated. Originally, a wire was passed around the transverse process bilaterally, and the free wire was passed beneath the subadjacent spinous process and was secured (Fig. 149-11). This technique was later modified to minimize the incidence of nerve root injury. With the modified technique, a hole is drilled at the base of the transverse process and the spinous process. A wire or, alternatively, a multistrand cable is passed through the hole at the base of the transverse process and then through the drill hole at the base of the spinous process, forming a figure-8 configuration. Autologous corticocancellous strips are placed over the pars interarticularis defect and decorticated transverse process and lamina. The bone grafts are secured into position by tightening the wire or cable.
Drummond D.S. Harrington instrumentation with spinous process wiring for idiopathic scoliosis. Orthop Clin North Am. 1998;19:281-289.
Harrington P.R. Treatment of scoliosis: correction and internal fixation by spinal instrumentation. J Bone Joint Surg [Am]. 1962;44:591-610.
Harrington P.R. Technical details in relation to the successful use of instrumentation in scoliosis. Orthop Clin North Am. 1972;3:49-67.
Harrington P.R. The history and development of Harrington instrumentation. Clin Orthop Relat Res. 1973;93:110-112.
Luque E.R. The anatomic basis and development of segmental spinal instrumentation. Spine. 1982;7:256-259.
McCormick P.C. Dorsal distraction and neutral segmental fixation of the thoracic and lumbar spine: Harrington and Luque techniques. In: Benzel E.C., editor. Spinal instrumentation. Park Ridge, IL: Publications Committee of the North American Association of Neurological Surgeons; 1994:125-141.
1. Harrington P.R. Treatment of scoliosis: correction and internal fixation by spinal instrumentation. J Bone Joint Surg [Am]. 1962;44:591-610.
2. Harrington P.R. Technical details in relation to the successful use of instrumentation in scoliosis. Orthop Clin North Am. 1972;3:49-67.
3. Harrington P.R. The history and development of Harrington instrumentation. Clin Orthop Relat Res. 1973;93:110-112.
4. Stillerman C.B., Gruen J.P., Roy R. Thoracic and lumbar fusion: techniques for posterior stabilization. In: Menezes A., Sonntag V., editors. Principles of spinal surgery. New York: McGraw-Hill; 1996:1199-1223.
5. Richardson W.J., Hardaker W.T.Jr. Management of thoracic and lumbar spinal instability. In: Wilkins R., Renegachary S., editors. Neurosurgery. New York: McGraw-Hill, 1996. pp 2298–3001
6. McCormick P.C. Dorsal distraction and neutral segmental fixation of the thoracic and lumbar spine: Harrington and Luque techniques. In: Benzel E.C., editor. Spinal instrumentation. Park Ridge, IL: Publications Committee of the North American Association of Neurological Surgeons; 1994:125-141.
7. Luque E.R. The anatomic basis and development of segmental spinal instrumentation. Spine. 1982;7:256-259.
8. Edwards C.C., Levine A.M. Early rod-sleeve stabilization of the injured thoracic and lumbar spine. Orthop Clin North Am. 1986;17:121-145.
9. Drummond D.S. Harrington instrumentation with spinous process wiring for idiopathic scoliosis. Orthop Clin North Am. 1998;19:281-289.
10. Nicol R.O., Scott J.H.S. Lytic spondylolysis repair by wiring. Spine (Phila Pa 1976). 1986;11:1027-1030.
11. Johnson G.V., Thompson A.G. The Scott wiring technique for direct repair of lumbar spondylosis. J Bone Joint Surg [Br]. 1992;74:426-430.






