[level-membership-for-orthopaedics-category]
CHAPTER 11 Dorsal Double Plating and Combined Palmar and Dorsal Plating for Distal Radius Fractures
If operative therapy is indicated to treat a distal radius fracture, the majority of cases can be treated by palmar plating. Extra- and intra-articular fractures can be managed by this method, which is straightforward, by using a simple surgical approach. The result is low morbidity and overall good clinical outcome, even in very osteoporotic bone. However, there is a subset of intra-articular fractures that require a dorsal approach to achieve anatomical reduction of the radiocarpal joint surface and direct fixation of specific key fragments. Moreover, a dorsal approach is always combined with a limited dorsal arthrotomy that allows for direct visualization of the radiocarpal joint surface and—importantly—the proximal carpal row, so as to rule out associated ligament tears. In a series of 100 consecutive distal radius cases that were plated at our institution, 75% were treated by using a palmar plate, 20% by dorsal double plating, and 5% by combined palmar and dorsal plating.
Biomechanical Background
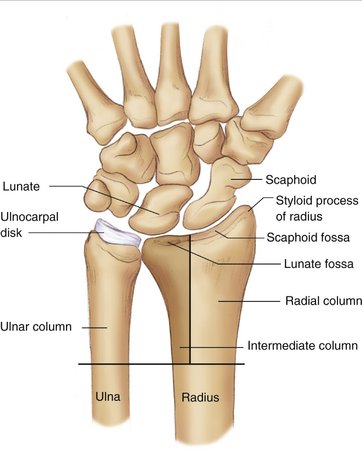
The concept of plating for distal radius fractures is based on the three-column model.1 The model says simply that the distal forearm consists of three columns (Fig. 11-1). The radial column is composed of the radial styloid process and the scaphoid facet; the intermediate column is formed by the lunate facet and the sigmoid notch; and the distal ulna is the ulnar column together with the triangular fibrocartilage and the ulnar part of the lunate facet and sigmoid notch. In extension fractures of the distal radius, the distal epiphyseal fragment is displaced toward the dorsal and radial directions. Separate buttressing of the intermediate and the radial columns by two individual plates to prevent dorsal (intermediate column plate) and radial (radial column plate) dislocation has been shown to be a stable mechanical construct with greater stiffness than a conventional 3.5-mm T-plate or a Pi plate (2.7 mm) in cadaver wrists that show a simulated dorsal metaphyseal defect.2
In vivo analysis of force transmission across the radioulnocarpal joint has revealed data that are consistent with the three-column model. Only a small amount of force is transmitted through the radial column. The radial column serves more as a radial osseous buttress and an insertion for the radiocarpal ligaments. In intra-articular fractures, the radial styloid most often is one single bone fragment without comminution or impaction of the joint surface. The greatest force is transmitted across the intermediate and the ulnar columns. In intra-articular fractures, the key articular fragments and impaction zones are found at the level of the intermediate column due to these compressive forces. The intermediate column, therefore, is the key to the radiocarpal joint. The ulnar column also transmits an amount of force that is comparable to that of the intermediate column. It is therefore very sensitive to radial shortening (relative ulnar overlength), which produces painful ulnar impaction. Thus, reconstruction of radial length is an important prognostic outcome factor. Moreover, the ulnar column is the pivot that serves as the center of rotation of the hand and carpus around the forearm, with a complex soft tissue stabilizing construct (TFC, ulnocarpal ligaments, ECU).3
Three-Step Approach to High-Energy Intra-articular Distal Radial Fractures
Analysis of the individual fracture personality on the basis of the initial emergency room radiograph when the fracture has been unreduced is difficult, and a clear treatment strategy often cannot be developed based on the initial imaging. So for complex, high-energy injuries, it may be advisable to perform a closed reduction and a joint-bridging external fixator as a first measure in the emergency situation (step 1). The advantages are as follows: closed reduction and external fixation are easy to perform, even by inexperienced staff; skin and soft tissue lesions can calm down over the coming days; and median nerve neuropathy usually resolves after preliminary closed reduction. A computed tomography (CT) scan of the wrist in traction allows accurate analysis of the fracture personality and provides more information about a definitive treatment strategy than does a CT scan of an unreduced fracture because some fragments are reduced under ligamentotaxis (step 2). When the swelling has subsided, usually after 3 to 7 days, the definitive osteosynthesis, according to the preoperative planning based on conventional radiographs and CT scans, can be performed (step 3). An external fixator in place is then a helpful intraoperative reduction tool.4
Analysis of the Fracture Personality
A thorough analysis of the fracture personality is the prerequisite for developing an adequate treatment strategy. Fernandez5 has proposed a pathomechanical classification that allows identification of the principal forces involved in the individual injury: bending, shear, avulsion, and compression. Categorizing the fracture into these groups helps to define the major treatment strategy: bending responds to ligamentotaxis; shear requires buttressing; avulsion needs reinsertion of ligaments; and compression affords individual reconstruction of the columns, often with formal revision of the intermediate column (“the key to the radiocarpal joint”).
In high-energy intra-articular fractures, a preoperative CT scan in traction should be indicated deliberately. If a three-step approach is performed, as delineated earlier, a CT scan with an external fixator in place is the preferred investigation. In our experience and in accordance with Melone,6 there are five key elements that should be analyzed in the CT image:
All five of these key elements should be identified and considered when planning treatment.
Dorsal Double Plating
The indications for dorsal double plating are any situations in which a dorsal arthrotomy is warranted in order to revise the radiocarpal joint surface and the proximal carpal row. We do not perform palmar arthrotomies so as to avoid provoking carpal ligament instability. A dorsal arthrotomy may be indicated to reconstruct the articular surface at the level of the intermediate column, especially when impacted articular fragments are present. Such fragments may require direct manipulation. In a dorsal arthrotomy, disruption of interosseous ligaments (especially the scapholunate) can be ruled out or confirmed and be treated immediately at the time of fixation of the distal radius fracture. Furthermore, a dorsal approach is preferred when a displaced dorsoulnar fragment is present. This fragment, which is a key fragment of the radiocarpal articular surface and the sigmoid notch, can then be reduced anatomically and fixed specifically with a separate intermediate column plate. In some cases of corrective osteotomies, a dorsal approach may also be preferred.7
Indications
Approach and Operative Technique
Anesthesia and Positioning
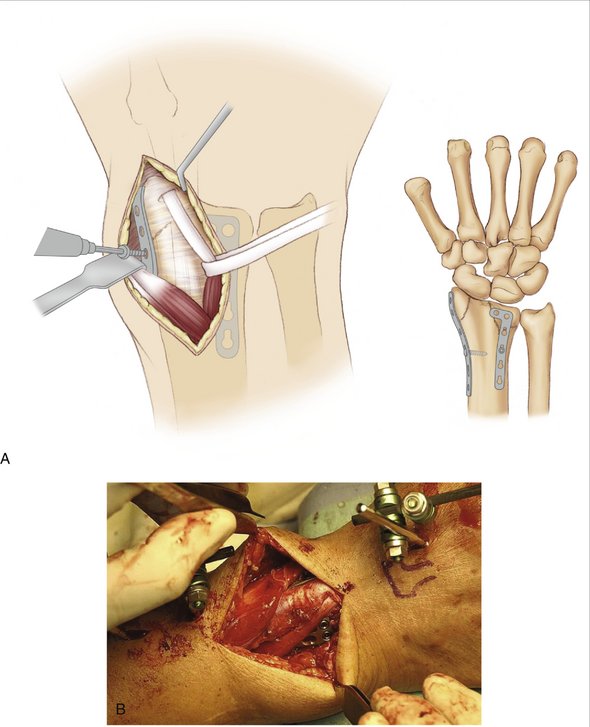
FIGURE 11-4 Correction of the reduction and of the positions of the plates can now be carried out without any problem. The osteosynthesis is then completed by inserting a standard screw into each of the most proximal plate holes. This prevents any further slipping of the plate. Locking head screws are then inserted into the distal plate holes. Two screws are sufficient in the radial plate. The most distal screw is usually very short, the proximal screw is long; it also supports the radiocarpal joint. The transverse plate arm in the area of the dorsoulnar plate is usually fixed with fixed-angle screws. This supports the reconstructed articular surface subchondrally. It must be ensured that the screws do not protrude into the joint. The threaded drill sleeve for the fixed-angle, locking screws must be screwed very carefully onto the plate. This is the only way to ensure that the screws sink completely into the plate and are securely anchored in the plate-hole threads. Check using the image intensifier. If the reconstruction is satisfactory and the implants are in the correct positions, the fixator is loosened and the wrist is passed through a full range of motion under image intensification in order to determine if the fixation is stable enough to allow early wrist motion.
(From Rikli DA, Businger A, Babst R: Dorsal double-plate fixation of the distal radius. Oper Orthop Traumatol 2005; 6:624-640. Used with permission.)
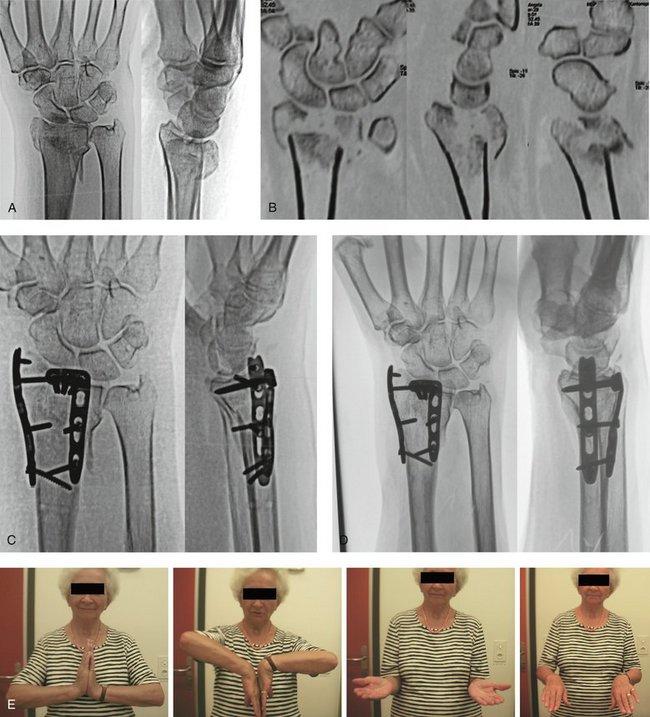
FIGURE 11-5 A Comminuted Intraarticular Distal Radius Fracture of a 75-Year-Old Patient. A, Anteroposterior and lateral views. B, CT-scan shows articular comminution, a displaced dorsoulnar fragment and metaphyseal bone defect. C, Postoperative x-rays after dorsal double plating. No bone graft, early rehabilitation. D, 1 year postoperatively. E, Clinical result 1 year postoperatively.
Results
We analyzed a series of 25 consecutive patients with intra-articular distal radius fractures treated with dorsal double plating (Table 11-1). The minimum follow-up was 12 months. There were 14 men and 11 women, for an average age of 52 years. No bone grafts or bone substitutes were used. All fractures united in an anatomical position. The average Disabilities of the Arm, Shoulder, and Hand (DASH) score was 7.2 (0 to 56) and the patient-rated wrist evaluation (PRWE) score was 8 (0 to 31). There was no significant loss of strength compared with the contralateral side as measured by a JAMAR dynamometer. The range of motion for flexion and extension was between 100 degrees and 160 degrees; for pronation and supination, it was between 160 degrees and 180 degrees. One patient showed irritation of the extensor pollicis longus tendon due to adhesions at the level of the musculotendinous junction, but no extensor tendon ruptures occurred. There was one case of mild algodystrophy that resolved completely. In six patients the implants were removed.7
| Patients | 25 |
| Men/women | 14/11 |
| Age | 52 (17-83) |
| A3 (early correction) | 2 |
| C1-C3 | 23 |
| Dominant hand | 17 |
| Cancellous bone graft | 0 |
| Functional rehabilitation | 25 |
| Stewart score: very good | 25 |
| DASH score (points) | 7.2 (0-56) |
| PRWE score (points) | 8.0 (0-31) |
| Extensor tendon irritation | 1 |
| Reflex sympathetic dystrophy | 1 |
| Implant removal | 6 |
DASH, disability of arm, shoulder, and hand; PRWE, patient-related wrist evaluation.
Combined Palmar and Dorsal Plating
The indications for combined palmar and dorsal plating are as follows:
Approach and Operative Technique
If the wrist is not in a joint-bridging external fixator (a three-step approach to high-energy injuries), an external fixator is placed first to preliminarily reduce the fracture by putting the wrist under traction. This measure is very helpful and is strongly recommended. Other traction devices may be used instead. It is preferable to start with the palmar approach, a modified Henry’s approach between the tendon of the flexor carpi radialis and the radial artery. The palmar cortical buttress is reconstructed, and a hyperextended palmar articular fragment is reduced. This palmar-ulnar fragment is then fixed with a single 2.4-mm locking plate. The articular fragment is held with one or two short screws so as to avoid interfering with any dorsoulnar fragment that may remain in an imperfect position. The radial column is buttressed by using the same palmar approach and a radial column plate (2.4-mm locking plate). As an alternative, both the palmar-ulnar fragment and the radial column can be stabilized by a single palmar T-plate (2.4-mm locking plate). That way, a limited dorsal approach has been established. Only the intermediate column is visualized through the third extensor tendon compartment (similar to dorsal double plating). It is not necessary to approach the radial column because this column is already controlled from the palmar access (Figs. 11-6 and 11-7). The dorsoulnar fragment and any centrally impacted fragment are visualized, and a limited transverse arthrotomy is performed. This allows for direct inspection of the proximal carpal row (SL tear) and the radiocarpal joint surface at the level of the intermediate column. The fragments are then reduced and fixed with a separate 2.4-mm locking plate. Then the palmar fixation is completed. Any of these steps may be controlled by using intraoperative fluoroscopy as needed. At the completion of fixation, the external fixator is opened, and the wrist is driven through flexion-extension, radial-ulnar duction, and pronation-supination to demonstrate the stability of the construct. The wounds are then closed in layers and the external fixator pins are removed. A sterile dressing and a dorsal or palmar plaster slap is applied.

FIGURE 11-6 A Comminuted Distal Radius Fracture of a 38-Year-Old Worker. A, Anteroposterior and lateral views. B, CT scan in traction (external fixator) shows articular involvement, the intermediate column fragment is flipped 90 degrees in two planes. C, Immediately postop. An associated complete SL tear was repaired, temporary carpal transfixation, external fixator left in place for 8 weeks to protect ligament repair. D, 1 year postoperatively, slight DISI and diastasis of DRUJ. E, Clinical result 1 year postoperatively; slight pain, back to work.
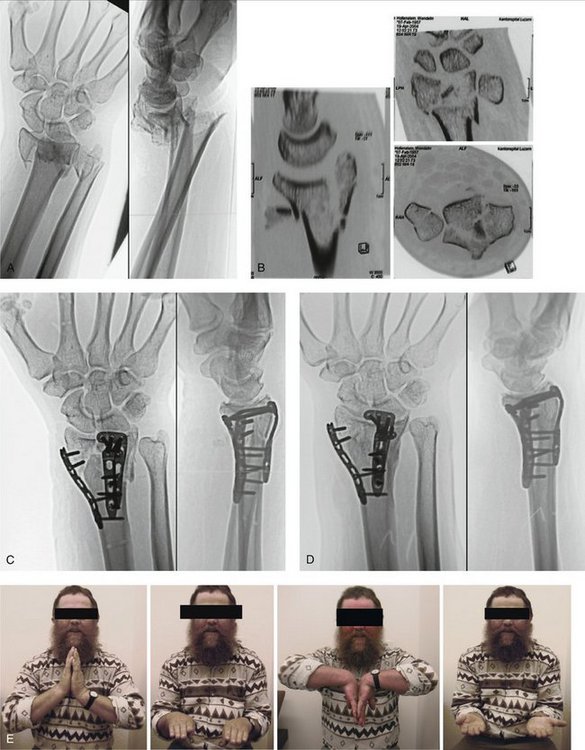
FIGURE 11-7 A Comminuted Intra-articular Distal Radius Fracture of a 40-Year-Old Farmer. A, Anteroposterior and lateral views. B, CT scan in traction (external fixator) shows impacted articular fragment, loss of palmar cortex and displaced dorsoulnar fragment. C, Immediately postop. D, Radiograph taken 1 year postoperatively. E, Clinical result 1 year postoperatively; pain-free, back to heavy labor.
Results
We analyzed the results of a consecutive series of 10 patients following combined palmar and dorsal plating for complex intra-articular distal radial fractures (Table 11-2). The average age was 47 years, and eight patients were heavy laborers. The minimum follow-up was 12 months. All had early active rehabilitation. All fractures united with no infectious complications. The range of motion in relation to the unaffected side was 80% for flexion, 95% for extension, 97% for pronation, and 94% for supination. Two patients had unsatisfactory clinical results and did not resume work; one had algodystrophy (associated SL tear, repaired), and one had a concomitant fracture-dislocation of the ipsilateral elbow. The DASH and PRWE scores of these two patients were 91 and 132, and 62 and 120, respectively. Eight patients returned to premorbid heavy labor with a DASH between 0 and 12.5 and a PRWE of 0 and 33. This latter group achieved grip strength of between 72% and 99% of the contralateral side.8
| Patients | 10 |
| Men/women | 10/0 |
| Heavy labor | 8 |
| Age | 47 y (av.) |
| Classification | C3 |
| Bone graft | 0 |
| Functional rehabilitation | 10 |
| Resume work | 8 |
| Unsatisfactory | 2 |
| DASH score (pts) (Back to work) | 0-12.5 |
| PRWE score (pts) (Back to work) | 0-33 |
| Grip strength (% of contralat.) (Back to work) | 72-99% |
| DASH score (pts) (Unsatisfactory) | 91,132 |
| PRWE score (pts) (Unsatisfactory) | 62,120 |
| Reflex sympathetic dystrophy | 1 |
| DASH, disability of arm, shoulder, and hand; PRWE, patient-related wrist evaluation. |
1. Rikli D, Regazzoni P, Babst R. Die dorsale Doppelplattenosteosynthese am distalen Radius: ein biomechanisches Konzept und dessen klinische Realisation. Zentralbl Chir. 2003;128:1003-1007.
2. Peine R, Rikli D, Hoffmann R, et al. Comparison of three different plating techniques for the dorsum of the distal radius. J Hand Surg [Am]. 2000;25:29-33.
3. Rikli DA, Honigmann P, Babst R, et al. Intra-articular pressure measurement in the radioulnocarpal joint using a novel sensor: in vitro and in vivo results. J Hand Surg [Am]. 2007;32:67-75.
4. Rikli DA, Regazzoni P. The double plating technique for distal radius fractures. Tech Hand Up Extrem Surg. 2000;4:107-114.
5. Fernandez DL. Distal radius fracture: the rationale of a classification. Chir Main. 2001;20:411-425.
6. Melone CP. Open treatment for displaced articular fractures of the distal radius. Clin Orthop. 1984;202:103-111.
7. Rikli DA, Businger A, Babst R. Dorsal double-plate fixation of the distal radius. Oper Orthop Traumatol. 2005;17:624-640.
8. Rikli D, Droeser R, Babst R. Combined dorsal and palmar plating for complex intraarticular distal radial fractures. Lugano: Vortrag Schweizerischer Chirurgenkongress; June 2006.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER 11 Dorsal Double Plating and Combined Palmar and Dorsal Plating for Distal Radius Fractures
If operative therapy is indicated to treat a distal radius fracture, the majority of cases can be treated by palmar plating. Extra- and intra-articular fractures can be managed by this method, which is straightforward, by using a simple surgical approach. The result is low morbidity and overall good clinical outcome, even in very osteoporotic bone. However, there is a subset of intra-articular fractures that require a dorsal approach to achieve anatomical reduction of the radiocarpal joint surface and direct fixation of specific key fragments. Moreover, a dorsal approach is always combined with a limited dorsal arthrotomy that allows for direct visualization of the radiocarpal joint surface and—importantly—the proximal carpal row, so as to rule out associated ligament tears. In a series of 100 consecutive distal radius cases that were plated at our institution, 75% were treated by using a palmar plate, 20% by dorsal double plating, and 5% by combined palmar and dorsal plating.
Biomechanical Background
The concept of plating for distal radius fractures is based on the three-column model.1 The model says simply that the distal forearm consists of three columns (Fig. 11-1). The radial column is composed of the radial styloid process and the scaphoid facet; the intermediate column is formed by the lunate facet and the sigmoid notch; and the distal ulna is the ulnar column together with the triangular fibrocartilage and the ulnar part of the lunate facet and sigmoid notch. In extension fractures of the distal radius, the distal epiphyseal fragment is displaced toward the dorsal and radial directions. Separate buttressing of the intermediate and the radial columns by two individual plates to prevent dorsal (intermediate column plate) and radial (radial column plate) dislocation has been shown to be a stable mechanical construct with greater stiffness than a conventional 3.5-mm T-plate or a Pi plate (2.7 mm) in cadaver wrists that show a simulated dorsal metaphyseal defect.2
In vivo analysis of force transmission across the radioulnocarpal joint has revealed data that are consistent with the three-column model. Only a small amount of force is transmitted through the radial column. The radial column serves more as a radial osseous buttress and an insertion for the radiocarpal ligaments. In intra-articular fractures, the radial styloid most often is one single bone fragment without comminution or impaction of the joint surface. The greatest force is transmitted across the intermediate and the ulnar columns. In intra-articular fractures, the key articular fragments and impaction zones are found at the level of the intermediate column due to these compressive forces. The intermediate column, therefore, is the key to the radiocarpal joint. The ulnar column also transmits an amount of force that is comparable to that of the intermediate column. It is therefore very sensitive to radial shortening (relative ulnar overlength), which produces painful ulnar impaction. Thus, reconstruction of radial length is an important prognostic outcome factor. Moreover, the ulnar column is the pivot that serves as the center of rotation of the hand and carpus around the forearm, with a complex soft tissue stabilizing construct (TFC, ulnocarpal ligaments, ECU).3
Three-Step Approach to High-Energy Intra-articular Distal Radial Fractures
Analysis of the individual fracture personality on the basis of the initial emergency room radiograph when the fracture has been unreduced is difficult, and a clear treatment strategy often cannot be developed based on the initial imaging. So for complex, high-energy injuries, it may be advisable to perform a closed reduction and a joint-bridging external fixator as a first measure in the emergency situation (step 1). The advantages are as follows: closed reduction and external fixation are easy to perform, even by inexperienced staff; skin and soft tissue lesions can calm down over the coming days; and median nerve neuropathy usually resolves after preliminary closed reduction. A computed tomography (CT) scan of the wrist in traction allows accurate analysis of the fracture personality and provides more information about a definitive treatment strategy than does a CT scan of an unreduced fracture because some fragments are reduced under ligamentotaxis (step 2). When the swelling has subsided, usually after 3 to 7 days, the definitive osteosynthesis, according to the preoperative planning based on conventional radiographs and CT scans, can be performed (step 3). An external fixator in place is then a helpful intraoperative reduction tool.4
Analysis of the Fracture Personality
A thorough analysis of the fracture personality is the prerequisite for developing an adequate treatment strategy. Fernandez5 has proposed a pathomechanical classification that allows identification of the principal forces involved in the individual injury: bending, shear, avulsion, and compression. Categorizing the fracture into these groups helps to define the major treatment strategy: bending responds to ligamentotaxis; shear requires buttressing; avulsion needs reinsertion of ligaments; and compression affords individual reconstruction of the columns, often with formal revision of the intermediate column (“the key to the radiocarpal joint”).
In high-energy intra-articular fractures, a preoperative CT scan in traction should be indicated deliberately. If a three-step approach is performed, as delineated earlier, a CT scan with an external fixator in place is the preferred investigation. In our experience and in accordance with Melone,6 there are five key elements that should be analyzed in the CT image:
All five of these key elements should be identified and considered when planning treatment.
Dorsal Double Plating
The indications for dorsal double plating are any situations in which a dorsal arthrotomy is warranted in order to revise the radiocarpal joint surface and the proximal carpal row. We do not perform palmar arthrotomies so as to avoid provoking carpal ligament instability. A dorsal arthrotomy may be indicated to reconstruct the articular surface at the level of the intermediate column, especially when impacted articular fragments are present. Such fragments may require direct manipulation. In a dorsal arthrotomy, disruption of interosseous ligaments (especially the scapholunate) can be ruled out or confirmed and be treated immediately at the time of fixation of the distal radius fracture. Furthermore, a dorsal approach is preferred when a displaced dorsoulnar fragment is present. This fragment, which is a key fragment of the radiocarpal articular surface and the sigmoid notch, can then be reduced anatomically and fixed specifically with a separate intermediate column plate. In some cases of corrective osteotomies, a dorsal approach may also be preferred.7
