[level-membership-for-pediatrics-category]
101 Disorders of the Nervous System
Etiology and Pathogenesis
Intraventricular Hemorrhage
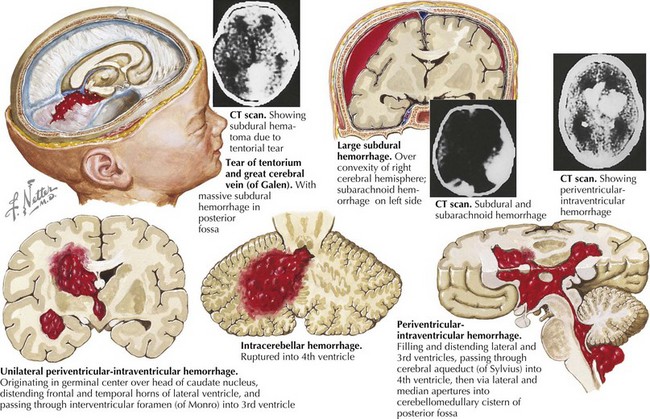
Although the premature cerebrovasculature has reasonable capacity for autoregulation within the normal range of blood pressure, this mechanism quickly becomes inadequate as blood pressures fluctuate outside the norm, predisposing the brain to ischemic injury during times of hypotension and hemorrhagic injury during times of hypertension. The periventricular germinal matrix of the premature brain is at high risk for hemorrhagic injury because of the presence of a rich but relatively immature capillary network. This region is particularly critical because it harbors the neural stem and progenitor cell population that provides precursors necessary for future myelination and development of the brain. Figure 101-1 demonstrates patterns of hemorrhagic injury that can occur in both premature and term infants.
Neonatal Seizures
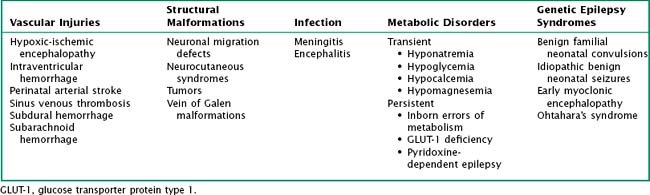
Neonatal seizures are often a manifestation of underlying neurologic disease or injury (Table 101-1). In each case, the metabolic or structural abnormalities cause disorganized electrical activity that can lead to epileptogenic foci.
Neonatal Hypotonia
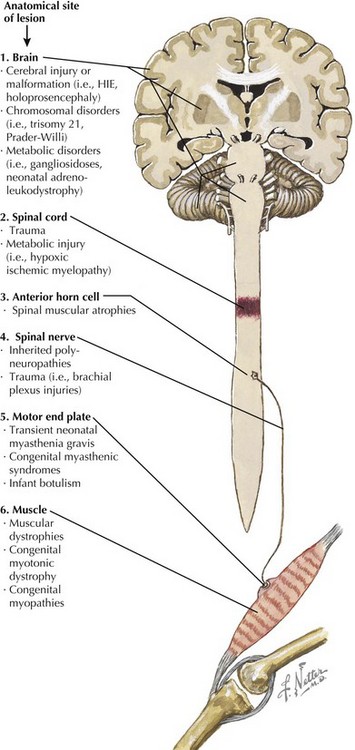
Hypotonia is a common sign of neurologic disease in newborns that can be caused by dysfunction anywhere along the neuromuscular axis. These may arise from genetic defects causing protein dysfunction in either nerve or muscle cells, loss of cerebral regulation of tone secondary to global central nervous system (CNS) dysfunction as in many chromosomal disorders or injuries, or disturbed signal transmission at the neuromuscular junction. The more common causes of hypotonia can be organized by the location of the primary defect (Figure 101-2).
Clinical Presentation
Neonatal Seizures
Neonatal seizures have a variety of manifestations and a variety of normal mimics (Box 101-1). Clonic seizures can occur either focally or multifocally and are repetitive high-amplitude, low-frequency jerking movements. Tonic seizures are constant stiffening of a portion of the body and may be focal or generalized. Myoclonic seizures include sudden extension or flexion of part of the body. Subtle seizures encompass other small abnormal movements that do not fit into the previously listed seizure types, including eye deviation, lip smacking, and tongue thrusting, among others. Subtle seizures and generalized tonic seizures often do not have electroencephalographic (EEG) correlates and are thought to emanate from deeper subcortical brain regions, a theory supported by animal studies.
Neonatal Hypotonia
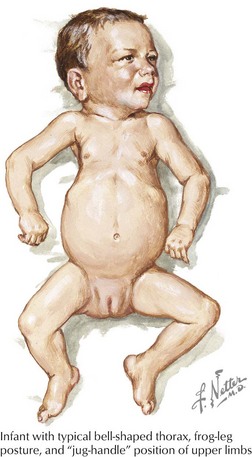
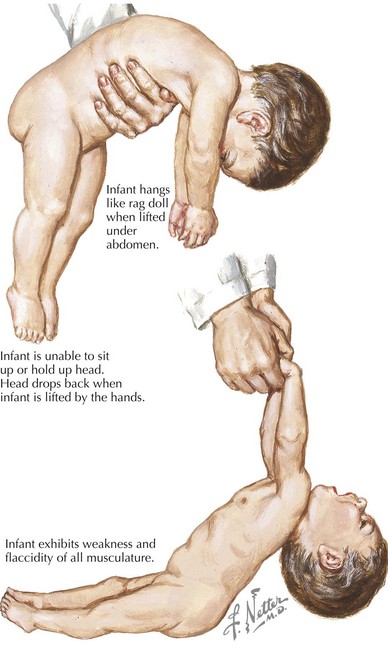
Hypotonia is a cardinal sign associated with many neurologic abnormalities that is characterized by decreased resistance of muscle to passive stretch. Hypotonia presenting in the newborn period has a similar clinical appearance regardless of where along the neuromuscular axis the disease originates. Figure 101-3 shows the characteristic appearance of hypotonic infants. These infants often appear in a frog leg posture with hips abducted and knees flexed when lying supine. Spontaneous movements are decreased compared with their healthy counterparts. Useful physical examination maneuvers to test for hypotonia are traction and prone suspension (Figure 101-4). With traction, a healthy full-term infant should demonstrate flexion at the shoulders and elbows and should be able to slightly flex the neck to keep the head in line with the body as it is brought up. Hypotonic infants show no flexion of the upper extremities, and their head fall to full extension as they are lifted. Similarly, in prone suspension, a healthy infant should show flexion of the extremities and some neck extension in an effort to maintain a horizontal position. Hypotonic infants lie draped over the examiner’s hand.
Evaluation and Management
Neurologic Assessment
Management
Neonatal Seizures
Treatment of neonatal seizures should always focus on correction of the underlying etiology if possible. Transient metabolic disturbances should be addressed specifically. In the absence of such abnormalities, phenobarbital continues to be the mainstay of treatment for neonatal seizures by both neonatologists and neurologists. Second-line agents include phenytoin (or its preferred precursor fosphenytoin) and benzodiazepines, with lorazepam being the most common medication chosen from the latter class. Typical doses are listed in Table 101-2. The most significant risks associated with these drugs are sedation, respiratory depression, and hypotension, and neonates should be monitored closely during initiation these therapies. Clearance of these drugs from the neonatal system is notoriously variable, and infants must be closely monitored for signs of toxicity with clinical observation and drug levels.
Table 101-2 Intravenous Dosages of Common Antiepileptics in Neonates
| Loading Dose | Maintenance Dose | |
|---|---|---|
| Phenobarbital | 20 mg/kg | 3–4 mg/kg/day divided BID |
| Fosphenytoin | 20 mg/kg | 3–4 mg/kg/day divided BID |
| Lorazepam | 0.05 mg/kg | repeated loading as needed |
BID, twice a day.
Aranda JV, Thomas R. Systematic review: intravenous Ibuprofen in preterm newborns. Semin Perinatol. 2006;30(3):114-120.
Booth D, Evans DJ: Anticonvulsants for neonates with seizures. Cochrane Database Syst Rev (4):CD004218. 2004.
Fenichel GM. Clinical Pediatric Neurology—A Signs and Symptoms Approach, ed 5. Philadelphia: Elsevier; 2005.
Glass HC, Glidden D, Jeremy RJ, et al. Clinical neonatal seizures are independently associated with outcome in infants at risk for hypoxic-ischemic brain injury. J Pediatr. 2009;155(3):318-323.
Jacobs S, Hunt R, Tarnow-Mordi W, et al: Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev (4):CD003311, 2007.
Painter MJ, Scher MS, Stein AD, et al. Phenobarbital compared with phenytoin for the treatment of neonatal seizures. N Engl J Med. 1999;341(7):485-489.
Schmidt B, Davis P, Moddemann D, et al. Long-term effects of indomethacin prophylaxis in extremely-low-birth-weight infants. N Engl J Med. 2001;344(26):1966-1972.
Volpe JJL. Neurology of the Newborn, ed 5. Philadelphia: Elsevier Saunders; 2008.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
101 Disorders of the Nervous System
Etiology and Pathogenesis
Intraventricular Hemorrhage
Although the premature cerebrovasculature has reasonable capacity for autoregulation within the normal range of blood pressure, this mechanism quickly becomes inadequate as blood pressures fluctuate outside the norm, predisposing the brain to ischemic injury during times of hypotension and hemorrhagic injury during times of hypertension. The periventricular germinal matrix of the premature brain is at high risk for hemorrhagic injury because of the presence of a rich but relatively immature capillary network. This region is particularly critical because it harbors the neural stem and progenitor cell population that provides precursors necessary for future myelination and development of the brain. Figure 101-1 demonstrates patterns of hemorrhagic injury that can occur in both premature and term infants.
Neonatal Seizures
Neonatal seizures are often a manifestation of underlying neurologic disease or injury (Table 101-1). In each case, the metabolic or structural abnormalities cause disorganized electrical activity that can lead to epileptogenic foci.
Neonatal Hypotonia
Hypotonia is a common sign of neurologic disease in newborns that can be caused by dysfunction anywhere along the neuromuscular axis. These may arise from genetic defects causing protein dysfunction in either nerve or muscle cells, loss of cerebral regulation of tone secondary to global central nervous system (CNS) dysfunction as in many chromosomal disorders or injuries, or disturbed signal transmission at the neuromuscular junction. The more common causes of hypotonia can be organized by the location of the primary defect (Figure 101-2).
Clinical Presentation
Neonatal Seizures
Neonatal seizures have a variety of manifestations and a variety of normal mimics (Box 101-1). Clonic seizures can occur either focally or multifocally and are repetitive high-amplitude, low-frequency jerking movements. Tonic seizures are constant stiffening of a portion of the body and may be focal or generalized. Myoclonic seizures include sudden extension or flexion of part of the body. Subtle seizures encompass other small abnormal movements that do not fit into the previously listed seizure types, including eye deviation, lip smacking, and tongue thrusting, among others. Subtle seizures and generalized tonic seizures often do not have electroencephalographic (EEG) correlates and are thought to emanate from deeper subcortical brain regions, a theory supported by animal studies.
[/not-level-membership-for-pediatrics-category]
