[level-membership-for-pediatrics-category]
Chapter 655 Disorders of the Nails
Nail abnormalities in children may be manifestations of generalized skin disease, skin disease localized to the periungual region, systemic disease, drugs, trauma, or localized bacterial and fungal infections (Table 655-1). Nail anomalies are also common in certain congenital disorders (Table 655-2).
Table 655-1 WHITE NAIL OR NAIL BED CHANGES
| DISEASE | CLINICAL APPEARANCE |
|---|---|
| Anemia | Diffuse white |
| Arsenic | Mees lines: transverse white lines |
| Cirrhosis | Terry nails: most of nail, zone of pink at distal end (see Fig. 655-3) |
| Congenital leukonychia (autosomal dominant; variety of patterns) | Syndrome of leukonychia, knuckle pads, deafness; isolated finding; partial white |
| Darier disease | Longitudinal white streaks |
| Half-and-half nail | Proximal white, distal pink azotemia |
| High fevers (some diseases) | Transverse white lines |
| Hypoalbuminemia | Muehrcke lines: stationary paired transverse bands |
| Hypocalcemia | Variable white |
| Malnutrition | Diffuse white |
| Pellagra | Diffuse milky white |
| Punctate leukonychia | Common white spots |
| Tinea and yeast | Variable patterns |
| Thallium toxicity (rat poison) | Variable white |
| Trauma | Repeated manicure: transverse striations |
| Zinc deficiency | Diffuse white |
From Habif TP, editor: Clinical dermatology, ed 4, Philadelphia, 2004, Mosby, p 887.
Table 655-2 CONGENITAL DISEASES WITH NAIL DEFECTS
| Large nails | Pachyonychia congenita, Rubinstein-Taybi syndrome, hemihypertrophy |
| Smallness or absence of nails | Ectodermal dysplasias, nail-patella, dyskeratosis congenita, focal dermal hypoplasia, cartilage-hair hypoplasia, Ellis–van Creveld, Larsen, epidermolysis bullosa, incontinentia pigmenti, Rothmund-Thomson, Turner, popliteal web, trisomy 13, trisomy 18, Apert, Gorlin-Pindborg, long arm 21 deletion, otopalatodigital, fetal alcohol, fetal hydantoin, elfin facies, anonychia, acrodermatitis enteropathica |
| Other | Congenital malalignment of the great toenails, familial dystrophic shedding of the nails |
Abnormalities in Nail Shape or Size
Anonychia is absence of the nail plate, usually a result of a congenital disorder or trauma. It may be an isolated finding or may be associated with malformations of the digits. Koilonychia is flattening and concavity of the nail plate with loss of normal contour, producing a spoon-shaped nail (Fig. 655-1). Koilonychia occurs as an autosomal dominant trait or in association with iron deficiency anemia, Plummer-Vinson syndrome, or hemochromatosis. The nail plate is relatively thin for the first year or two of life and, consequently, may be spoon-shaped in otherwise normal children.

Figure 655-1 Spoon nails (koilonychia). Most cases are a variant of normal.
(From Habif TP, editor: Clinical dermatology, ed 4, Philadelphia, 2004, Mosby, p 885.)
For a discussion of pachyonychia congenita, see Chapter 650.
Clubbing of the nails (hippocratic nails) is characterized by swelling of each distal digit, an increase in the angle between the nail plate and the proximal nail fold (Lovibond angle) to >180 degrees, and a spongy feeling when one pushes down and away from the interphalangeal joint, because of an increase in fibrovascular tissue between the matrix and the phalanx (Fig. 655-2). The pathogenesis is not known. Nail clubbing is seen in association with diseases of numerous organ systems, including pulmonary, cardiovascular (cyanotic heart disease), gastrointestinal (celiac disease, inflammatory bowel disease), and hepatic (chronic hepatitis) systems, as well as in healthy individuals as an idiopathic or familial finding.

Changes in Nail Color
Leukonychia is a white opacity of the nail plate that may involve the entire plate or may be punctate or striate (see Table 655-1). The nail plate itself remains smooth and undamaged. Leukonychia can be traumatic or associated with infections such as leprosy and tuberculosis, dermatoses such as lichen planus and Darier disease, malignancies such as Hodgkin disease, anemia, and arsenic poisoning (Mees lines). Leukonychia of all nail surfaces is an uncommon hereditary autosomal dominant trait that may be associated with congenital epidermal cysts and renal calculi. Paired parallel white bands that do not change position with growth of the nail and thus reflect a change in the nail bed are associated with hypoalbuminemia and are called Muehrcke lines. When the proximal portion of the nail is white and the distal 20-50% of the nail is red, pink, or brown, the condition is called half-and-half nails or Lindsay nails; this is seen most commonly in patients with renal disease but may occur as a normal variant. White nails of cirrhosis, or Terry nails (Fig. 655-3), are characterized by a white ground-glass appearance of the entire or the proximal end of the nail and a normal pink distal 1-2 mm of the nail; this finding is associated with hypoalbuminemia.
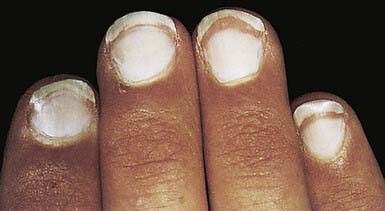
Figure 655-3 Terry nails. The nail bed is white with only a narrow zone of pink at the distal end.
(From Habif TP, editor: Clinical dermatology, ed 4, Philadelphia, 2004, Mosby, p 885.)
Bluish black to greenish nails may be caused by Pseudomonas infection (Fig. 655-4), particularly in association with onycholysis or chronic paronychia. The coloration is due to subungual debris and pyocyanin pigment from the bacterial organisms.

Nail Separation
Onycholysis indicates separation of the nail plate from the distal nail bed. Common causes are trauma, long-term exposure to moisture, hyperhidrosis, cosmetics, psoriasis, fungal infection (distal onycholysis), atopic or contact dermatitis, porphyria, drugs (bleomycin, vincristine, retinoid agents, indomethacin, chlorpromazine [Thorazine]), and drug-induced phototoxicity from tetracyclines (Fig. 655-5) or chloramphenicol.

Figure 655-5 Distal onycholysis secondary to oral tetracycline usage and ultraviolet light exposure.
Beau lines are transverse grooves in the nail plate (Fig. 655-6) that represent a temporary disruption of formation of the nail plate. The lines first appear a few weeks after the event that caused the disruption in nail growth. A single transverse ridge appears at the proximal nail fold in most 4- to 6-wk-old infants and works its way distally as the nail grows; this line may reflect metabolic changes after delivery. At other ages, Beau lines are usually indicative of periodic trauma or episodic shutdown of the nail matrix secondary to a systemic disease such as hand-foot-and-mouth disease, measles, mumps, pneumonia, or zinc deficiency. Onychomadesis is an exaggeration of Beau lines leading to proximal separation of the nail bed (Fig. 655-7).


Trachyonychia (20-nail Dystrophy)
Trachyonychia is characterized by longitudinal ridging, pitting, fragility, thinning, distal notching, and opalescent discoloration of all the nails (Fig. 655-8). Patients have no associated skin or systemic diseases and no other ectodermal defects. Its occasional association with alopecia areata has led some authorities to suggest that trachyonychia may reflect an abnormal immunologic response to the nail matrix, whereas histopathologic studies have suggested that it may be a manifestation of lichen planus, psoriasis, or spongiotic (eczematous) inflammation of the nail matrix. The disorder must be differentiated from fungal infections, psoriasis, nail changes of alopecia areata, and nail dystrophy secondary to eczema. Eczema and fungal infections rarely produce changes in all the nails simultaneously. The disorder is self-limited and eventually remits by adulthood.

Nail Infection
Fungal infection of the nails has been classified into 4 types. White superficial onychomycosis manifests as diffuse or speckled white discoloration of the surface of the toenails. It is caused primarily by Trichophyton mentagrophytes, which invades the nail plate. The organism may be scraped off the nail plate with a blade, but treatment is best accomplished by the addition of a topical azole antifungal agent. Distal subungual onychomycosis involves foci of onycholysis under the distal nail plate or along the lateral nail groove, followed by development of hyperkeratosis and yellow-brown discoloration. The process extends proximally, resulting in nail plate thickening, crumbling (Fig. 655-9), and separation from the nail bed. Trichophyton rubrum and, occasionally, T. mentagrophytes infect the toenails; fingernail disease is almost exclusively due to T. rubrum, which may be associated with superficial scaling of the plantar surface of the feet and often of one hand. The dermatophytes are found most readily at the most proximal area of the nail bed or adjacent ventral portion of the involved nail plates. Topical therapies such as ciclopirox 8% lacquer may be effective for solitary nail infection. Because of its long half-life in the nail, either terbinafine or itraconazole may be effective when given as pulse therapy (1 wk of each month for 3-4 mo). Dosage is weight dependent. Either agent is superior to griseofulvin, fluconazole, or ketoconazole. The risks, the most concerning of which is hepatic toxicity, and costs of oral therapy are minimized with the use of pulsed dosing.

Paronychial Inflammation
Paronychial inflammation may be acute or chronic and generally involves 1 or 2 nail folds on the fingers. Acute paronychia manifests as erythema, warmth, edema, and tenderness of the proximal nail fold, most commonly as a result of pathogenic staphylococci or streptococci (Fig. 655-10). Warm soaks and oral antibiotics are generally effective; incision and drainage may be occasionally necessary. Development of chronic paronychia follows prolonged immersion in water (Fig. 655-11), such as occurs in finger or thumb sucking, exposure to irritating solutions, nail fold trauma, or diseases, including Raynaud phenomenon, collagen vascular diseases, and diabetes. Swelling of the proximal nail fold is followed by separation of the nail fold from the underlying nail plate and suppuration. Foreign material, embedded in the dermis of the nail fold, becomes a nidus for inflammation and infection with Candida species and mixed bacterial flora. A combination of attention to predisposing factors, meticulous drying of the hands, and long-term topical antifungal agents and topical potent corticosteroids may be required for successful treatment of chronic paronychia.


De Berker D. Fungal nail disease. N Engl J Med. 2009;360:2108-2116.
De Berker D. Childhood nail diseases. Dermatol Clin. 2006;24:355-363.
Gregoriou S, Agryriou G, Larios G, et al. Nail disorders and systemic disease: what the nails tell us. J Fam Pract. 2008;57:509-514.
Ginter-Hanselmayer G, Weger W, Smolle J. Onychomycosis: a new emerging infection disease in childhood population and adolescents. Report on treatment experience with terbinafine and itraconazole. J Eur Acad Dermatol Venereol. 2008;22:470-475.
Seghal VN. Twenty nail dystrophy trachyonychia: an overview. J Dermatol. 2007;34:361-366.
Rogopoulos D, Larios G, Gregoriou S, et al. Acute and chronic paronychia. Am Fam Physician. 2008;77:339-346.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
Chapter 655 Disorders of the Nails
Nail abnormalities in children may be manifestations of generalized skin disease, skin disease localized to the periungual region, systemic disease, drugs, trauma, or localized bacterial and fungal infections (Table 655-1). Nail anomalies are also common in certain congenital disorders (Table 655-2).
Table 655-1 WHITE NAIL OR NAIL BED CHANGES
| DISEASE | CLINICAL APPEARANCE |
|---|---|
| Anemia | Diffuse white |
| Arsenic | Mees lines: transverse white lines |
| Cirrhosis | Terry nails: most of nail, zone of pink at distal end (see Fig. 655-3) |
| Congenital leukonychia (autosomal dominant; variety of patterns) | Syndrome of leukonychia, knuckle pads, deafness; isolated finding; partial white |
| Darier disease | Longitudinal white streaks |
| Half-and-half nail | Proximal white, distal pink azotemia |
| High fevers (some diseases) | Transverse white lines |
| Hypoalbuminemia | Muehrcke lines: stationary paired transverse bands |
| Hypocalcemia | Variable white |
| Malnutrition | Diffuse white |
| Pellagra | Diffuse milky white |
| Punctate leukonychia | Common white spots |
| Tinea and yeast | Variable patterns |
| Thallium toxicity (rat poison) | Variable white |
| Trauma | Repeated manicure: transverse striations |
| Zinc deficiency | Diffuse white |
From Habif TP, editor: Clinical dermatology, ed 4, Philadelphia, 2004, Mosby, p 887.
Table 655-2 CONGENITAL DISEASES WITH NAIL DEFECTS
| Large nails | Pachyonychia congenita, Rubinstein-Taybi syndrome, hemihypertrophy |
| Smallness or absence of nails | Ectodermal dysplasias, nail-patella, dyskeratosis congenita, focal dermal hypoplasia, cartilage-hair hypoplasia, Ellis–van Creveld, Larsen, epidermolysis bullosa, incontinentia pigmenti, Rothmund-Thomson, Turner, popliteal web, trisomy 13, trisomy 18, Apert, Gorlin-Pindborg, long arm 21 deletion, otopalatodigital, fetal alcohol, fetal hydantoin, elfin facies, anonychia, acrodermatitis enteropathica |
| Other | Congenital malalignment of the great toenails, familial dystrophic shedding of the nails |
Abnormalities in Nail Shape or Size
Anonychia is absence of the nail plate, usually a result of a congenital disorder or trauma. It may be an isolated finding or may be associated with malformations of the digits. Koilonychia is flattening and concavity of the nail plate with loss of normal contour, producing a spoon-shaped nail (Fig. 655-1). Koilonychia occurs as an autosomal dominant trait or in association with iron deficiency anemia, Plummer-Vinson syndrome, or hemochromatosis. The nail plate is relatively thin for the first year or two of life and, consequently, may be spoon-shaped in otherwise normal children.
Figure 655-1 Spoon nails (koilonychia). Most cases are a variant of normal.
(From Habif TP, editor: Clinical dermatology, ed 4, Philadelphia, 2004, Mosby, p 885.)
For a discussion of pachyonychia congenita, see Chapter 650.
Clubbing of the nails (hippocratic nails) is characterized by swelling of each distal digit, an increase in the angle between the nail plate and the proximal nail fold (Lovibond angle) to >180 degrees, and a spongy feeling when one pushes down and away from the interphalangeal joint, because of an increase in fibrovascular tissue between the matrix and the phalanx (Fig. 655-2). The pathogenesis is not known. Nail clubbing is seen in association with diseases of numerous organ systems, including pulmonary, cardiovascular (cyanotic heart disease), gastrointestinal (celiac disease, inflammatory bowel disease), and hepatic (chronic hepatitis) systems, as well as in healthy individuals as an idiopathic or familial finding.
