Chapter 691 Disorders for Which Defects Are Poorly Understood or Unknown
Ellis–Van Creveld Syndrome
Skeletal radiographs reveal short tubular bones with clubbed ends, especially the proximal tibia and ulna (Fig. 691-1). Carpal bones display extra ossification centers and fusion; cone-shaped epiphyses are evident in the hands. A bony spur is often noted above the medial aspect of the acetabulum.

Cartilage-Hair Hypoplasia
Radiographs show short tubular bones with flared, irregularly mineralized, and cupped metaphyses (Fig. 691-2). The knees are more affected than are the hips, and the fibula is disproportionately longer than the tibia. The metacarpals and phalanges are short and broad. Spinal radiographs reveal mild platyspondyly.

Metatropic Dysplasia
Skeletal radiographs show characteristic changes dominated by severe platyspondyly and short tubular bones with expanded and deformed metaphyses that exhibit a dumbbell appearance (Fig. 691-3). The pelvic bones are hypoplastic and exhibit a halberd appearance because of a small sacrosciatic notch and a notch above the lateral margin of the acetabulum.

Juvenile Osteochondroses
The juvenile osteochondroses are a heterogeneous group of disorders in which regional disturbances in bone growth cause noninflammatory arthropathies. They are summarized in Table 691-1. Some have localized pain and tenderness (Freiberg disease, Osgood-Schlatter disease, osteochondritis dissecans), whereas others present with painless limitation of joint movement (Legg-Calvé-Perthes disease, Scheuermann disease). Bone growth may be disrupted, leading to deformities. The diagnosis is usually confirmed radiographically, and treatment is symptomatic. The pathogenesis of these disorders is believed to involve ischemic necrosis of primary and secondary ossification centers. Although familial forms have been reported, these disorders usually occur sporadically.
| EPONYM | AFFECTED REGION | AGE AT PRESENTATION |
|---|---|---|
| Legg-Calvé-Perthes disease | Capital femoral epiphysis | 3-12 yr |
| Osgood-Schlatter disease | Tibial tubercle | 10-16 yr |
| Sever disease | Os calcaneus | 6-10 yr |
| Freiberg disease | Head of second metatarsal | 10-14 yr |
| Scheuermann disease | Vertebral bodies | Adolescence |
| Blount disease | Medial aspect of proximal tibial epiphysis | Infancy or adolescence |
| Osteochondritis dissecans | Subchondral regions of knee, hip, elbow, and ankle | Adolescence |
Caffey Disease (Infantile Cortical Hyperostosis)
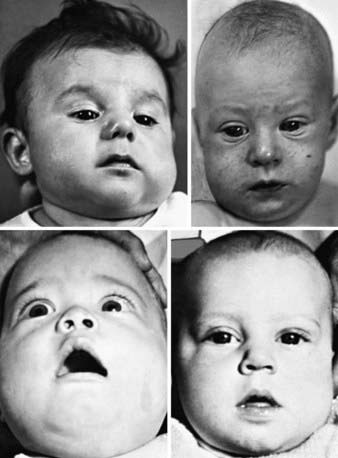
Prenatal and more often postnatal onset have been described. Prenatal onset may be mild (autosomal dominant) or severe (autosomal recessive). Severe prenatal disease is characterized by typical bone lesions, polyhydramnios, hydrops fetalis, severe respiratory distress, prematurity, and high mortality. Onset in infancy (<6 mo; average, 10 wk) is most common; manifestations include the sudden onset of irritability, swelling of contiguous soft tissue that precedes the cortical thickening of the underlying bones, fever, and anorexia. The swelling is painful with a woodlike induration but with minimal warmth or redness; suppuration is absent. There are unpredictable remissions and relapses; an episode can last 2 wk to 3 mo. The most common bones involved include the mandible (75%) (Fig. 691-4), the clavicle, and the ulna. If swelling is not prominent or visible, the diagnosis might not be evident.
Laboratory features include elevated erythrocyte sedimentation rate and serum alkaline phosphatase as well as, in some patients, increased serum prostaglandin E levels. There may be thrombocytosis and anemia. The radiographic features include soft-tissue swelling and calcification and cortical hyperostosis (Fig. 691-5). All bones may be affected except the phalanges or vertebral bodies. The differential diagnosis includes other causes of hyperostosis such as chronic vitamin A intoxication, prolonged prostaglandin E infusion in children with ductal dependent congenital heart disease, primary bone tumors, and scurvy.

 mo of age. Pressure from the external thickenings has forced the radial heads laterad out of the elbows. B, At
mo of age. Pressure from the external thickenings has forced the radial heads laterad out of the elbows. B, At  mo, 9 mo after onset, all affected bones are still greatly swollen, owing largely to expansion of the medullary cavities, although there are still residues of the earlier cortical thickening. The radial heads are still dislocated, and the radial diaphyses are now anchored in this ectopic position by solid bony bridges between them and the ulnar diaphyses, a single bridge on the right and three on the left. At 32 mo, these bridges were still intact, although they had diminished slightly in caliber. It is possible that these bony bridges represent ossification of parts of the interosseous membrane.
mo, 9 mo after onset, all affected bones are still greatly swollen, owing largely to expansion of the medullary cavities, although there are still residues of the earlier cortical thickening. The radial heads are still dislocated, and the radial diaphyses are now anchored in this ectopic position by solid bony bridges between them and the ulnar diaphyses, a single bridge on the right and three on the left. At 32 mo, these bridges were still intact, although they had diminished slightly in caliber. It is possible that these bony bridges represent ossification of parts of the interosseous membrane.Treatment includes indomethacin and prednisone if there is a poor response to indomethacin.
Baujat G, Le Merrer M. Ellis-van Creveld syndrome. Orphanet J Rare Dis. 2007;2:27.
Dagoneau N, Goulet M, Genevieve D, et al. DYNC2H1 mutations cause asphyxiating thoracic dystrophy and short rib-polydactyly syndrome, type III. Am J Hum Genet. 2009;84:706-711.
de Vries J, Yntema JL, van Die CE, et al. Jeune syndrome: description of 13 cases and a proposal for follow-up protocol. Eur J Pediatr. 2010;169(1):77-88.
Genevieve D, Le Merrer M, Feingold J, et al. Revisiting metatropic dysplasia: presentation of a series of 19 novel patients and review of the literature. Am J Med Genet A. 2008;146:992-996.
Glorieux FH. Caffey disease: an unlikely collagenopathy. J Clin Invest. 2005;115:1142-1144.
Kamoun-Goldrat A, le Merrer M. Infantile cortical hyperostosis (Caffey disease): a review. J Oral Maxillofac Surg. 2008;66:2145-2150.
Krakow D, Robertson SP, King LM, et al. Mutations in the gene encoding filamin b disrupt vertebral segmentation, joint formation and skeletogenesis. Nat Genet. 2004;36:405-410.
Makitie O, Sulisalo T, de la Chapelle A, et al. Cartilage-hair hypoplasia. J Med Genet. 1995;32:39-43.
Restrepo S, Sanchez AM, Palacios E. Infantile cortical hyperostosis of the mandible. Ear Nose Throat J. 2004;83:454-455.
Ruiz-Perez VL, Ide SE, Strom TM, et al. Mutations in a new gene in Ellis-van Creveld syndrome and weyers acrodental dysostosis. Nat Genet. 2000;24:283-286.
Sharrard WJW. Abnormalities of the epiphyses and limb inequality. In: Sharrard WJW, editor. Paediatric orthopaedics and fracture. Oxford, UK: Blackwell Scientific Publications, 1993.
Taskinen M, Ranki A, Pukkala E, et al. Extended follow-up of the Finnish cartilage-hair hypoplasia cohort confirms high incidence of non-Hodgkin lymphoma and basal cell carcinoma. Am J Med Genet A. 2008;146:2370-2375.
Thiel CT, Mortier G, Kaitila I, et al. Type and level of rmrp functional impairment predicts phenotype in the cartilage hair hypoplasia-anauxetic dysplasia spectrum. Am J Hum Genet. 2007;81:519-529.





