90
Cysts
Introduction
True Cysts – Common
Epidermoid Inclusion Cyst (EIC) (Epidermal Inclusion Cyst, ‘Sebaceous Cyst’)
• A visible comedonal-like opening or pore (resembles a blackhead) may be seen on the surface of the papule or nodule (Fig. 90.1A).


Fig. 90.1 Epidermoid inclusion cysts. A Typical clinical appearance of an epidermoid inclusion cyst with a yellowish hue. Two pores are present in this example. B Painful inflammatory reactions to cyst rupture are a frequent cause for presentation to a physician. Culture will often prove these lesions to be sterile, even if draining pus. Antibiotic treatment can be helpful due to their anti-inflammatory effects. B, Courtesy, Mary S. Stone, MD.
• Cyst contents may rupture into the dermis, eliciting an acute and chronic inflammatory reaction, leading to significant redness and pain; this inflammation is often confused with a bacterial infection (Fig. 90.1B).
• Most commonly sporadic; multiple lesions rarely associated with Gardner syndrome or Gorlin syndrome.
Milium (Milia – Plural)
• A small, superficial (1–2 mm), firm cyst that is white in color and is sometimes confused with a whitehead (Fig. 90.2); occasionally they are grouped.

• Commonly observed on the face in newborns; in this setting, they often resolve spontaneously.
• The majority of patients with multiple facial milia have no underlying condition; however, there may be a secondary cause (Table 90.1).
Pilar Cyst (Wen)
• Most common location is the scalp; sometimes there is associated overlying alopecia (Fig. 90.3).

Fig. 90.3 Pilar cyst. A non-inflamed pilar cyst is skin-colored, mobile, and has a smooth surface. Courtesy, Mary S. Stone, MD.
• Solitary or multiple relatively firm nodules.
Pilonidal Cyst
True Cysts – Less Common
Vellus Hair Cyst

Steatocystoma
• 2- to 10-mm, skin-colored to pigmented papule or nodule, usually multiple and grouped; commonly develop on the trunk or in the axillae and groin (Fig. 90.5).


Hidrocystoma
Apocrine
• Often a solitary, translucent to bluish papule on the eyelid margin (Fig. 90.6).

Fig. 90.6 Apocrine hidrocystoma. A single, slightly bluish, translucent papule on the lower eyelid near the lateral canthus. Courtesy, Mary S. Stone, MD.
• Histology: the lining resembles that of an apocrine gland (decapitation secretion).
• Rx: if bothersome or symptomatic, excision by an experienced surgeon.

‘False’ Cysts (No True Epithelial Lining)
Mucocele
• Compressible mucosal-colored to bluish papule or nodule, most commonly seen on the lower, inner mucosal lip (Fig. 90.8).

Fig. 90.8 Mucocele. A bluish translucent papule on the lower mucosal lip. Courtesy, Mary S. Stone, MD.
• Secondary to disruption of the minor salivary ducts.
• Rx: if persistent, excision or other destructive procedure, intralesional CS.
Digital Mucous Cyst
• Translucent, skin-colored to bluish papule or nodule most commonly on digits, in particular the dorsal, distal finger near the distal interphalangeal joint (Fig. 90.9).

Fig. 90.9 Digital mucous cyst. A translucent papule on the dorsal distal phalanx of the finger causing a depression in the nail plate. Courtesy, Mary S. Stone, MD.
• There may be a connection to the joint space.
• Occurs in the setting of osteoarthritis.
• Longitudinal nail deformity may be present when the lesion compresses the nail matrix.
• Puncture can result in drainage of a gelatinous material.
• Rx: observation, intralesional CS, repeated incision and drainage, excision.
Ganglion Cyst
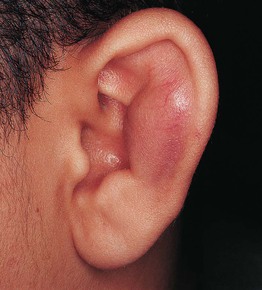
Pseudocyst of the Auricle
• Painless swelling, generally unilateral, of the scaphoid fossa of the ear (Fig. 90.10).
For further information see Ch. 110. From Dermatology, Third Edition.






