CHAPTER 42 Correction of the deviated septum
Physical evaluation
• Thorough history: A detailed patient history including history of nasal trauma, previous nasal surgery, airway complaints, allergies, and age is obtained. A negative history of airway obstruction is not a reliable indication of a patent airway, since the patient has no basis for comparison.
• Facial analysis: The nose and face are evaluated in 3 dimensions and findings are confirmed with soft tissue cephalometric analysis of life-size photographs. This is performed in order to assess symmetry of the nose and its relationship to other facial structures. Asymmetry may be present in other facial features, thus affecting the global evaluation of the face. The AP view of the face is also used to evaluate the dorsal nasal aesthetic lines as well as the width of the nasal dorsum.
• Often, the nasal bones follow the direction of the deviated septum, however these structures may move independently. Deviation of the lower nose may involve the caudal septum, anterior nasal spine, and the lower lateral cartilages.
• Midvault deviation consistently accompanies at least anterior and commonly mid and posterior septal deviation.
• In all types of septal deviation, the middle and/or inferior turbinates may be enlarged. The enlargement is usually juxtaposed to the concave side of the septum.
• There are six classes of septal deviation.
Technical steps
Nasal bones/upper lateral cartilage
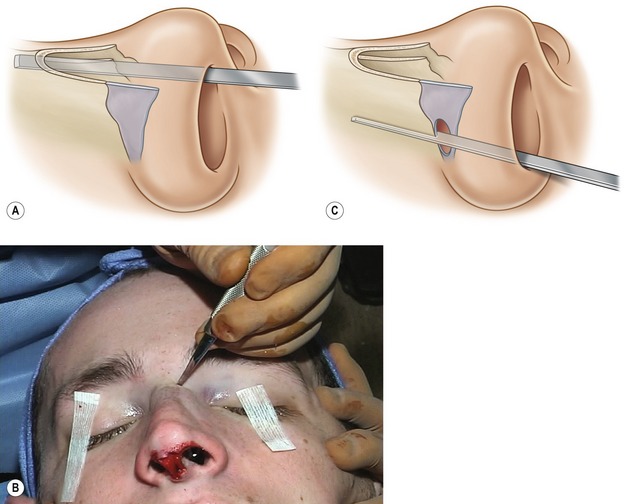
Prior to osteotomy, a push rasp is utilized in order to remove any bony hump. The rasp is angled toward the cheek to minimize the chance of septal fracture. After removing the hump, the upper nose is reassessed for symmetry. Often there may be far worse deviation than expected of the upper nose after hump removal. A medial osteotomy is first performed with a 4 or 6 mm osteotome, which is placed medial to the nasal bones and advanced cephalically with careful use of a mallet (Fig. 42.4A). A vertical osteotomy is then done with a 2 mm osteotome. The osteotome is percutaneously placed anteriorly in order to avoid the angular vessels (Fig. 42.4B). It is then directed posteriorly and cephalically and several interrupted osteotomies are made. After a small stab incision at the nasal vestibule with a #15 blade, a Joseph’s periosteal elevator is then used to incise the vestibular lining and elevate the periosteum. An internal low-to-low osteotomy is performed using a guarded osteotome and carried posterior to the natural suture line (Fig. 42.4C). A portion of the osteotomy is therefore made in the frontal process of the maxilla. This avoids the lateral step deformity seen after some osteotomies. Following adequate osteotomies, the upper lateral cartilages are assessed. There is often a discrepancy in the upper lateral cartilage length after the completion of the osteotomy. If a difference in length in the upper lateral cartilage exists, they may be trimmed in order to obtain symmetry. If the cephalic nasal asymmetry is unilateral only, the defect may be camouflaged using an onlay cartilage graft. However, correcting the unilateral defect with an osteotomy is preferred for its functional superiority.
Septum
Septal tilt
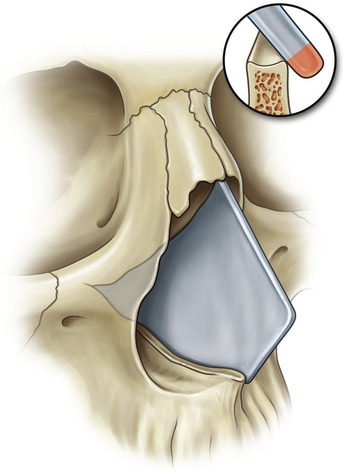
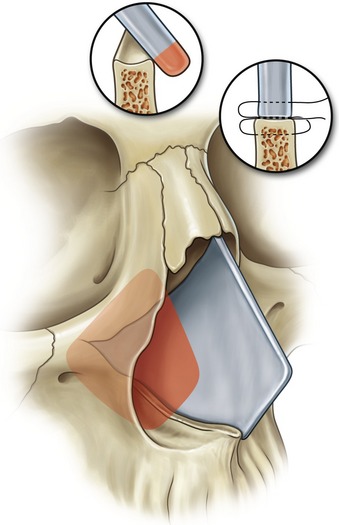
The septal tilt is corrected by initially removing the posterio-caudal portion of the septum, leaving an L-strut septum anteriorly and caudally. The sharp end of the septal elevator is used to incise the septal cartilage and the dull end is used to elevate the mucoperichondrium. At least 10 mm of cartilage is maintained anteriorly. The remainder of the posterocaudal septum is disengaged from the vomerine groove and anterior nasal spine. The septum must then be repositioned after removal of a small segment of the overlapping cartilage and fixated in the midline (Fig. 42.5). This is performed with a figure-of-eight suture using 5-0 PDS. Prior to repositioning of the septum, it is imperative that the anterior nasal spine be in the midline, otherwise correction of the septal deformity will not be adequate. The nasal spine may be repositioned with an osteotomy, if needed.
C-shaped deviation
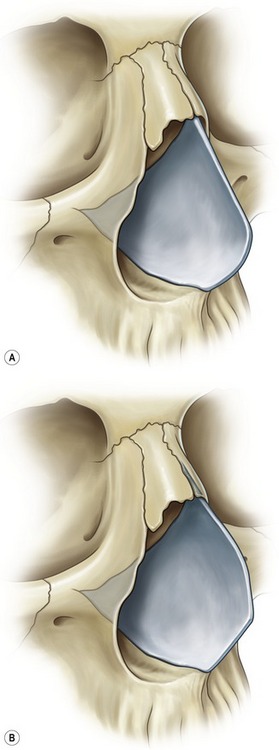
Correction of the anteroposterior deformity first requires resection of the posterio-caudal portion of the septum, as described for septal tilt. An osteotomy of the anterior nasal spine and residual vomerine plate is often necessary in order to place this structure in the midline. Also, partial disjunction of the perpendicular plate of the ethmoid and quadrangle cartilage is done only if deemed beneficial to correct the deviation in the cephalic third of the nose. Finally, the L-shaped frame is scored in a cephalocaudal direction on the concave surface if the other measures do not result in straightening the septum. Bilateral extramucosal stents (Simple-stents) are placed and fixed in position with a through-and-through suture. Stents are left for three weeks (Fig. 42.6A).
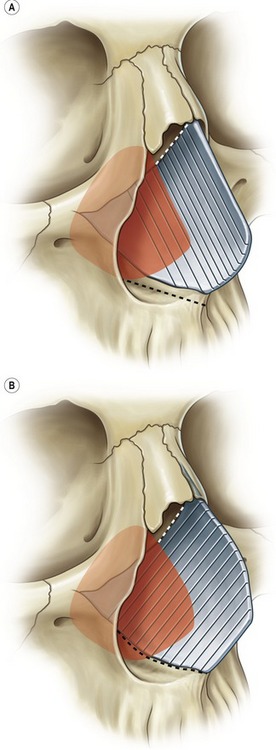
Correction of the cephalocaudal deformity also requires resection of the posterio-caudal septum (Fig. 42.6B). Complete separation of the junction between the cartilaginous septum and the maxillary crest is performed, as well as a partial release of the cephalic portion of the quadrangular cartilage from the perpendicular cartilage if deemed necessary. An anterior nasal spine osteotomy may be needed to correct deviation at this level. The caudal cartilage is scored in an anteroposterior orientation on the concave side of the deformity. Spreader grafts are also utilized anteriorly. If deviation only involves the caudal septum, bilateral spreader grafts and a septal rotation suture may suffice. Internal extramucosal stents are then placed.
S-shaped deviation
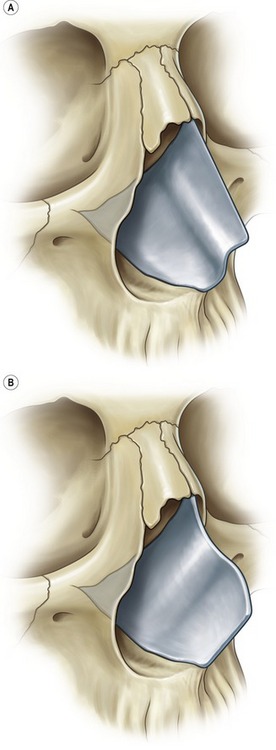
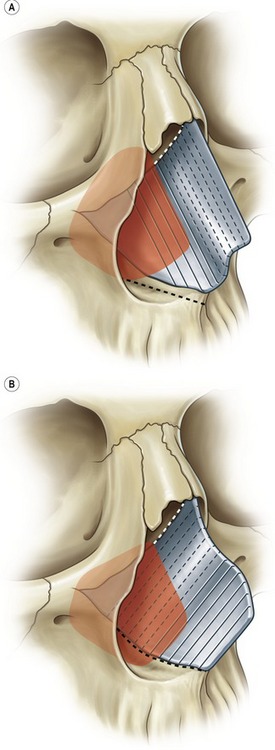
The cephalocaudal and anteroposterior S-shaped septal deviations are treated similarly to the techniques described above for C-shaped septal deviations (Fig. 42.7). For both types, the posterio-caudal septum is resected as described above. If the deviation is cephalocaudal, the cartilage will be scored in an anteroposterior direction, whereas if the deviation is anteroposterior, the scoring will be performed in a cephalocaudal orientation. Scoring is always performed on the concave surface of the deformity. In either case, the anterior nasal spine and the vomerine bone are carefully examined and repositioned to midline using an osteotomy, if worthwhile. Partial mobilization of the perpendicular plate and quadrangle cartilage is considered only if the septum remains deviated. The anterior septum is controlled using bilateral spreader grafts (Fig. 42.8). Extramucosal internal stents are placed posteriorly as previously described.
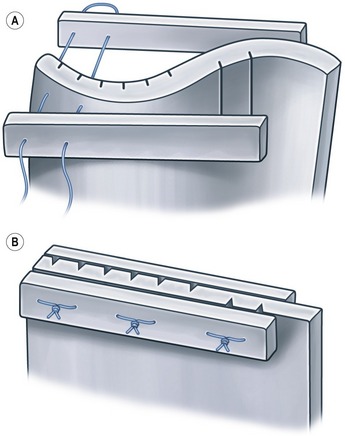
If the caudal septal deviation persists despite septal surgery, cartilaginous scoring, and straightening with spreader grafts, a septal rotation suture is placed. A 5-0 polydioxanone suture is placed through the upper lateral cartilage on the deviated side caudally, through the septum/spreader graft composite, and through the opposite upper lateral cartilage cephalically. The suture is then returned to the deviated side and tied, effectively repositioning the caudal septum. A second suture is placed across the upper lateral cartilages and spreader graft-septum composite to prevent bowing of the cartilages.
Lower lateral cartilage
Failure to recognize and correct asymmetry in the lower lateral cartilages may lead to persistent tip asymmetry postoperatively. Following septal correction and release of the lower lateral cartilages, discrepancies in size and projection of the lower lateral cartilages may become evident. Once the septum is repositioned on the maxillary crest, the deviation located at the caudal septum is evaluated. The medial and lateral crura are measured using calipers. Typically, the longer cartilage is located on the side opposite to the deviation. Depending on the tip projection relative to the dorsum, either the crura of the longer lower lateral cartilage is shortened to match the length of the contralateral side or elongated. This can be achieved by transecting and overlapping the lateral crus and shortening the medial crus, if the shortening seems to meet the aesthetic goals. Otherwise the short lower lateral cartilage is dissected and advanced to the level of the opposite lower lateral cartilage and fixed to the columellar strut. Excessive medial crura may also be excised at the footplate region.
Postoperative care
Following the completion of the procedure, a dorsal splint is applied. The dorsal splint reapproximates the free tissue envelope to the corrected framework. A combination of metal splints and Aquaplast over Steri-Strips is preferred. The Aquaplast provides stability whereas the metal portion allows precise molding of the Aquaplast splint. Doyle splints are also placed within the nostrils in an extramucosal fashion. The use of the Doyle splints allows further stabilization of the septum. Splints are left on for 8 days. The Simple-Stent extramucosal internal stents that are placed after any septal correction surgery are kept in for several weeks. The patient is kept on a first generation cephalosporin for the duration that the Doyle internal splints are used. A Medrol dose-pack is also prescribed to minimize swelling and bruising. Heavy physical activity is curtailed for three weeks.
Complications
Pearls & pitfalls
Pearls
• Understanding the septum has become the cornerstone to the reconstruction and functional restoration of the crooked nose.
• The anatomic deviation may be at the bony pyramid, the upper lateral cartilages, the lower lateral cartilages, the caudal septum, or any combination of these entities.
• The ultimate goal is to provide a consistent, stable long-term correction that is both aesthetically pleasing and functionally sound.
Pitfalls
• The shortfalling of this procedure is that the healing of the cartilage and the bone can not be controlled completely.
• However, adherence to the above recommended diagnostic and surgical algorithm will result in more predictable outcomes.
• It is a meticulous process and is fraught with pitfalls.
• Once the primary rhinoplasty is performed, secondary revisions for latent deviation are even more problematic due to alteration of normal nasal architecture.
Summary of steps
1. Thorough history and physical examination: History of nasal trauma, prior nasal surgery, airway complaints, and allergies are ascertained. Three-dimensional evaluation as well as cephalometric analysis of life-size photographs is performed in order to evaluate the location and severity of asymmetry. A detailed evaluation of the upper nose (nasal bones and upper lateral cartilages), septum, lower lateral cartilages, anterior nasal spine and medial crural footplates will give an accurate assessment of asymmetry.
2. Anesthesia and vasoconstriction is administered via general anesthesia and infiltration of lidocaine with 1 : 200,000 epinephrine. The nose is packed with 4% cocaine posteriorly and cephalically. Repeat injection of the nose is performed with lidocaine with 1 : 100,000 epinephrine.
3. A stair step incision is made in the columella and continued on the caudal margin of the medial and lateral crura of the lower lateral cartilages.
4. Wide exposure of the upper and lower lateral cartilages is performed with care to ensure adequate vascularity to the nasal skin flaps.
5. Nasal bones are exposed using a subperiosteal dissection.
6. A cephalic trim of the lower lateral cartilages leaves 4 mm of cartilage anteriorly and at least 6 mm of cartilage posteriorly.
7. Bony and cartilaginous hump removal with a push rasp.
8. Medial osteotomy with 4 or 6 mm osteotome.
9. Vertical percutaneous osteotomy with 2 mm osteotome.
10. Internal low-to-low osteotomy.
11. Assessment of the upper lateral cartilages and trim to symmetry.
12. The septum is accessed via a mucoperichondrial flap.
13. Septal deviation is then corrected using a variety of techniques including posterior caudal septal resection, leaving an L-strut with at least 10 mm of cartilage anteriorly. Depending on the type of septal deformity, cartilaginous scoring, partial mobilization of the perpendicular plate and quadrangle cartilage, and anterior nasal spine osteotomy may become necessary.
14. Lower lateral cartilages are measured with calipers. If discrepancy in size of the lower lateral cartilages exists, the longer lateral crus is trimmed and repositioned to match the length of the contralateral side or the shorter lower lateral cartilage is elongated.
15. The anterior nasal spine may have to be repositioned with an osteotomy.
16. The medial crural footplates may require mobilization, and straightening with fixation to a columellar strut.
17. The anterior septum is supported using bilateral spreader grafts.
18. Internal extramucosal stents are placed to aid fixation of the straightened septum while healing.
19. Dorsal nasal splint using with an Aquaplast and metal splint provides stability and allows the soft tissue envelope to adhere to the corrected framework.
20. The patient is kept on a first-generation cephalosporin for the duration of the internal Doyle splinting, usually eight days. A Medrol dose-pack may also be used to minimize swelling and bruising. Heavy physical activity is curtailed for 3 weeks.
Byrd HS, et al. The crooked nose: an algorithm for repair. In: Gunter JP, Rohrich RJ, Adams W. Dallas rhinoplasty. St. Louis: Quality Medical Publishing; 2007:999–1014.
Byrd HS, Salomon J, Flood J. Correction of the crooked nose. Plast Reconstr Surg. 1998;102:2148–2157.
Fancesconi G, Fenili O. Treatment of deflection of the anterocaudal portion of the nasal septum. Plast Reconstr Surg. 1973;5:342–345.
Foda HMT. The role of septal surgery in management of the deviated nose. Plast Reconstr Surg. 2005;115:406–415.
Gunter JP, Rohrich RJ. Management of the deviated nose: the importance of septal reconstruction. Clin Plast Surg. 1988;15:43–55.
Guyuron B, Behmand RA. Caudal nasal deviation. Plast Reconstr Surg. 2003;111:2449–2457.
Guyuron B. Classification of septal deviation and reconstructive technique. In: Gunter JP, Rohrich RJ, Adams WP. Dallas rhinoplasty. St. Louis, MO: Quality Medical Publishing; 2007:929–938.
Guyuron B. Precision rhinoplasty. Part I: The role of life-size photographs and soft-tissue cephalometric analysis. Plast Reconstr Surg. 1988;81(4):489–499.
Mowlavi A, et al. Septal cartilage defined: Implications for nasal dynamics and rhinoplasty. Plast Reconstr Surg. 2006;117:2171–2174.
Rohrich RJ, et al. The deviated nose: optimizing results using a simplified classification and algorithmic approach. Plast Reconstr Surg. 2002;110:1509–1523.





