[level-membership-for-critical-care-medicine-category]
Chapter 23 Cor Pulmonale
2 What are the subtypes of cor pulmonale?
Cor pulmonale can be acute or chronic.
 In acute cor pulmonale the afterload to the right ventricle can rise in a matter of minutes (e.g., massive pulmonary embolism) giving very little room for compensation. The result will be acute right ventricular dilatation and failure, its severity depending primarily on the degree of acute PA hypertension.
In acute cor pulmonale the afterload to the right ventricle can rise in a matter of minutes (e.g., massive pulmonary embolism) giving very little room for compensation. The result will be acute right ventricular dilatation and failure, its severity depending primarily on the degree of acute PA hypertension.

3 What is the pathophysiology of right ventricular failure?
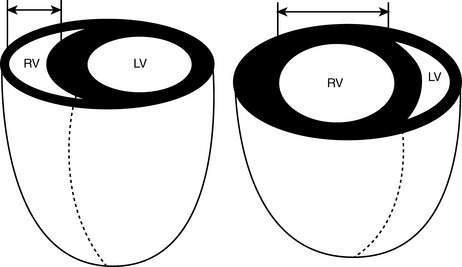
Under normal conditions, the pulmonary circulation is a low-resistance circuit, and the right ventricle generates the same stroke volume as the left ventricle with end-systolic pressures that are just 20% to 25% of those in the left ventricle. The low pressure within the thin free wall of the right ventricle also allows myocardial perfusion to occur both in systole and in diastole. Because of its structure, similar to that of veins rather than arteries, the right ventricle accommodates well additional volume but not higher pressure. When pressure overload occurs acutely, the right ventricle can only dilate and, if the pressure is sufficiently elevated, fail. Chronically, in response to increased systolic workload the free wall of the right ventricle hypertrophies and becomes similar to the left ventricle. Laplace’s law helps explaining the evolution from hypertrophy to dilatation and failure (Fig. 23-1): In a thin-wall chamber, an increase in intraluminal pressure increases wall stress unless thickness increases or the internal radius decreases. As the right ventricle hypertrophies, myocardial perfusion becomes limited to diastole, making its myocardium more susceptible to ischemia, and thus leading to dilatation and failure.
4 What are the causes of cor pulmonale?
Any process that results in pulmonary hypertension can cause cor pulmonale. Pulmonary hypertension is defined as mean PA pressures > 20 mm Hg at rest or > 30 mm Hg with exercise. The most frequent cause of pulmonary hypertension and cor pulmonale is COPD, due to chronic hypoxemia. In COPD the degree of hypertension is generally moderate, and oxygen supplementation may be effective in relieving some of the pressure load to the right ventricle and delaying failure. Additional causes of cor pulmonale include chronic pulmonary thromboembolic disease, left-sided cardiac abnormalities, untreated obstructive sleep apnea (OSA), interstitial lung diseases, and primary pulmonary hypertension. A comprehensive classification of the diseases of the lung associated with PA hypertension and cor pulmonale is shown in Table 23-1.
Table 23-1 Classification of cor pulmonale according to causative factor
| Category | Example |
|---|---|
| Diseases affecting the air passages of the lung and alveoli | COPD Cystic fibrosis Infiltrative or granulomatous defects Idiopathic pulmonary fibrosis Sarcoidosis Pneumoconiosis Scleroderma Mixed connective tissue disease Systemic lupus erythematosus Rheumatoid arthritis Polymyositis Eosinophilic granulomatosis Radiation Malignant infiltration |
| Diseases affecting thoracic cage movement | Kyphoscoliosis Thoracoplasty Neuromuscular weakness Sleep apnea syndrome Idiopathic hypoventilation |
| Diseases affecting the pulmonary vasculature | Primary disease of the arterial wall Primary pulmonary hypertension Pulmonary arteritis Toxin-induced pulmonary hypertension Chronic liver disease Peripheral pulmonary stenosis |
| Thrombotic disorders | Sickle cell diseases Pulmonary microthrombi |
| Embolic disorders | Thromboembolism Tumor embolism Other embolic processes (amniotic fluid, air, fat) Schistosomiasis and other parasitic infections |
| Pressure on PAs | Mediastinal tumors Aneurysms Granulomata Fibrosis |
Modified from Rubin LJ, ed: Pulmonary Heart Disease. Boston, 1984, Martinus Nijhoff, p 4.
7 What are the signs and symptoms of cor pulmonale?
Symptoms of cor pulmonale include the following:












9 What are the electrocardiographic (ECG) findings associated with right ventricular hypertrophy?
 Right axis deviation: QRS negative in lead I, positive in aVR
Right axis deviation: QRS negative in lead I, positive in aVR
 Tall R waves in the right precordial leads, deep S waves in the left precordial leads
Tall R waves in the right precordial leads, deep S waves in the left precordial leads
 Right atrial enlargement: P pulmonale, large P wave, in II and V1
Right atrial enlargement: P pulmonale, large P wave, in II and V1
 ST-segment changes in the opposite direction of the QRS (i.e., wide QRS-ST angle)
ST-segment changes in the opposite direction of the QRS (i.e., wide QRS-ST angle)
 Right bundle branch block: wide QRS (> 1.12 seconds); RSR′ in V1 and V2
Right bundle branch block: wide QRS (> 1.12 seconds); RSR′ in V1 and V2
11 What tests can help determine the diagnosis of cor pulmonale?
Laboratory investigations to detect the underlying cause of cor pulmonale may include the following:
 Arterial blood gas analysis with acid-base status.
Arterial blood gas analysis with acid-base status.
 Hematocrit to detect polycythemia.
Hematocrit to detect polycythemia.

 Antinuclear antibody level for connective tissue diseases, such as scleroderma.
Antinuclear antibody level for connective tissue diseases, such as scleroderma.

Radiographic findings include the following:

 Enlargement of the central PAs (right PA > 16 mm, left PA > 18 mm) with oligemic peripheral lung fields (Westermark sign)
Enlargement of the central PAs (right PA > 16 mm, left PA > 18 mm) with oligemic peripheral lung fields (Westermark sign)


 Computed tomography and computed tomographic angiography
Computed tomography and computed tomographic angiography
 Dilation of the main PA diameter (≥ 29 mm has a reported sensitivity of 84% and a specificity of 75% for diagnosing pulmonary hypertension).
Dilation of the main PA diameter (≥ 29 mm has a reported sensitivity of 84% and a specificity of 75% for diagnosing pulmonary hypertension).

 Ultrafast, ECG-gated computed tomography (CT)
Ultrafast, ECG-gated computed tomography (CT)
 Ultrafast, ECG-gated CT has been evaluated to study right ventricular function: it may estimate ejection fraction and wall mass with high accuracy.
Ultrafast, ECG-gated CT has been evaluated to study right ventricular function: it may estimate ejection fraction and wall mass with high accuracy. Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA)
Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA)




Echocardiographic findings include the following:
 Transthoracic and transesophageal two-dimensional echocardiography (TTE and TEE, respectively) can be used to evaluate ventricular size and function, valvular dysfunction, and pulmonary hypertension.
Transthoracic and transesophageal two-dimensional echocardiography (TTE and TEE, respectively) can be used to evaluate ventricular size and function, valvular dysfunction, and pulmonary hypertension.



 Doppler echocardiography is used to estimate PA pressure noninvasively.
Doppler echocardiography is used to estimate PA pressure noninvasively.




12 What are the indications for use of echocardiography in the evaluation of cor pulmonale?
Indications for TEE and diagnosis of pulmonary hypertension include the following:
Class I: Conditions for which evidence and/or general agreement of an effective treatment exist
Class II: Conditions for which conflicting evidence and/or a divergence of opinion exist about the usefulness or efficacy of a procedure or treatment
Class III: Conditions for which evidence and/or general agreement exist that the treatment is not effective and in some cases may be harmful
13 Discuss nonpharmacologic treatment options for patients with cor pulmonale
 Lifestyle modifications. Although data are not available, it seems sensible that promoting a healthy lifestyle that includes moderate aerobic exercise and weight reduction should be beneficial. Strenuous activity should be avoided, and supplemental oxygen may be beneficial during even graded exercise, such as walking.
Lifestyle modifications. Although data are not available, it seems sensible that promoting a healthy lifestyle that includes moderate aerobic exercise and weight reduction should be beneficial. Strenuous activity should be avoided, and supplemental oxygen may be beneficial during even graded exercise, such as walking.



14 What are the pharmacologic therapies for patients with cor pulmonale?



15 Discuss the different classes of vasodilators used in the treatment of cor pulmonale
Long-term treatment of cor pulmonale includes the following:
 Calcium channel blockers (nifedipine, diltiazem, amlodipine) have been used both in the short term as a test of pulmonary vascular responsiveness and in the long term as therapy.
Calcium channel blockers (nifedipine, diltiazem, amlodipine) have been used both in the short term as a test of pulmonary vascular responsiveness and in the long term as therapy.



Vasodilators for acute cor pulmonale include the following:
 Bridge treatment while other options are worked out and
Bridge treatment while other options are worked out and
 Test of reactivity of the pulmonary circulation for chronic vasodilator therapy with other drugs.
Test of reactivity of the pulmonary circulation for chronic vasodilator therapy with other drugs.
Inotropes with vasodilatory properties include the following:
 Dobutamine is the prototype of these agents. Dobutamine is a catecholamine with β1 and β2 adrenergic vascular effects. Dobutamine enhances myocardial contractility and decreases vascular resistance, thus increasing stroke volume and decreasing pulmonary and systemic pressure. The balance of these actions determines the effectiveness of the drug in each individual patient. Ideally, it will decrease PA pressure and increase cardiac output enough to maintain an adequate systemic blood pressure. Its effect is limited by systemic hypotension and tachycardia. An advantage of this drug is that, like all catecholamines, it has a short half-life, and its effect regresses rapidly on discontinuation.
Dobutamine is the prototype of these agents. Dobutamine is a catecholamine with β1 and β2 adrenergic vascular effects. Dobutamine enhances myocardial contractility and decreases vascular resistance, thus increasing stroke volume and decreasing pulmonary and systemic pressure. The balance of these actions determines the effectiveness of the drug in each individual patient. Ideally, it will decrease PA pressure and increase cardiac output enough to maintain an adequate systemic blood pressure. Its effect is limited by systemic hypotension and tachycardia. An advantage of this drug is that, like all catecholamines, it has a short half-life, and its effect regresses rapidly on discontinuation.





1 American College of Cardiology Foundation: 2003 Guideline Update for the Clinical Application of Echocardiography: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Washington: DC; 2003.
2 Bogaart H.J., Abe K., Noordergraf A.V., et al. The right ventricle under pressure. Cellular and molecular mechanisms of right-heart failure in pulmonary hypertension. Chest. 2009;135:794–804.
3 Criner G.J. Effects of long-term oxygen therapy on mortality and morbidity. Respir Care. 2000;45:105–118.
4 Gordon C., Collard C.D., Pan W. Intraoperative management of pulmonary hypertension and associated right heart failure. Curr Opin Anaesthesiol. 2010;23:49–56.
5 Haddad F., Couture P., Tousignant C., et al. The right ventricle in cardiac surgery, a perioperative perspective: I. Anatomy, physiology, and assessment. Anesth Analg. 2009;108:407–421.
6 Han M.K., McLaughlin V.V., Criner G.J., et al. Pulmonary diseases and the heart. Circulation. 2007;916:2992–3005.
7 Inglessis I., Shin J.T., Lepore J.J., et al. Hemodynamic effects of inhaled nitric oxide in right ventricular myocardial infarction and septic shock. J Am Coll Cardiol. 2004;44:793–798.
8 McLaughlin V.V., McGoon M.D. Pulmonary arterial hypertension. Circulation. 2006;114:1417–1431.
9 Metha S., Hill N.S. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163:540–577.
10 Minai O.A., Chaouat A., Adnot S. Pulmonary hypertension in COPD: epidemiology, significance, and management: pulmonary vascular disease: the global perspective. Chest. 2010;137:39S–51S.
11 Oswald-Mammosser M., Weitzenblum E., Quoix E., et al. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest. 1995;107:1193–1198.
12 Piazza G., Goldhaber S.Z. Chronic thromboembolic pulmonary hypertension. N Engl J Med. 2011;364:351–360.
13 Scharf S.M., Iqbal M., Keller C., et al. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med. 2002;166:314–322.
14 Simonneau G., Robbins I.M., Beghetti M., et al. Updated classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–S54.
15 Stobierska-Dzierzek B., Awad H., Michler R.E. The evolving management of acute right-sided heart failure in cardiac transplant recipients. J Am Coll Cardiol. 2001;38:923–931.
16 Vizza C.D., Lynch J.P., Ochoa L.L., et al. Right and left ventricular dysfunction in patients with severe pulmonary disease. Chest. 1998;113:576–583.
[/level-membership-for-critical-care-medicine-category][not-level-membership-for-critical-care-medicine-category]
Chapter 23 Cor Pulmonale
2 What are the subtypes of cor pulmonale?
Cor pulmonale can be acute or chronic.
In acute cor pulmonale the afterload to the right ventricle can rise in a matter of minutes (e.g., massive pulmonary embolism) giving very little room for compensation. The result will be acute right ventricular dilatation and failure, its severity depending primarily on the degree of acute PA hypertension.
3 What is the pathophysiology of right ventricular failure?
Under normal conditions, the pulmonary circulation is a low-resistance circuit, and the right ventricle generates the same stroke volume as the left ventricle with end-systolic pressures that are just 20% to 25% of those in the left ventricle. The low pressure within the thin free wall of the right ventricle also allows myocardial perfusion to occur both in systole and in diastole. Because of its structure, similar to that of veins rather than arteries, the right ventricle accommodates well additional volume but not higher pressure. When pressure overload occurs acutely, the right ventricle can only dilate and, if the pressure is sufficiently elevated, fail. Chronically, in response to increased systolic workload the free wall of the right ventricle hypertrophies and becomes similar to the left ventricle. Laplace’s law helps explaining the evolution from hypertrophy to dilatation and failure (Fig. 23-1): In a thin-wall chamber, an increase in intraluminal pressure increases wall stress unless thickness increases or the internal radius decreases. As the right ventricle hypertrophies, myocardial perfusion becomes limited to diastole, making its myocardium more susceptible to ischemia, and thus leading to dilatation and failure.
4 What are the causes of cor pulmonale?
Any process that results in pulmonary hypertension can cause cor pulmonale. Pulmonary hypertension is defined as mean PA pressures > 20 mm Hg at rest or > 30 mm Hg with exercise. The most frequent cause of pulmonary hypertension and cor pulmonale is COPD, due to chronic hypoxemia. In COPD the degree of hypertension is generally moderate, and oxygen supplementation may be effective in relieving some of the pressure load to the right ventricle and delaying failure. Additional causes of cor pulmonale include chronic pulmonary thromboembolic disease, left-sided cardiac abnormalities, untreated obstructive sleep apnea (OSA), interstitial lung diseases, and primary pulmonary hypertension. A comprehensive classification of the diseases of the lung associated with PA hypertension and cor pulmonale is shown in Table 23-1.
Table 23-1 Classification of cor pulmonale according to causative factor
| Category | Example |
|---|---|
| Diseases affecting the air passages of the lung and alveoli | COPD Cystic fibrosis Infiltrative or granulomatous defects Idiopathic pulmonary fibrosis Sarcoidosis Pneumoconiosis Scleroderma Mixed connective tissue disease Systemic lupus erythematosus Rheumatoid arthritis Polymyositis Eosinophilic granulomatosis Radiation Malignant infiltration |
| Diseases affecting thoracic cage movement | Kyphoscoliosis Thoracoplasty Neuromuscular weakness Sleep apnea syndrome Idiopathic hypoventilation |
| Diseases affecting the pulmonary vasculature | Primary disease of the arterial wall Primary pulmonary hypertension Pulmonary arteritis Toxin-induced pulmonary hypertension Chronic liver disease Peripheral pulmonary stenosis |
| Thrombotic disorders | Sickle cell diseases Pulmonary microthrombi |
| Embolic disorders | Thromboembolism Tumor embolism Other embolic processes (amniotic fluid, air, fat) Schistosomiasis and other parasitic infections |
| Pressure on PAs | Mediastinal tumors Aneurysms Granulomata Fibrosis |
Modified from Rubin LJ, ed: Pulmonary Heart Disease. Boston, 1984, Martinus Nijhoff, p 4.
7 What are the signs and symptoms of cor pulmonale?
Symptoms of cor pulmonale include the following:
9 What are the electrocardiographic (ECG) findings associated with right ventricular hypertrophy?
Right axis deviation: QRS negative in lead I, positive in aVR
[/not-level-membership-for-critical-care-medicine-category]
