[level-membership-for-anesthesiology-category]
Consent and Information for Patients
CONSENT AS AN ACTIVE PROCESS
Information
There is no statute which clearly defines what information should be given to patients about anaesthesia, and different countries’ legal systems have taken slightly divergent views. The AAGBI guidance is shown in Table 19.1. It must be emphasized that the anaesthetist should adapt this to the individual patient and surgery. For instance, visual loss after prone surgery is a rare but significant procedure-related complication which is relevant to specific patients.
TABLE 19.1
AAGBI Guidance on Information Which Should be Provided to Patients Relating to Anaesthesia
 Generally what may be expected as part of the proposed anaesthetic technique. For example, fasting, the administration and effects of premedication, transfer from the ward to the anaesthetic room, cannula insertion, noninvasive monitoring, induction of general and/or local anaesthesia, monitoring throughout surgery by the anaesthetist, transfer to a recovery area, and return to the ward. Intraoperative and postoperative analgesia, fluids and antiemetic therapy should also be described.
Generally what may be expected as part of the proposed anaesthetic technique. For example, fasting, the administration and effects of premedication, transfer from the ward to the anaesthetic room, cannula insertion, noninvasive monitoring, induction of general and/or local anaesthesia, monitoring throughout surgery by the anaesthetist, transfer to a recovery area, and return to the ward. Intraoperative and postoperative analgesia, fluids and antiemetic therapy should also be described.

 Alternative anaesthetic techniques, where appropriate.
Alternative anaesthetic techniques, where appropriate.








 Techniques of a sensitive nature, such as the insertion of an analgesic suppository.
Techniques of a sensitive nature, such as the insertion of an analgesic suppository.
Communicating Risk
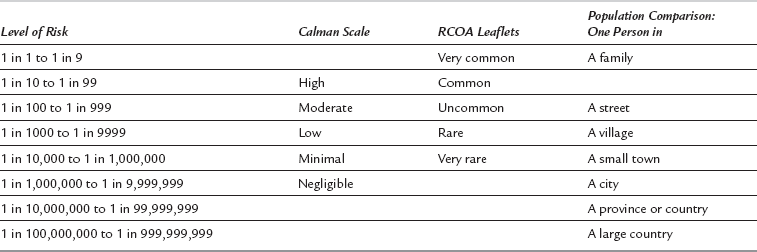
Patients prefer to be given numerical estimates of risk; doctors prefer to provide less precise qualitative estimates. Given the current state of evidence, neither is more accurate. The risk to the individual patient is usually unknown with sufficient precision. There is reasonable evidence that patients (and doctors) do not have sufficient understanding of probabilities for these to be used alone. Verbal likelihood scales are therefore most commonly used. The problem lies in the interpretation by anaesthetist and patient of the scale. ‘Never’ and ‘always’ are straightforward, but ‘common’, ‘rare’ and ‘unusual’ are subjective terms. Even within anaesthesia information systems, these are used differently. Drug information uses the ‘Calman’ scale; the Royal College of Anaesthetists (RCOA) uses a different scale. In order to provide more personal context, the population scale is sometimes used, comparing the risk to the number of people on a street, village, town, etc. (Table 19.2).
Capacity
1. Adult patients are assumed to have capacity unless it is established that they lack capacity. Capacity is the ability to (a) understand and remember the information and (b) use it to arrive at a decision.
2. Patients must be given a reasonable chance to demonstrate their capacity. A person’s lack of capacity cannot be assumed solely because they have taken drugs, alcohol or premedication, nor because they are making seemingly ‘wrong’ choices. In particular, the inability to communicate verbally does not imply a lack of capacity. Doctors (including anaesthetists) must make reasonable attempts to provide information for the patient so that they can decide on treatment options for themselves.
3. The treatment of adults without capacity must be in their best interests. This is a wider definition of best interests than solely medical best interests. Although generally more relevant to critical care than anaesthesia, the Act is clear that the treatment must be necessary, the least restrictive and in the patient’s wider best interests.
4. Patients may appoint proxy decision-makers with Lasting Power of Attorney (LPA). These individuals have the legal right to give or receive consent on behalf of a patient without capacity for carrying out or continuation of treatment. The exception is for life-sustaining treatment or treatment considered inappropriate by the doctor.



[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
Consent and Information for Patients
CONSENT AS AN ACTIVE PROCESS
Information
There is no statute which clearly defines what information should be given to patients about anaesthesia, and different countries’ legal systems have taken slightly divergent views. The AAGBI guidance is shown in Table 19.1. It must be emphasized that the anaesthetist should adapt this to the individual patient and surgery. For instance, visual loss after prone surgery is a rare but significant procedure-related complication which is relevant to specific patients.
TABLE 19.1
AAGBI Guidance on Information Which Should be Provided to Patients Relating to Anaesthesia
Generally what may be expected as part of the proposed anaesthetic technique. For example, fasting, the administration and effects of premedication, transfer from the ward to the anaesthetic room, cannula insertion, noninvasive monitoring, induction of general and/or local anaesthesia, monitoring throughout surgery by the anaesthetist, transfer to a recovery area, and return to the ward. Intraoperative and postoperative analgesia, fluids and antiemetic therapy should also be described.
Alternative anaesthetic techniques, where appropriate.
[/not-level-membership-for-anesthesiology-category]
