Congenital disorders and diseases secondarily involving the urinary tract
Congenital urinary tract disorders
Introduction
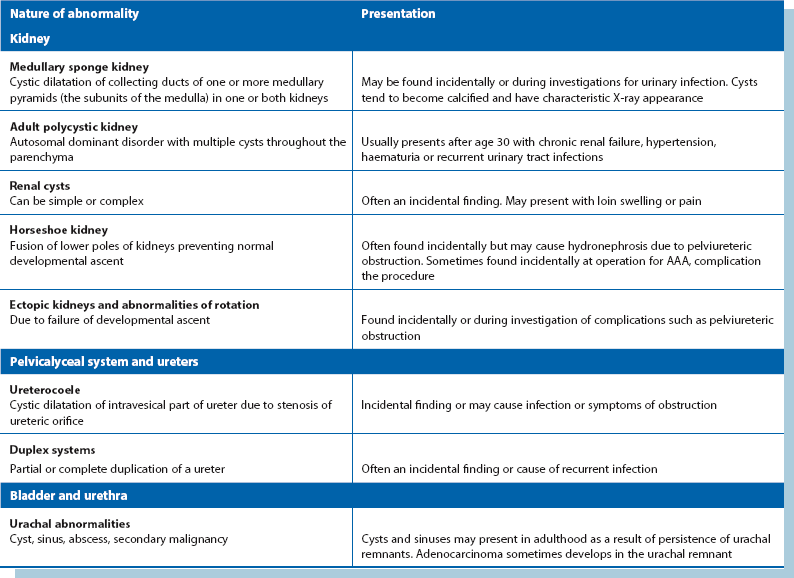
Serious congenital disorders of the kidneys and urinary tract nearly all present at birth or in early childhood (see Ch. 51). The exception is polycystic kidney which presents more commonly in adulthood. Less common abnormalities of the upper tract may interfere with normal flow dynamics and predispose to infection, e.g. duplex systems or medullary sponge kidney. Asymptomatic abnormalities such as unilateral renal agenesis, renal cysts or horseshoe kidney may be discovered incidentally during investigation or during surgery. With advancing age, a large proportion of the population develops benign renal cysts; these are usually of no clinical consequence. A summary of congenital disorders that present after childhood is given in Table 39.1.
Adult polycystic kidney disease (PCKD) is an autosomal dominant disorder characterised by bilateral multiple cysts of renal parenchyma (see Fig. 39.1). The cysts slowly expand, compressing the parenchyma, and may disrupt local control of blood pressure and eventually impair renal function. Polycystic kidneys have three main variants:

Fig. 39.1 Polycystic kidneys
IVU tomogram from a 52-year-old woman with hypertension and microscopic haematuria; both kidneys exhibit multiple lucent areas in the nephrogram representing cysts (arrowed) and the pelvicalyceal systems are slightly compressed
• A rare infantile form also affecting the liver; affected children often die young
• A serious adult form manifesting in middle age with hypertension or progressive renal failure. It is the commonest cause of inherited renal failure. Kidneys can appear normal on ultrasound scanning up to about the age of 20
• A less serious adult form usually found incidentally in later life with almost normal renal function. Patients are usually hypertensive
Thus, adult polycystic kidney may present with hypertension or progressive chronic renal failure. The enlarged kidneys may cause loin pain or be discovered incidentally on abdominal examination. These kidneys are vulnerable to even minor trauma, and haematuria and urinary tract infections are common presentations.
Medullary sponge kidney
This is caused by cyst-like dilatation (ectasia) of the renal medulla collecting ducts and may affect one or both kidneys. Cysts tend to calcify, giving a characteristic radiographic appearance of streaky linear calcification of renal papillae (see Fig. 39.2). On excretion pyelography (IVU), tubular ectasia can be demonstrated as a ‘flare’ in the renal papilla. Marked degrees of medullary sponge kidney predispose to recurrent infection and stone formation because of intrarenal urine stasis but patients rarely present before adulthood. Minor degrees are often seen on IVU without causing symptoms.
Case History
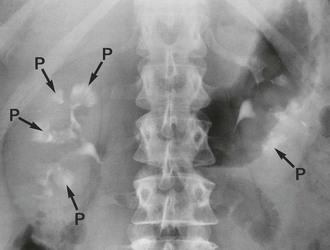
Fig. 39.2 Medullary sponge kidney
Bilateral medullary sponge kidney on an IVU from a 55-year-old woman with recurrent urinary tract infections; the renal papillae P has a typical ‘flared’ appearance and retains contrast because of the dilated collecting ducts. No radiopacity was visible on the control film although it can be seen in a considerable proportion of cases because of calcification in the ectatic ducts of the papillae
Duplex systems
The urinary collecting system may be duplicated to a greater or lesser extent. Duplication is usually complete proximally but may be incomplete distally. Lesser duplications are usually asymptomatic and discovered by chance on imaging. Complete duplex ureter is relatively common and may result in renal damage from infection, reflux or obstruction (see Fig. 39.3). The ureter draining the upper renal pole (upper moiety) is often inserted ectopically into the urethra (or vagina), resulting in continuous incontinence. Otherwise it joins the bladder ectopically below the orifice of the lower pole ureter. The orifice is often tightly stenosed, causing obstruction. This causes back pressure on the kidney and sometimes distal ureter dilatation known as a ureterocoele.
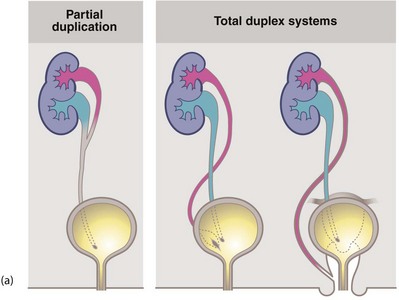
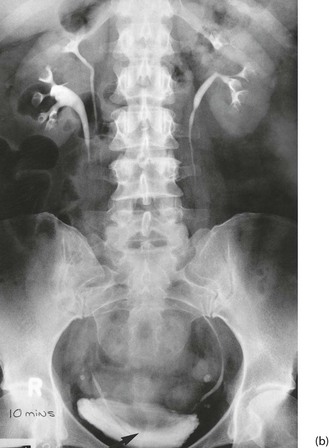
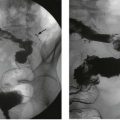
Fig. 39.3 Duplex systems
(a) Partial and total duplication. In a total duplex system (right), the ureter from the upper renal moiety may open into the urethra or vagina (i.e. wholly ectopic). Such an ectopic ureter causes continuous incontinence and presents early in life. Otherwise, it opens inferiorly in the bladder (centre). The orifice is often stenosed and a ureterocoele results (dilated lower end of ureter). Vesicoureteric reflux often occurs via the upper ureteric orifice back into the lower renal moiety.
(b) Duplication of the ureters on the right side; only one ureter can be seen passing as far as the bladder. The vesicoureteric junction is associated with a small, elongated ureterocoele (arrowed)
Horseshoe kidney
This abnormality is caused by embryological fusion of the two developing kidneys at their lower poles. Normal renal ascent in fetal life is prevented by the inferior mesenteric artery at the abdominal aorta, so the isthmus of the kidney comes to lie across the aorta at the third or fourth lumbar vertebral level. The condition is usually a chance finding on imaging (see Fig. 39.4) or else at abdominal aortic surgery, when it may cause serious operative difficulties. Horseshoe kidney is sometimes associated with pelviureteric junction obstruction, the symptoms of which may prompt the diagnosis. Occasionally, a horseshoe kidney first causes problems during pregnancy.

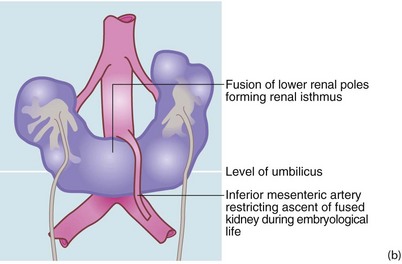
Fig. 39.4 Horseshoe kidney
Horseshoe kidney shown on IVU from a 51-year-old woman with recurrent urinary tract stones; the pelvicalyceal systems are oriented obliquely and converge inferiorly because the isthmus is stretched over the vertebral column. Each pelvis and ureter is more medially placed than normal and the whole renal mass lies much lower than would normal kidneys. The isthmus of a horseshoe kidney can rarely be demonstrated by IVU or ultrasound but can easily be imagined in this image
Renal ectopia and other renal abnormalities
Other renal abnormalities may be found incidentally. These include ectopic kidneys (see Fig. 39.5), rotational abnormalities, unilateral agenesis, aplasia or hyperplasia. These abnormalities may confuse the diagnosis and sometimes result in surgical mishap, e.g. excision of a pelvic kidney mistaken for an ovarian tumour. Note that transplanted kidneys are usually deliberately sited in the iliac fossa.

Fig. 39.5 Ectopic kidneys
(a) A 48-year-old woman with recurrent urinary tract infections; IVU shows abnormal pelvicalyceal systems P of bilateral pelvic kidneys.
(b) Right pelvic kidney discovered incidentally during arteriography for severe claudication. Its blood supply can be seen to arise from the distal aorta and iliac artery. The patient needed an aortofemoral bypass but when faced with the technical difficulties, agreed to conservative management of her claudication
Diseases secondarily involving the urinary tract
Retroperitoneal fibrosis (RPF)
Retroperitoneal fibrosis compresses both ureters, causing bilateral hydronephrosis and eventually renal failure. It can also be associated with inferior vena cava obstruction. Diagnosis is usually made on IVU or CT scanning which shows bilateral hydronephrosis (see Fig. 39.7). The fibrotic process also draws the ureters closer together in the midline. The ESR is characteristically elevated.