Chapter 3. Common postnatal problems
This chapter aims to address the commoner problems that paediatricians are called to review on the postnatal ward. It is by no means an exhaustive list of the problems that may occur and a standard textbook of neonatology should be consulted for more detailed information.
QUESTIONS
1. The following are contraindications to the BCG vaccination. Choose two correct answers:
a. Prematurity
b. Down syndrome
c. Babies born to HIV positive mothers
d. Babies with chronic lung disease
e. Family history of egg allergy
f. Family history of inflammatory bowel disease
g. Babies being treated with dexamethasone for chronic lung disease.
2. You are called to delivery suite to speak to some parents that have refused to let their baby have vitamin K. The father says that it is unsafe and causes cancer. Mum wishes to breast feed.
a. What are you going to tell them?
b. You find out that mother is on anticonvulsant medication. Does that affect what you say?
After you have discussed this with the family, the father then points out that there is a family history of glucose-6-phosphate dehydrogenase deficiency.
3. A baby is noted to have a sacral dimple on the postnatal check. On further examination, the dimple is found to be 2 cm above the anus and there is a small erythematous patch over the spine.
a. Are there any investigations you would do?
b. Why?
4. A mother was started on treatment for TB 7 days before delivery and her sputum for AFB is negative. Her baby is asymptomatic on examination. What management would be appropriate for the baby? Give two answers.
a. Isolate the baby from the mother
b. Encourage bottle feeding
c. Treat with isoniazid, rifampicin and pyrazinamide
d. Treat with isoniazid and rifampicin
e. Treat with isoniazid
f. Encourage breast feeding
g. Vaccinate the baby with BCG at birth
h. Vaccinate the baby with isoniazid-resistant BCG at three months
i. Do nothing.
5. You are called to see a term baby who is now 28 hours old. The baby has not passed meconium. The parents want to take their baby home and are becoming quite agitated. How do you manage the situation? Choose the most appropriate action.
a. Send baby home
b. Send baby home with clinic review in one week
c. Arrange urgent surgical review
d. Arrange contrast studies
e. Arrange plain abdominal x-ray
f. Keep in for observation.
6. A baby is noted on routine postnatal check to have absent red reflexes. Which of the following diagnoses need to be considered?
a. Congenital hypoparathyroidism
b. Retinopathy of prematurity without plus disease
c. Congenital hyperparathyroidism
d. Hallermann–Streiff syndrome
e. Persistence of the tunica vasculosa lentis
f. Retinal haemorrhage
g. Retinoblastoma
h. Lowe syndrome
i. Congenital glaucoma
j. CHARGE syndrome.
7. On a routine review of a baby on the neonatal unit, you noticed the baby has purulent discharge from both eyes. The baby is 4 days old. What is the most likely organism to cause this? Choose the best answer.
8.
i. Which of the following are risk factors for developmental dysplasia of the hip?
a. Male
b. Transverse lie
c. Previous affected sibling
d. Polyhydramnios
e. Intra-uterine growth retardation
f. First-born child
g. Torticollis.
ii. A mother reports that she required some form of harness when she was a baby. There have been two previous children who have been normal. The hips appear stable on examination. What action would you take?
9. A mother is known to have thyroid disease but has normal thyroid function tests. One of your SHOs organises for the baby to come back for thyroid function tests at 4 days of age. The results of these are as follows:
| Free T4 | 80 pmol/L |
| Total T4 | 300 pmol/L |
| TSH | 2 mU/L |
What action would you take?
a. No action and discharge the child
b. Repeat the tests in 2 weeks time
c. Repeat the test in 2 days time
d. Refer to paediatric endocrinology clinic
e. None of the above.
10. A baby is noted on postnatal check to have an undescended testicle (UDT). Which of the following statements are correct?
a. The majority of UDT will have descended successfully by 12 months of age
b. If still not descended at 12 months, 75% will descend by 36 months of age
c. Only a small minority are palpable
d. Early orchidopexy will preserve fertility in the majority
e. UDT requires orchidopexy to reduce the incidence of malignant change
f. UDT requires urgent review because of the risk of torsion
g. UDT usually responds well to hormonal therapy
h. UDT may be associated with urinary tract abnormalities.
12. The mother of a newborn baby girl informs you that her two previous babies, both boys, had pyloric stenosis, as did she. Which of the following statements are correct?
a. The chance of pyloric stenosis in this baby is no different to that for a baby with no family history
b. As this is a female infant, pyloric stenosis is less likely compared to a male infant
c. A test feed and abdominal ultrasound should be performed
d. Prophylactic pyloromyotomy is indicated
e. The baby should be fed normally
f. Treatment with anticholinergic drugs is now widely accepted as first-line management
g. In up to 7% of cases of pyloric stenosis there may be associated malformations.
13. A term baby is two weeks old, breast fed and thriving, with normal urine and stool colour. Examination is unremarkable but she is noticed to be moderately jaundiced. The bilirubin is 180 μmol/L, conjugated 10. Which of the following investigations should you carry out as part of your initial assessment?
a. Liver USS
b. HIDA scan
c. Haemoglobin
d. DCT
e. Urinalysis
f. Clinitest
g. Thyroid function tests
h. Red cell fragility
i. Blood cultures
j. UDPGT
k. Gene screen for Gilbert’s.
14. How would your approach differ if the conjugated bilirubin had been 40 μmol /L but with normal urine and stool colour?
15. A liver ultrasound scan suggests that bile ducts are present, and shows what appears to be an abnormally large gall bladder. What is the most likely diagnosis? Choose one answer.
a. Atypical biliary atresia
b. Duodenal web with biliary reflux
c. Normal variant
d. Inspissated bile
e. Diverticulum of the bile duct
f. Cystic dilatation of the common bile duct
g. Choledochocele.
16. A liver ultrasound examination is equivocal. A gall bladder is seen and the report states that the bile ducts were not clearly visualised but could have been obscured by the gall bladder. Which of the following is most appropriate? Choose one answer.
17. A baby is born to a mother who was noted to have significant anti-D levels during pregnancy. A cord blood sample was sent and you have just been informed that the cord bilirubin level was 180 μmol/L. The baby is now 4 hours old. You send a repeat blood sample for group and crossmatch, and Coombs’ test, and commence phototherapy. The following results are obtained within 2 hours:
| Bilirubin | 240 μmol/L |
| Hb | 12.5 g/dL (fragments seen suggestive of severe haemolysis) |
| Group A Rh positive | |
| Coombs strongly positive | |
Blood bank informs you that there are very abnormal antibodies in addition to Rhesus antibodies, and there may well be a delay of a few hours until blood is available.
Which of the following should be considered?
a. Encourage frequent breast feeding
b. Immunoglobulin infusion
c. Phenobarbitone
d. Albumin
e. High intensity daylight fluorescent bulb phototherapy
f. Intravenous fluids
g. Metalloporphyrin treatment
h. Withhold vitamin K to reduce risk of added oxidative damage
i. Liver USS to exclude biliary atresia.
18. A midwife calls you to review a baby with the following. The parents are extremely anxious about the baby? What are you going to tell them?
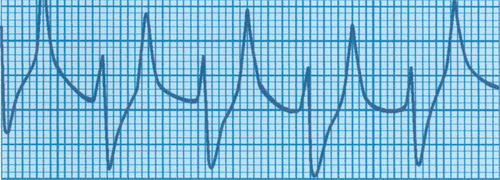 |
| Figure 3.1. |
ANSWER 1
a. Prematurity is not a contraindication for immunisation. It is commonly thought that babies under a certain weight should not be immunised – this is also not the case.
b. Down syndrome (or any stable neurological condition) is not a contraindication for immunisation. 1
c. Babies born to mothers with HIV must not be given BCG vaccine until the baby’s serology is confirmed to be negative. There have been reports of dissemination of BCG in HIV positive individuals. 1
d. Babies with chronic lung disease who are not receiving steroid treatment can receive the BCG vaccination. 1
e. A family history of egg allergy is not a contraindication for BCG vaccination. Egg allergy is only a problem with yellow fever and influenza vaccines. There is increasing evidence that MMR vaccine can be given even to children with a history of previous anaphylaxis after egg ingestion. 1
f. This is not contraindicated. There was previous speculation linking the MMR vaccine with inflammatory bowel disease but this evidence is not convincing. 1
g. Babies who are receiving immunosuppressive doses of steroids, greater than 300 μg/kg/day of dexamethasone for at least one week (which is equivalent to 2 mg/kg/day prednisolone), should not receive live vaccines. Administration of live vaccines should be postponed for at least 3 months after immunosuppressive treatment has stopped. 1
ANSWER 2
a. Vitamin K prevents vitamin K deficiency bleeding (VKDB – previously known as haemorrhagic disease of the newborn). Vitamin K is a fat soluble vitamin and humans have very low stores. Formula milk contains approximately 50μg/mL which is more than 20 times higher than in breast milk. All babies have very low vitamin stores at birth and milk provides the only source until bacterial activity in the gut provides a secondary source. Deficiency is associated with a small but significant risk of serious bleeding in the newborn baby which can be prevented by postnatal administration of vitamin K. The incidence of classical (2–7 day) VKDB is 0.25–1.7% in infants who have not received postnatal vitamin K and is reduced to 2.7/100,000 infants given 1 mg orally at birth, 1 week and 1 month. Bleeding associated with vitamin K deficiency may be from mucosal surfaces, such as the gastrointestinal tract, and reversed by later vitamin K treatment. It may also be intracranial and associated with severe and irreversible brain damage. Early (first 24 hours) and late (2–8 weeks, although presentation 15 weeks after delivery has been reported) disease are classically manifest as intracranial bleeding. 2
A paper published in 1992 suggested that babies who had received intramuscular vitamin K might be more likely to develop leukaemia. 3 Since then there have been more studies investigating the claim – a large analysis of data lead by the Department of Health concluded that solid tumours were no commoner in children given intramuscular vitamin K at birth. The situation with regard to childhood leukaemia is less clear and it was felt that the situation was unlikely to be clarified by the collection of further data as all infants were now receiving prophylaxis. The increased risk, if real, is small (unadjusted odds ratio 1.25:95% CI 1.06–1.46), and this could be due to the fact that those selected for different modes of prophylaxis already had different risk factors for the later development of cancer. It must be acknowledged that it has not been possible to prove that no risk exists. This could only be proven by a controlled study that would not be possible either technically or ethically.
b. Yes it does. Maternal anticonvulsants, particularly phenobarbitone, phenytoin and carbamazepine, are reported to be associated with a significantly increased risk of VKDB, both early and classical. However, the risk appears relatively small. In a study measuring prothrombin times in 137 babies whose mothers were receiving phenobarbitone, phenytoin or carbamazepine, only 14 out of 105 babies born to mothers with therapeutic drug levels had prothrombin times above the normal range and none had an overt bleeding tendency. All reverted to normal within two hours of administration of 1 mg of parenteral vitamin K. 4 Sodium valproate does not appear to be associated with any coagulation abnormalities.
c. Infants with glucose-6-phosphate dehydrogenase (G6PD) deficiency may experience acute haemolytic episodes after exposure to identifiable pharmaceutical agents. Vitamin K1 has a potential as an oxidant substance and is frequently included in the list of drugs to be used with caution in this condition. However, a study observing the haemolysis rates in red cells incubated with a vitamin K1 preparation could show no difference in haemolysis between G6PD deficient and control red cells. The authors concluded that red blood cells in G6PD deficiency are not at increased risk of oxidative damage from vitamin K. 5
ANSWER 3
a. Ultrasound of the spine and possible MRI.
b. Spinal dysraphism needs to be excluded.
Most infants with sacral dimples that fall within the natal cleft are healthy and have no associated abnormalities.‘High-risk’ dimples are defined as those that are deep, larger than 0.5 cm, more than 2.5 cm from the anus or associated with other cutaneous markers, such as a fat pad, hairy patch or erythematous macule. One report shows that 40% of babies with atypical dimples have sacral dysraphism. Spinal dysraphisms are disorders of the caudal neural tube. They include a variety of anomalies ranging from tethered cord (commonest) to diastomatomyelia (a longitudinal cleft in the spinal cord which may be due to either a cartilaginous, fibrous or osseous bar). Symptoms are variable, and signs include sensory and motor deficits of the limbs, bladder and bowel dysfunction.
ANSWER 4
Answers e and f are correct.
Mothers only need to be separated from their newborn babies if they are considered to have infectious TB. This is unlikely unless the diagnosis was made very close to the date of delivery. There is no reason to recommend bottle feeding as the concentration of anti-tuberculosis drugs in breast milk is too low to constitute any problems, and therefore breast feeding should be encouraged. The child cannot be infected by the mother through breast milk but it must be noted that drugs in breast milk do not offer effective treatment for TB disease in a nursing infant.
Current recommendations are that infants should receive treatment if the mother has had less than two weeks of treatment herself, following confirmation of tuberculosis. 8 This should take the form of isoniazid 5mg/kg and pyridoxine 5–10mg daily in the first instance. Babies should not receive BCG initially but should have a tuberculin test at 6–12 weeks of age. If this is negative, medications may be discontinued and BCG given. If the skin test is positive, appropriate medication should be given for a total of six months. Isoniazid-resistant BCG is not required. BCG is said to be effective at reducing the chance of a child developing active disease by around 70–80%.
ANSWER 5
Answer e is correct.
Term infants pass meconium at or shortly after birth with sources quoting 95–98.5% passing the first stool within 24 hours after birth and 100% passage within 48 hours in normal infants. Of those who have not passed stool a relatively small proportion may have a significant underlying problem (Hirschsprung’s disease affects around 1 in 5000 live births and these babies will represent approximately 1 in 250 of babies who have not passed meconium within the first 24 hours after birth).
The commonest cause of delayed passage of stool is meconium plug syndrome. In a radiological analysis of 133 infants with bowel obstruction, 66% had meconium plug syndrome, 20% had meconium ileus, and 18% had Hirschsprung’s. Meconium plug syndrome is associated with a number of conditions all of which produce abnormal motility of the neonatal bowel. These conditions include pregnancy-induced hypertension, diabetes, magnesium sulphate or other tocolytic agents, prematurity, sepsis, hypothyroidism and other metabolic conditions.
Preterm infants are more likely to experience delay in passage of first stool. For those weighing less than 1500g, just over 20% do not pass stool for 48 hours. For those weighing less than 1000g, the median time for first passage is the third day, with 10% still not having passed stool at 12 days. 9. and 10.
Most people would advocate an abdominal x-ray, with review by a paediatric surgeon if there is any abnormality on the x-ray. Some people may delay this for 48 hours, provided the infant remains well.
ANSWER 6
b. Retinopathy of prematurity without plus disease does not cause an absent red reflex. Retinal detachment can cause loss of a red reflex but plus disease will have been present in this situation.
c. Congenital hyperparathyroidism does not cause an absent red reflex.
d. Hallermann–Streiff syndrome, also known as oculomandibulodyscephaly with hypotrichosis syndrome, is one of many syndromes in which cataract is either a common or occasional finding. Cataracts occur in 94% of cases of Hallermann–Streiff.
e. Persistence of the tunica vasculosa lentis will cause an abnormal red reflex.
Persistence of the tunica vasculosa lentis may be a normal finding reflecting delayed regression of a normal fetal vascular structure. In the majority of infants, regression of these vessels is usually complete by 34 weeks gestation. However, in a number of cases it may be associated with congenital infections including rubella and CMV, and it may also be found in premature infants with active ROP. All these infants should be referred for ophthalmological review.
Persistent hyperplastic primary vitreous is another congenital abnormality that leads to a white pupil. This is due to the embryonic vitreous failing to regress. At birth, a plaque of white tissue can be seen behind the lens. It may be associated with cataract, glaucoma and microphthalmia. Again urgent ophthalmological review is indicated for early surgery.
f. Retinal haemorrhages are variably reported to occur in 2.5–50% of all births. Approximately 50% of these occur unilaterally. When severe and widespread the red reflex may not appear normal. Limited data suggest these regress within 10 days and are not associated with any significant long-term problems.
g. Retinoblastoma presents with leukocoria, glaucoma and strabismus. This is the most common intraocular primary tumour of childhood with an incidence of 1 in 20,000 live births. Although the average age of diagnosis is 18 months, diagnosis has been made prenatally and in the early postnatal period. Retinoblastoma needs to be excluded as early treatment leads to a better outcome. Disease confined to the eye has a 98% 5-year disease-free survival.
h. Lowe syndrome consists of cataract, renal tubular acidosis, glaucoma, aminoaciduria and glycosuria. Therefore, the red reflex will be absent or abnormal.
i. Congenital glaucoma leads to epiphoria, photophobia and blepharospasm, and affected babies present with a cloudy cornea and enlargement of the eye. When corneal clouding is marked it may not be possible to elicit a red reflex. Again the prognosis depends on the age of onset and time to diagnosis.
j. CHARGE syndrome is classically associated with a coloboma. Retinal coloboma is the most common and again the red reflex will be abnormal.
ANSWER 7
Answer a – Staphylococcus aureus is the most likely organism to cause conjunctivitis in this age group.
Conjunctivitis is a common neonatal infection occurring in 1–12% of all newborn infants and in a higher frequency in the developing world. The organisms responsible for causing conjunctivitis are isolated with a frequency given by the order of the organisms as listed in this question. Staphylococcus aureus is therefore the most common but may be present due to colonisation with no conjunctival reaction.
Chlamydia is becoming increasingly common and affects at least half of all infants born to a colonised mother. It is seen more often in the developing world. Infection may be associated with respiratory problems but is unlikely in this case as onset is usually 5–12 days after birth. It may start with one eye being affected and then becomes bilateral. Conventional cultures are negative and there is no response to usual treatment. The combination of these two factors usually prompts suspicion of Chlamydia. For the treatment of chlamydial ophthalmia or pneumonia, oral erythromycin and tetracycline eye drops for 2 weeks is recommended. However, in approximately 20–30% of infants, therapy will not eradicate the organism and the infant may require repeat treatment. There are a few published studies on the use of the new oral macrolide antibiotics, such as azithromycin, roxithromycin, or clarithromycin and these agents may be effective. 11. and 12.
Gonococcal conjunctivitis usually occurs earlier than four days, typically within 24 hours of delivery although late presentation has been reported. Copious purulent discharge is common and permanent damage may result. It is thus vital to make the diagnosis early and start treatment. A swab must be sent for both Gram stain and culture in enriched medium. Treatment used to be with systemic penicillin and penicillin eye drops, but now a single dose of intramuscular or intravenous ceftriaxone is used. 13
Pseudomonal ophthalmia is a rare cause of neonatal conjunctivitis but can cause extreme damage to the eye. It causes a systemic infection along with conjunctivitis, and therefore requires intravenous antibiotics with review from ophthalmologists.
Herpes simplex is the commonest virus causing conjunctivitis but is a rare isolate. All purulent conjunctivitis need screening for the causative organisms and treatment with appropriate anti-microbial or anti-viral therapy. If not treated, neonatal conjunctivitis can have severe and permanent ophthalmological sequelae.
ANSWER 8
i.c, f and g
Risk factors can be identified in 40% of infants with DDH. Of these risk factors the most commonly documented are:
Positive family history. If there is one affected parent, there is a risk of 12% for the newborn infant. This rises to 36% if there has been a previous affected child as well as an affected parent.
Female sex. Girls are five times more likely to be affected than boys.
Oligohydramnios and macrosomia. These are both risk factors due to intra-uterine compression.
Breech presentation. The incidence is increased 10-fold if the breech presents with extended knees.
DDH is associated with other anomalies including talipes and torticollis.
ii. This infant should be referred for screening by an orthopaedic specialist due to the increased risk of DDH in the infant, as described above.
The finding of stable hips on examination is not a reassurance. Studies have reported up to 50% of cases of DDH being missed on routine examination and other reports have shown that very experienced senior personnel may be unable to detect DDH even when they know it to be present. All babies should therefore have their hips checked at any routine examination.
ANSWER 9
Answer e is correct.
This infant is thyrotoxic and requires urgent admission and treatment. Any other action may be too late as this is potentially an extremely dangerous condition. Free T4 is very high (normal range after day 3, 14–28 pmol/L) as is the total T4 (normal range 1–4 weeks, 106–214 pmol/L). TSH is still measurable and may be very difficult to interpret in the early neonatal period. The upper limit of normal may be as high as 120 mU/L on day 1 and then falls to lie within the normal range of 0.3–10 mU by 7 days. A value within these ranges cannot be taken to exclude hyperthyroidism within the neonatal period.
Transplacental passage of thyroid stimulating antibodies due to maternal Graves’ disease is the commonest cause of neonatal thyrotoxicosis. When a mother is receiving thyroid suppressing drugs such as propylthiouracil, suppression of the features of hyperthyroidism may occur for several days following delivery. It is worth noting that symptoms may even develop when mothers have inactive Graves’ disease or are hypothyroid on thyroid replacement therapy. Abnormalities of thyroid function have been detected in as many as 16.5% of babies born to mothers with Graves’ disease although a significantly smaller proportion are clinically thyrotoxic.
Severe hyperthyroidism is associated with significant mortality and these infants should therefore be referred for specialist treatment immediately. Propylthiouracil or carbimazole may be needed to suppress thyroid function and propranolol given to control peripheral stimulatory effects. Severely affected infants may require more intense treatment.
ANSWER 10
a. True – undescended testicle occurs in approximately 3% of babies born at term and in up to 33% of babies born prematurely. By 12 months, the incidence has fallen to around 1% (two-thirds will have resolved by this time). One-third are bilateral.
c. False – at least two-thirds of unilateral undescended testicles are palpable, usually within the inguinal canal or distal to the external ring.
d. False – the effect of orchidopexy on fertility is still debated but there is no doubt that impaired fertility may persist in some infants despite surgery. Biopsy of the testes at the time of orchidopexy shows abnormal histology, and abnormal testosterone levels have also been demonstrated in association with abnormal function of testicular cell lines. Patients with a history of UDT have subnormal semen analysis but equivalent paternity rates if unilateral. Fertility is severely impaired with bilateral UDT giving paternity rates of approximately 50%, unaffected by early surgical correction.
e. False – studies have demonstrated an increased risk of testicular malignancy of 7.4–60-fold; 15–20% of tumours arise in the normally descended contralateral testis. Orchidopexy does not appear to reduce this risk but does facilitate detection.
f. False – there is an increased incidence of torsion in undescended testes but this an uncommon complication.
g. False – hormonal replacement is controversial and is not a routine part of management. Trials combining buserelin and HCG have been associated with an increased descent rate but this remains an experimental treatment.
h. True – UDT is associated with a number of anomalies including epididymal abnormalities, hypospadias, posterior urethral vales and anomalies of the upper urinary tract. There is some evidence to suggest that both UDT and the anomaly may be due to abnormalities in fetal testosterone levels.
ANSWER 11
a. You need to refer this baby for specialist assessment. Talipes occur with an incidence of 1 in 1000 live births, with a male to female ratio of 2–4:1; 50% are bilateral. External compression in utero is responsible for postural talipes, but in these cases the neutral position can normally be obtained by manipulation. Abnormalities in ligaments and tendons, neural dysfunction, abnormal muscle development and defects in the development of bones of the foot have been associated with more severe forms of talipes and intervention is required in these cases. Treatment should begin as early as is practically possible and thus early referral is important. Stretching exercises should be commenced and continued. In more severe cases or those failing to respond to conservative treatment, serial plaster casts are required followed by tenotomy and prolonged splinting. Failure to respond to this treatment may require more complex surgical procedures.
b. In the long term, although functional recovery is good and only a small number require salvage surgery, the majority will have a foot that is not morphologically normal. It must be appreciated that the condition does not just affect the foot but the whole lower limb as a unit and a small calf and foot are normal features. There will commonly be some residual functional deficit, which only major surgery could possibly correct. This degree of surgical intervention is not felt to be warranted for the extra gain obtained.
ANSWER 12
a. False – pyloric stenosis occurs in 1–3% of live births. If a mother has had this condition, the incidence is 19% in male offspring and 7% in female offspring. It only occurs in 5% of boys and 2.5% of girls when the father was affected. It is 15 times more likely to occur in siblings of affected infants. It is frequently said to be commoner in first-born male offspring but this is disputed. The risk is lower with increased maternal age, higher maternal education and low birth weight. 14
b. True – the male to female ratio of 4:1 remains constant despite varying estimates of incidence.
c. False – these are not indicated in the absence of symptoms.
d. False – this has never been described.
e. True – there is no evidence to suggest that manipulation of feeding regimes may influence onset of symptoms.
f. False – atropine treatment has been shown to be effective in small studies. Treatment results in a decrease in pyloric muscle thickness and in projectile vomiting. Although this has been reported in several studies, in both human and veterinary practice, it has not achieved widespread acceptance. 15
g. True – major associations are malrotation, obstructive uropathy and oesophageal atresia. Other anomalies associated with pyloric stenosis include hiatus hernia and a deficiency in hepatic glucuronyl transferase activity similar to that seen in Gilbert’s syndrome.
ANSWER 13
a. False – in the absence of a significantly elevated conjugated bilirubin, liver USS is not indicated.
b. False – as above.
c. True – assessment of haemoglobin with a full blood count and a screen would be a useful investigation at this stage.
d. False – this may be indicated in secondary assessment if haemolysis is thought to be a significant component.
e. True – to rule out infection which may present as prolonged jaundice.
f. True – to exclude galactosaemia.
g. True – this is normally recommended but every infant will have had a Guthrie test to rule out hypothyroidism. There is no evidence to suggest that this test misses infants who have developed unconjugated jaundice.
h. False – conditions such as elliptocytosis and spherocytosis can cause unconjugated hyperbilirubinaemia. However, both are rare, and unlikely to be relevant in the absence of other family history or evidence of haemolysis.
j. False – UDPGT levels are used to exclude Crigler–Najjar syndrome, which even in its mild form is associated with severe jaundice and is difficult to treat.
k. False – although this test is possible, the condition is mild and self-limiting, and is generally not thought to warrant specific screening.
ANSWER 14
A conjugated bilirubinaemia greater than 25–30 μmol/L or 10% of total serum bilirubin is said to be significant.
Although pale stools and dark urine are characteristic of established conjugated jaundice, they may not be seen in the first 3–4 weeks after birth and therefore cannot be taken as definite indication of non-obstructive causes. Other causes of prolonged jaundice should be considered including alpha-1-anti-trypsin deficiency, cystic fibrosis, congenital infection, amino acidaemias, congenital hypopituitarism and biliary atresia.
ANSWER 15
Answer f is correct.
Cystic dilatation of the common bile duct, diverticulum of the bile duct and choledochocele with intrahepatic extension are all types of choledochal cyst. Of these, the commonest is cystic dilatation of the common bile duct. Choledochal cysts are four times more likely to found in girls compared to boys, and usually present within the first 10 years of life. In children, the features of abdominal pain, jaundice and abdominal mass only occur in one-third. In the case under discussion, the bile ducts are present and therefore the proximal biliary ductal system is either normal or enlarged. This is in contrast to the findings in biliary atresia where the bile ducts may be difficult to visualise. There may be substantial distal obstruction of the biliary tract in various forms of choledochal cysts.
ANSWER 16
Answer c is most appropriate.
This baby could have biliary atresia and there is very good evidence that the efficacy of surgical treatment decreases progressively with time. Biliary atresia involves progressive obliteration and sclerosis of bile ducts, and a major determinant of satisfactory outcome following porto-enterostomy is the patient’s age at operation. In one series reporting outcome for 131 infants, long-term survival rate was 46% if operated on within the first 2.5 months after birth, compared with 24% for those where surgery was later than this. 16
Other answers:
a. False – you have not excluded biliary atresia with these investigations and to leave for a further 4 weeks is not appropriate.
d. False.
e. False – though a HIDA scan is indicated, it would be more appropriate for referral to the specialist team who will continue the management of the baby, and organise further warranted investigations.
ANSWER 17
a. False – adequate hydration is essential and although breast milk is not contraindicated, it is not sensible to rely upon breast feeding to maintain this. Feed volumes during early postnatal breast feeding are very variable and hydration may be relatively poor. Furthermore, breast feeding will compromise phototherapy, which in this situation should be continuous and at maximum efficacy.
b. True – treatment of severe Rhesus or ABO isoimmunisation with high dose intravenous immunoglobulin has been shown to significantly reduce the need for exchange transfusion, duration of phototherapy and length of hospital stay. A single 0.5g/kg dose on day one is effective. 17
c. False – phenobarbitone may increase the rate of bilirubin conjugation by induction of hepatic enzymes. Treatment of mothers antenatally, and of babies postnatally, may result in a significant reduction in serum bilirubin levels. Since first reported in 1968, barbiturates have frequently been used in pregnancy and the neonatal period, but the lack of specificity of action and the significant risk of adverse side effects (depression of vitamin K clotting factors and respiratory depression) mean that current recommendations are that this form of treatment should only be used in exceptional circumstance when no other effective treatment modalities are available.
d. False – bilirubin is transported in the plasma tightly bound to albumin and the portion that is unbound, or loosely bound, can more readily leave the intravascular space and cross the intact blood–brain barrier. Elevations in the levels of unbound bilirubin (UB) have been associated with kernicterus in sick preterm newborns. Although it is acknowledged that albumin is important for bilirubin binding, there is no consensus as to whether routine administration of albumin is indicated in hyperbilirubinaemia. In infants who are hypoalbuminaemic, it seems prudent to make sure albumin levels are in the normal range to improve bilirubin binding and thus potentially decrease the passage of bilirubin across the blood–brain barrier causing damage. However, there is no evidence that raising albumin levels into a supra-normal range has added benefit.
The American Academy of Pediatrics states that the risk of bilirubin encephalopathy is unlikely to be a simple function of the total serum bilirubin level or the concentration of UB but is more likely a combination of both. 18
e. False – daylight fluorescent bulbs provide suboptimal benefit. Light of a wavelength between 425 and 475nm is thought to be most effective, and light in the blue region of the spectrum is thus most commonly used. Daylight tubes emit light at wavelengths of 300–700nm but do not have a higher output in the blue spectrum. Green light may also be effective. Although the wavelength of green light is outside the optimal range, it penetrates further into the skin and may be more efficient at conversion of bilirubin to lumirubin than blue light. These bulbs are available but are not widely used. The minimal effective irradiance of phototherapy is 5 microwatts/cm 2/nm with reported increase in effectiveness up to 40 microwatts/cm 2/nm. This will be influenced by the nature of the phototherapy unit and by the distance from the infant.
f. True – adequate hydration is essential in the early postnatal period, and intravenous fluids may be the only way of ensuring this occurs.
g. False – the use of synthetic metalloporphyrins has been shown to be extremely effective in the management of jaundice in both preterm and term infants. These act through competitive inhibition of haem oxygenase and have been shown to reduce the need for exchange transfusion and the length of phototherapy. Although efficacy has been demonstrated, data on long-term safety is awaited. These products are not currently available in the UK but are available in the USA.
h. False – vitamin K should be given immediately after birth.
i. False – at this stage no radiological investigations are indicated unless the conjugated bilirubin is extremely high. This is unlikely in Rhesus disease.
ANSWER 18
Mongolian blue spots are flat birthmarks with blue-grey pigmentation, usually on the base of the spine, the buttocks and back and even sometimes on the ankles or wrists. The distinctive skin discoloration is due to the deep placement of the pigment and results from entrapment of melanocytes in the dermis during their migration from the neural crest into the epidermis
They are extremely common especially in Asian, East Indian, African and Latino heritage. They may be seen in about 10% of Caucasians and up to 90% of African–Americans. They typically disappear spontaneously within four years but can persist for life. No sex predilection is reported.
They commonly appear at birth or shortly after birth and look like bruises. They must therefore be documented well in the notes and parents should be made aware that they are present and that they are of no consequence. However they should be aware that others may still see them as bruises and raise concerns.
Several associations have been documented, e.g. cleft lip, melanoma, Hunter’s syndrome. There is no long-term morbidity or mortality associated with them when an isolated finding.
REFERENCES
1. Department of Health, The Green Book – Immunisation against infectious disease. ( 2006)DoH, London.
2. Hey, E, Vitamin K – what, why, and when, Arch Dis Child Fetal Neonatal Ed 88 (2003) F80–F83.
3. Golding, J; Greenwood, R; Birmingham, K, Childhood cancer, intramuscular vitamin K, and pethidine given during labour, BMJ 305 (1992) 341–346.
4. Hey, E, Effect of maternal anticonvulsant treatment on neonatal blood coagulation, Arch Dis Child 81 (1999) F208–F210.
5. Kaplan, M; Waisman, D; Mazor, D, Effect of vitamin K1 on glucose-6-phosphate dehydrogenase deficient neonatal erythrocytes in vitro, Arch Dis Child Fetal Neonatal Ed 79 (1998) F218–F220.
6. Kriss, VM; Dessai, NS, Occult spinal dysraphism in neonates: assessment of high-risk cutaneous stigmata on sonography, Am J Radiol 171 (1998) 1687–1692.
7. Higgins, JC; Axelsen, F, Simple dimple rule for sacral dimples, Am Fam Phys 65 (12) ( 2002;) 2435.
8. Health Protection Agency. Pregnancy and tuberculosis, guidance for clinicians. HPA, London, 2006
9. Fletcher, MA, Physical diagnosis in neonatology. ( 1998)Lippincott-Raven, New York.
10. Ashcroft, K, Pediatric surgery. ( 2000)WB Saunders, Philadelphia.
11. Darville, T, Chlamydia trachomatis infections in neonates and young children, Semin Pediatr Infect Dis 16 (4) ( 2005) 235–244.
12. Zar, HJ, Neonatal chlamydial infections: prevention and treatment, Paediatr Drugs 7 (2) ( 2005) 103–110.
13. Centers for Disease Control and Prevention. MMWR Recommendations and Reports. 2002;51:1–78
14. Applegate, MS; Druschel, CM, The epidemiology of infantile hypertrophic pyloric stenosis in New York State, 1983 to 1990, Arch Pediatr Adolesc Med 149 (1995) 1123–1129.
15. Kawahara, H; Imura, K; Nishikawa, M, Intravenous atropine treatment in infantile hypertrophic pyloric stenosis, Arch Dis Child 87 (2002) 71–74.
16. Grosfeld, JL; Fitzgerald, JF; Predaina, R, The efficacy of hepatoportoenterostomy in biliary atresia, Surgery 106 (1989) 692–701.
17. Gottstein, R; Cooke, RW, Systematic review of intravenous immunoglobulin in haemolytic disease of the newborn, Arch Dis Child Fetal Neonatal Ed 88 (2003) F6–F10.
18. Subcommittee on Hyperbilirubinemia, Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation, Pediatrics 114 (2004) 297–316.