CNS neoplasia II
Special situations
This chapter deals with pituitary tumours, some less common tumour presentations and some inherited syndromes with a particular predisposition to developing CNS tumours.
Pituitary tumours (common)
Clinical features
These include endocrine malfunction, visual disturbance and headache.
Headache is a late feature and may reflect bony erosion or hydrocephalus.
Investigations
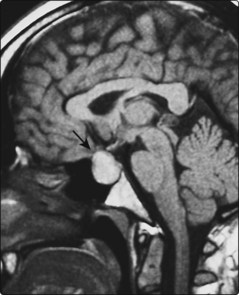
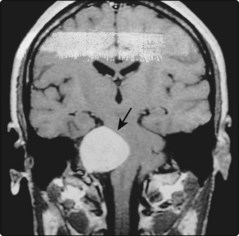
A highly elevated serum prolactin level (>4000 mU/l (normal <400)) implies a prolactinoma. More moderate elevations may be seen with other pituitary tumours that block the inhibition of prolactin release by dopamine. The tumours and their relation to other structures, especially the optic chiasm, are best seen on MRI (Fig. 1) but may also be seen on a CT scan with dedicated pituitary views. Endocrine assessment may be required, for example thyroid function, adrenal function, follicle-stimulating hormone and luteinizing hormone.
Cerebellopontine angle tumours (rare)
Pineal region tumours (rare)
These tumours present with visual disturbance and headache and Parinaud’s syndrome, characterized by failure of upgaze, eyelid retraction, dilated unreactive pupils, convergence–retraction nystagmus (on attempted convergence, all extraocular muscles contract, pulling the globe back into the orbit), hydrocephalus and papilloedema.
Other tumours
Numerous eponymous syndromes are described for tumours at the skull base. They present with pain and associated cranial nerve deficits, depending on the location of the lesion. Neurofibromas and Schwannomas, meningiomas and bony metastases or direct invasion by adenocarcinoma of the nasopharynx can all present this way. The differential diagnosis is from chronic meningitis (p. 98), osteomyelitis and inflammatory processes, for example sarcoidosis or Tolosa–Hunt syndrome.
Special situations
Inherited tumour syndromes
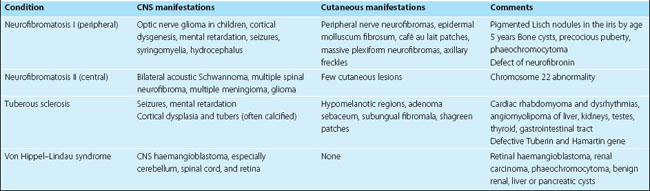
A variety of inherited diseases present with nervous system tumours, some with typical skin abnormalities (Table 1). They are rare. Most are inherited as autosomal dominant traits. The genetic locus of some of these conditions has been characterized but the pathophysiology is not yet understood.
Paraneoplastic syndromes
The nervous system is especially susceptible to non-metastatic manifestations of malignancy (Table 2). In some cases, humoral factors have been demonstrated, for example antibodies to Purkinje cells of the cerebellum in paraneoplastic cerebellar disorders, but it is not always clear if they are pathogenic. Certain tumours are particularly prone to causing these syndromes, especially small cell bronchial carcinoma, breast and female genital tract carcinoma and lymphoma. Paraneoplastic syndromes affecting other parts of the nervous system include: subacute myelopathy, retinopathy, stiff person syndrome and Lambert–Eaton myasthenic syndrome.
| Syndrome | Clinical features | Comments |
|---|---|---|
| Cerebellar degeneration |




