Clinical examination of the wrist, thumb and hand

Referred pain
History
• What is the problem? The patient describes the symptoms that are experienced in the wrist, thumb, hand or fingers. They are variable and may include pain, paraesthesia, numbness and weakness.
• How did it start? Was there an injury? Especially when a capsular pattern is found during the examination, the possibility of a fracture must be considered.
• Or did it start after particular exertion? Most ligamentous, muscular or tendinous lesions result from overuse. The symptoms may have started spontaneously, as usually happens in arthrotic or arthritic disorders.
• How has the problem developed? Because of the distal localization of the lesion, its evolution can only be judged in terms of the intensity of the symptoms, or by their appearance or disappearance, but not by reference of the symptoms.
Inspection
The typical articular deformities of arthrotic or arthritic changes in the joints are well known.
Functional examination
The wrist, thumb and hand are examined using 21 tests (Box 20.1).
The distal radioulnar joint
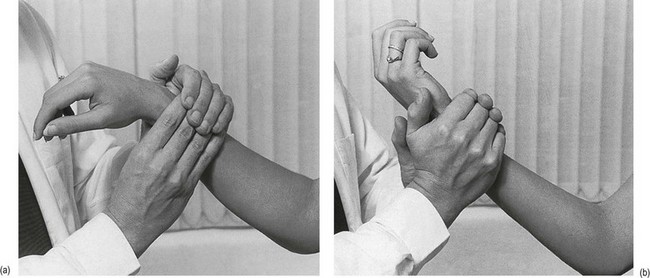
Passive pronation
The patient holds the elbow in 90° flexion. The examiner grasps the patient’s forearm just proximally to the wrist with both hands. The heel of the contralateral hand is placed on the palmar aspect of the ulna, the fingers of the other hand at the dorsal aspect of the radius. Pronation is performed by a simultaneous movement of both hands (Fig. 20.1a).
The wrist
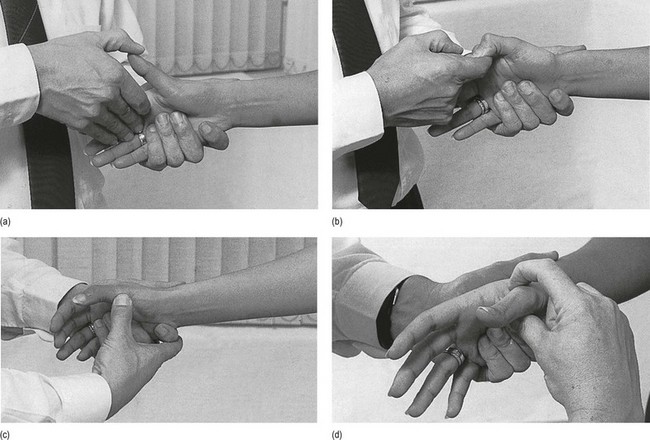
Passive movements (Fig. 20.2)
The normal end-feel of flexion and extension is capsular (elastic). If these movements are positive, the examiner must be able to tell whether the condition is of the capsular or the non-capsular type (see Ch. 23).
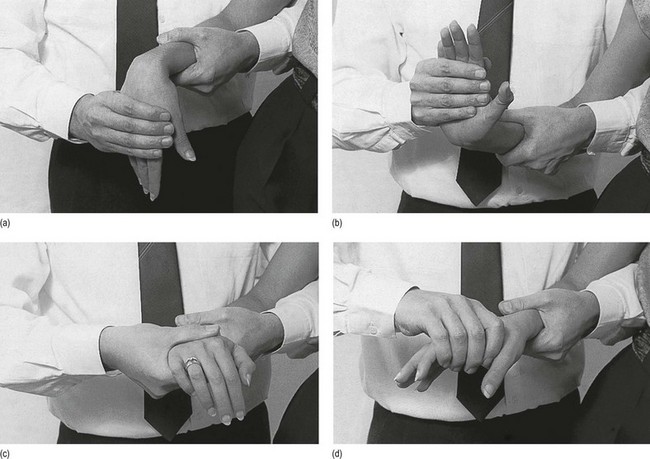
Passive flexion
The patient holds the elbow flexed at a right angle. The examiner takes hold of the patient’s forearm with the contralateral hand, in order to achieve good fixation. With the other hand, the patient’s hand is grasped and the wrist is flexed to the end of its range. The movement stretches the structures on the dorsal aspect of the wrist (ligaments, tendons) and pinches some structures on the palmar aspect (Fig. 20.2a).
Passive extension
Using the same grip, the examiner can bring the wrist into extension. Extension stretches the palmar tissues and pinches other tissues dorsally (Fig. 20.2b).
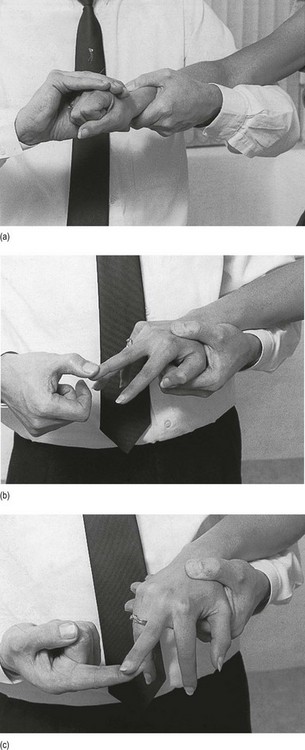
Resisted movements
For the resisted tests (Fig. 20.3) the patient’s elbow is kept in extension. This puts more stress on the contractile structures of the wrist and makes it possible to detect even the slightest tendinous and muscular lesions.
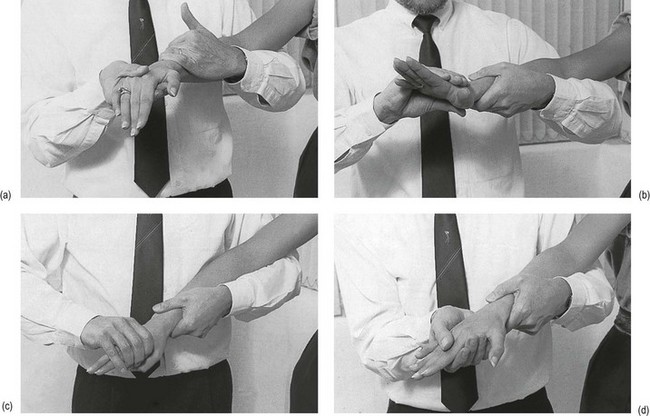
Resisted flexion
This test examines the flexors of the wrist and fingers – the flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis and profundus (Fig. 20.3a).
Resisted extension
This tests the extensors of the wrist and fingers – the extensor carpi radialis longus, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum communis, extensor indicis proprius and extensor digiti minimi (Fig. 20.3b).
The thumb
Passive movement
Backwards movement during extension
The patient flexes the elbow to a right angle and presents the hand with the palm upwards. The examiner takes hold of it with the ipsilateral hand and fixes it. With the other hand the thumb is brought into extension. Then the thumb is moved backwards so as to stretch the anterior part of the capsule of the trapezium–first metacarpal joint (Fig. 20.4).
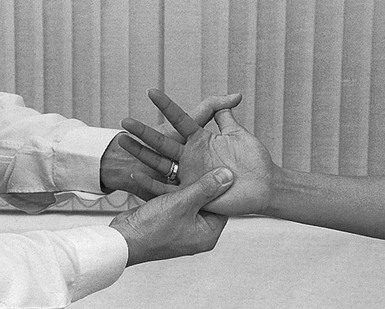
Fig 20.4 Passive movement of the thumb.
Resisted movements (Fig. 20.5)
Resisted extension
The patient presents the hand with the thumb upwards and it is fixed by the examiner’s contralateral hand. Resistance is then applied with the thumb of the other hand at the dorsal aspect of the distal phalanx. Extension tests the extensors of the thumb – the extensor pollicis longus and extensor pollicis brevis (Fig. 20.5a).
Resisted flexion
Resistance is applied to the palmar aspect of the distal phalanx of the patient’s thumb and tests the flexors of the thumb – the flexor pollicis longus and brevis (Fig. 20.5b).
The intrinsic muscles of the hand: dorsal and palmar interossei
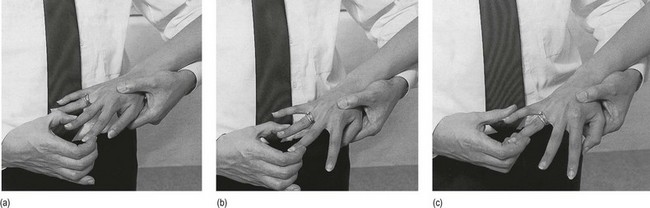
Squeezing with the index and middle fingers
The patient presents the hand in the horizontal position with the dorsal aspect upwards. The examiner puts an index finger between the patient’s index (II) and middle (III) fingers and asks the patient to squeeze it, so testing the palmar interosseus of the index finger and the dorsal radial interosseus of the middle finger (Fig. 20.6a).

Squeezing with the middle and ring fingers
The examiner’s finger is squeezed between the patient’s middle (III) and ring (IV) fingers. The examiner carries out the test as before, with the finger between the patient’s middle and ring fingers, so testing the dorsal ulnar interosseus of the middle finger and the palmar interosseus of the ring finger (Fig. 20.6b).
Squeezing with the ring and little fingers
The examiner’s finger is squeezed between the patient’s ring (IV) and little (V) fingers. The dorsal interosseus of the ring finger and the palmar interosseus of the little finger are tested (Fig. 20.6c).
Resisted separation of the index and middle fingers
The examiner resists the separation of the patient’s fingers at the distal phalanges, which tests the dorsal interosseus of the index finger and the dorsal ulnar interosseus of the middle finger (Fig. 20.7a).
Accessory tests
These tests (Fig. 20.8) are not part of the standard examination. They are only done when there is a need for more information about the patient’s problem.
Resisted extension of the wrist with the fingers held actively flexed
The patient is asked to flex the fingers and to press the fingertips in the palm of the hand. In this position resisted extension of the wrist is repeated (Fig. 20.8a).
Examination of the fingers
This examination (summarized in Box 20.3) is performed only when the patient clearly presents with a problem in the fingers.
Passive movements
• Flexion: with one hand the examiner fixes the proximal bone and with the other at the distal bone the joint is brought into flexion.
• Extension: with one hand the examiner fixes the proximal bone and with the other at the distal bone the joint is brought back to the starting position. Extension is usually not possible, except in very mobile or hypermobile individuals.
• Rotation in one direction: with one hand the examiner fixes the proximal bone. The other takes hold of the distal bone, brings the joint into slight flexion and rotates it in one direction. Very little movement is possible.
• Rotation in the opposite direction: the same manœuvre is performed but this time the rotation goes in the opposite direction.
Resisted movements
• Flexion: with one hand the examiner takes hold of the patient’s wrist and hand; the other is used to supply resistance against the patient’s attempt to flex the finger. Resistance is supplied at the palmar aspect of the distal phalanx.
• Extension: the examiner again fixes the patient’s wrist and hand. With the other hand at the distal phalanx the patient’s attempt to extend the finger is resisted.

