[level-membership-for-pediatrics-category]
Chapter 409 Chylothorax
Etiology
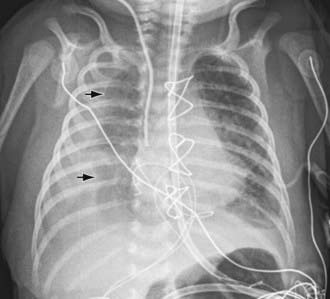
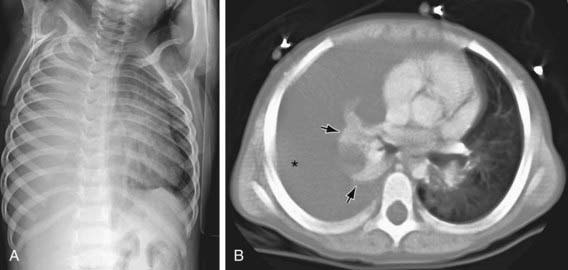
Chylothorax in children occurs most frequently because of thoracic duct injury as a complication of cardiothoracic surgery (Fig. 409-1). Other cases are associated with chest injury (Fig. 409-2) or with primary or metastatic intrathoracic malignancy (Fig. 409-3), particularly lymphoma. In newborns, rapidly increased venous pressure during delivery may lead to thoracic duct rupture. Less common causes include lymphangiomatosis; restrictive pulmonary diseases; thrombosis of the duct, superior vena cava, or subclavian vein; tuberculosis or histoplasmosis; and congenital anomalies of the lymphatic system (Fig. 409-4). Refractory chylothorax in the fetus has been associated with a missense mutation in integrin aα9. Chylothorax can occur in trauma and child abuse (Chapter 37). It is important to establish the etiology, because treatment varies with the cause. In some patients, no specific cause is identified.


Anderst JD. Chylothorax and child abuse. Pediatr Crit Care Med. 2007;8:394-396.
Bellini C, Boccardo F, Campisi C, et al. Lymphatic dysplasias in newborns and children: the role of lymphoscintigraphy. J Pediatr. 2008;152:587-589.
Cleveland K, Zook D, Harvey K, et al. Massive chylothorax in small babies. J Pediatr Surg. 2009;44:546-550.
Epaud R, Dubern B, Larroquet M, et al. Therapeutic strategies for idiopathic chylothorax. J Pediatr Surg. 2008;43:461-465.
Helin RD, Angeles ST, Bhat R. Octreotide therapy for chylothorax in infants and children: a brief review. Pediatr Crit Care Med. 2006;7:576-579.
Ma GC, Liu CS, Chang SP, et al. A recurrent ITGA9 missense mutation in human fetuses with severe chylothorax. Prenat Diagn. 2008;28:1057-1063.
Panthongviriyakul C, Bines JE. Post-operative chylothorax in children: an evidence-based management algorithm. J Paediatr Child Health. 2008;44:716-721.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
Chapter 409 Chylothorax
Etiology
Chylothorax in children occurs most frequently because of thoracic duct injury as a complication of cardiothoracic surgery (Fig. 409-1). Other cases are associated with chest injury (Fig. 409-2) or with primary or metastatic intrathoracic malignancy (Fig. 409-3), particularly lymphoma. In newborns, rapidly increased venous pressure during delivery may lead to thoracic duct rupture. Less common causes include lymphangiomatosis; restrictive pulmonary diseases; thrombosis of the duct, superior vena cava, or subclavian vein; tuberculosis or histoplasmosis; and congenital anomalies of the lymphatic system (Fig. 409-4). Refractory chylothorax in the fetus has been associated with a missense mutation in integrin aα9. Chylothorax can occur in trauma and child abuse (Chapter 37). It is important to establish the etiology, because treatment varies with the cause. In some patients, no specific cause is identified.
[/not-level-membership-for-pediatrics-category]
