[level-membership-for-surgery-category]Chapter 60
Chronic Venous Insufficiency
Deep Vein Valve Reconstruction
Michael C. Dalsing
Chronic venous insufficiency (CVI) can be asymptomatic or advance to a state of chronic, unrelenting venous ulceration. Skin changes such as hyperpigmentation consistent with CVI of the lower extremity have been reported in 6 to 7 million U.S. citizens, with progression to venous ulceration occurring in up to 2%.1–3 It is estimated that the cost of venous ulcer care alone is more than $1 billion annually.4 The excellent early success of ulcer healing with compression is marred by the risk of recurrence in up to 40% of compliant patients but approaching 100% in noncompliant patients.5,6 Treating all superficial and perforator vein insufficiency can reduce the recurrence risk, but it still is noted in up to 33% of patients with primary deep CVI and 70% of those with the postthrombotic syndrome. These facts demonstrate the importance of deep venous disease in the pathophysiologic process of CVI.7 Deep venous obstructive disease in combination with venous insufficiency has been noted in up to 55% of patients with CVI, especially in those with the most severe symptoms.8 Correcting iliac obstruction while ignoring the deep venous insufficiency can result in a long-term ulcer-free rate of nearly 60%.9 What patients remain are a select but finite cohort with chronic deep venous insufficiency who will benefit from valve reconstruction.
Pathogenesis
Etiology
Rarely patients are observed with congenital absence of lower extremity venous valves, venous aplasia or dysplasia.10 More commonly patients with primary venous insufficiency have either floppy, redundant, elongated valve cusps or an enlarged venous diameter, both of which prevent normal valve cusp apposition.11–14 In these cases, there is no apparent inciting event that caused the anatomic changes observed. As a consequence of these pathologic changes, spontaneously with standing or with additional stresses, reflux occurs in the affected valves. Except in the case of aplasia or dysplasia, in-situ tightening (repair) of the structurally intact valve can render it competent and functional.
Secondary venous insufficiency is often the result of acute deep venous thrombosis (DVT) and in 40% to 70% of all affected patients may be the cause of chronic deep venous valvular incompetence.11,15–17 The resulting inflammation and scarring with or without recanalization can cause foreshortening and fibrosis of the valve leaflets, small perforations, or valve adhesion and luminal narrowing.11 The valves are generally so damaged that in-situ repair is not feasible. The options remaining to prevent complete system reflux are transplantation of a competent valve from a distant location, transposition of the incompetent venous system to a position distal to a local competent valve, or the use of less traditional valve substitutes.
This standard differentiation between “primary” and “secondary” (postthrombotic) venous disease has been challenged by clinical imaging studies and by direct observation of the veins and valves at surgery. The simultaneous occurrence of both pathologic processes within the same patient is a clinical observation made decades ago.18 During attempted surgical repair of venous valve reflux, 6 of 11 excised veins demonstrated typical postthrombotic pathologic changes, but nonthrombotic phlebosclerosis was noted in the remaining 5.11 Phlebosclerosis was defined as vein wall thickening or fibrosis at the valve station or thickening of the valve cusps or intima (or both). One theory suggested to explain the thickened yet preserved normal valve architecture is that primary reflux with the associated sustained high venous wall pressure might cause the pathologic picture. DVT could also be the cause with rapid resolution of venous thrombi, an event documented by investigators studying acute DVT,19 allowing the involved valves to escape the severe damage usually associated with thrombosis. Alternatively, the valve itself may not be directly involved in the thrombotic process. Venous reflux has been documented proximal to an isolated distal thrombosis.19–21 In this case, the fibrotic process in the vein wall may involve the valve station only during thrombus resolution; the resultant thickened, noncompliant vein wall could cause the cusps to become floppy by virtue of a decrease in wall diameter.11 The valve remains architecturally intact, thin, and compliant and can be made competent by standard reefing of the cusps.
Hemodynamics
To realize the goal of controlling lower limb venous hypertension, correction of deep axial reflux proximal to the calf and ankle area is required (see Chapters 11 and 12). If one disregards this axiom, most commonly by ignoring profunda femoris vein reflux, isolated femoral vein valve reconstruction will be clinically unsuccessful because the offending hemodynamic effects will not be altered.22 Alternatively, when the profunda system is competent, repair of femoral vein incompetence does improve lower limb venous hemodynamics by preventing total axial reflux.22,23 In some cases of femoral vein thrombosis with occlusion, there is tremendous dilatation of the profunda femoris vein such that repair of valvular reflux in this vein will adequately reverse overall pathologic venous hemodynamics (Fig. 60-1).24 An alternative method of correcting significant axial reflux when both femoral systems are incompetent is to position a competent valve in the popliteal vein.25–27 At least one investigator has performed multiple tibial vein valve repairs to accomplish the same goal.28

Diagnostic Evaluation
History and Physical Examination
Patients with CVI may present initially with dependent edema, leg fatigue, itching, telangiectases, a feeling of overall fullness, or any combination thereof. Progression in severity may be noted by the presence of varicose veins, increasing pain, intractable edema, and skin changes (such as eczema, cellulitis, hyperpigmentation, lipodermatosclerosis, and stasis ulcers). A careful history should take note of previous episodes of DVT, known hypercoagulable conditions, and any limitations in physical and occupational activity resulting from venous insufficiency. In addition, the physical examination can eliminate other causes of the presenting signs and symptoms, such as ischemic ulcers, diabetic ulcers, dermatologic disorders, and even skin or soft tissue cancer. Each patient should ultimately be stratified according to the CEAP system to clearly define the venous disease present, which will allow the formation of a focused and appropriate management strategy.29 Candidates for deep venous valvular reconstruction typically have class 5/6 disease or disabling symptoms, such as severe edema (C4). An in-depth extension of the clinical classification (Venous Clinical Severity Score) provides a quantification of disease severity and is a useful evaluation tool to determine a patient’s response to treatment.30 Quality of life surveys provide an estimation of the impact of venous disease on the patient’s life and the effect that therapy has on the patient’s overall well-being.31 Application of these surveys before and after surgery will demonstrate those patients most improved by the intervention.
Noninvasive Evaluation
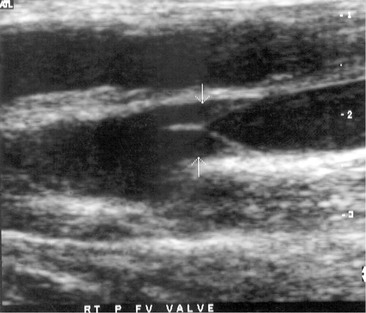
The noninvasive evaluation of patients with chronic deep venous insufficiency begins with a complete venous duplex study (see Chapter 18). It is essential to clarify the extent and anatomic location of all venous disease (specific veins can be imaged to determine the precise location of reflux), and it will provide some indication of the etiology (congenital, primary, or secondary) and aid in determining the pathophysiologic mechanism (reflux, obstruction, or both) of the disease present. The imaging is often so clear that venous valve cusps can be seen moving in the venous stream (Fig. 60-2). Insufficiency within any segment of the deep venous system is defined as a prolonged reflux time through the valve after a provocative test. A reflux time of longer than 0.5 second is considered abnormal in the tibial and deep femoral veins but is somewhat longer, more than 1 second, for the femoral and popliteal veins.32 Venous obstruction is seen as thickened, scarred, and constricted veins or valves with poor flow and diminished augmentation after distal or proximal compression. Respiratory variation can be lost as a consequence of local disease or proximal obstruction or stenosis. Similar imaging and spectral analysis will determine obstruction or, more commonly, insufficiency of the superficial and perforator veins. This is all the diagnostic evaluation needed if only the superficial and perforator veins are found to be pathologic.
I use air plethysmography (see Chapter 17) to provide an overall quantification of the impact of deep venous insufficiency before deep venous valvular reconstruction and to provide some insight into the effectiveness of treatment. Currently, this diagnostic modality is used for specific indications or as a research tool only.33
Invasive Evaluation
For patients being considered for deep venous valvular repair, venography is required for precise operative planning. Ascending venography (see Chapter 20) defines deep venous system anatomy, helps eliminate obvious obstruction as an etiologic factor, and provides a means of selecting the most disease-free portion of the incompetent and postthrombotic venous system when valve transplantation is an option.11,34 Ambulatory venous pressure has been shown to correlate with the presence of venous ulceration and is one method available to estimate the degree of venous hypertension.35 A venous reflux time of less than 20 seconds confirms that valvular reflux is present in the limb being evaluated. Intravenous hemodynamic study, although useful, can be provided by less invasive means, so it is not always a component of an ascending venographic evaluation. Similarly, the practice of directly measuring lower limb intravenous pressure before and after thigh cuff occlusion has not proved to be a reliable determinant of significant proximal venous occlusion.11,34,36 The importance of significant iliac vein occlusive disease is determined best by the use of intravenous ultrasonography.36 Descending venography (see Chapter 20) is used to determine valve leaflet integrity, anatomic location, and extent or degree of reflux (Fig. 60-3).37 Assessment of the competence of the profunda femoris venous system in addition to the femoral system is imperative because it will affect the choice and location of venous valve repair and the potential for valve transposition.27,38,39 Descending venography does not have absolute accuracy in determining the presence or absence of a normal valve.11 Raju and colleagues reported that descending venography had a false-positive rate of 11% (a valve considered present was absent at surgery) and false-negative rate of 25% (a valve thought absent was present on direct inspection) when direct inspection at operation was the “gold standard.”11 However, when it is combined with a well-performed venous duplex examination, it is the best method available to determine preoperatively whether in-situ reconstruction will be possible.

Treatment Selection
Natural History and Patient Risk Assessment
The natural history of patients being considered for deep venous valvular repair has generally been extensive because all less invasive interventions to solve the patient’s problems have been attempted and have failed. With the traditional approach of treating all superficial and perforator disease first regardless of the status of the deep system, about 33% of patients with primary deep venous incompetence and 70% of those with postthrombotic syndrome will experience ulcer recurrence, thus emphasizing that deep venous disease must eventually be treated in select patients.7 Separate investigators have added external valvuloplasty of the femoral vein to high ligation and saphenous vein stripping to improve the clinical durability in advanced disease, with gratifying results.40,41 Iliac vein occlusive disease has been treated with the knowledge that symptoms may resolve in about 60% of patients.9 For the remaining 40%, deep venous reflux will require intervention to alleviate symptoms.
Patient risk assessment must follow the tenets of any open operative intervention (see Chapter 31). Hemodynamic instability from the operation is minimal, but because the operative intervention is time-consuming and technically challenging, general anesthesia is typically required. An acceptable cardiac and pulmonary status is required. Systemic infection should be treated before intervention. Systemic disease that might have an impact on healing, such as collagen vascular disease, diabetes, chronic renal insufficiency, or lower extremity arterial occlusive disease, will influence the surgeon’s decision to perform a venous intervention.42 These conditions are relative contraindications to aggressive venous intervention unless they are corrected or medically optimized before venous valve repair.
Treatment Options
The treatment options available to correct deep venous valvular reflux are determined by the availability of complete and structurally intact venous valves. Selection of the operative technique when the valve cusps are architecturally preserved is somewhat determined by the degree of cusp prolapse, the surgeon’s preference, and the reported long-term success. In the case of valve prolapse secondary to vein wall dilatation only, vasospasm alone may reestablish a competent valve, and in such cases simple external banding of the vein will provide a workable solution to prevent reflux.43 When wall dilatation with more pronounced cusp prolapse is present, external valvuloplasty will provide a way to decrease wall diameter, and the use of certain techniques will also enable reefing of the valve cusps into a functional position. With pronounced valve leaflet prolapse, internal valvuloplasty allows direct and extensive cusp shortening and reduction of wall diameter. When there is no identifiable valve structure within an incompetent system, two potential options are available. If a parallel axial system has a competent valve or one that can be made so, a transposition procedure is an option. When this is not feasible, valve transplantation of a competent valve from a distant location remains an option. Valve substitutes are being investigated, with some autogenous options showing promise. The quest for a percutaneous option has provided few answers to date. In some instances, intervention in two or more separate axial venous systems (e.g., the femoral and profunda femoris veins) or into the popliteal location will be required to prevent axial reflux into the calf and ankle soft tissues. Multiple valve repairs in the same incompetent axial system (e.g., two or more in the femoral vein) are being investigated in the hope of decreasing recurrent reflux and thus symptoms28,44–46; however, many surgeons have reported success when only one valve per incompetent system is repaired.
Surgical Treatment
Relevant Anatomy
The common femoral, profunda femoris, and femoral veins are covered by skin, soft tissue, and fascia in the groin and by the sartorius muscle more distally. More caudally, the femoral vein occupies the adductor [Hunter’s] canal, which places it deep to the sartorius and flanked by the vastus medialis and adductor longus fascia muscles. As the femoral vein exits the adductor canal, it is called the popliteal vein and lies between the heads of the gastrocnemius muscle distally but is covered only by skin, soft tissue, and fascia directly behind the knee. The anterior tibial veins lie in the anterior calf compartment deep to the anterior tibialis muscle. The posterior tibial and peroneal veins lie in the deep posterior compartment and are covered by the soleus and gastrocnemius muscles, which form the superficial posterior compartment.47
Valves are universally present in the paired tibial and peroneal veins, with 3 to 12 valves rather evenly distributed in each vein.48 The majority of popliteal veins (>90%) have one to three valves with a slight trend to be located more caudal in the leg.48 The femoral veins have one to five valves.48,49 The most constant valve occurring in about 90% of patients is found in the femoral vein 1 to 2 cm distal to joining the profunda femoris vein.48–50 In 88% of patients, the profunda femoris vein has one to four valves.48 The common femoral vein may (30%-50% of patients) have one or two valves within a few centimeters of the inguinal ligament.48–50
Operative Planning
In the event that an intact valve has been confirmed by preoperative duplex and venographic studies, most experienced surgeons choose the proximal femoral vein for valvuloplasty or to repair both the femoral and profunda femoris valves if both systems are incompetent. This decision is based on the ease of exposure, familiarity with the approach, and size of the veins available for repair. When both proximal femoral axial systems are incompetent, some have chosen repair of the popliteal vein valve, which is considered the “gateway” to the lower leg venous system. However, mid or distal femoral vein valves can be repaired if they are surgically accessible and amenable to valvuloplasty by virtue of retained architecture. As one proceeds down the venous system, vein diameters and valve leaflets become smaller and therefore more difficult to repair. Nevertheless, even tibial vein valves have been successfully repaired. If a transposition operation is planned, duplex ultrasound and descending venography must have identified the presence of a competent valve. Valve transplantation requires having identified a valve in the axillary or brachial vein by duplex ultrasonography or venography. Ligation of upper extremity veins is well tolerated. The optimal place for implantation into the lower extremity is into the least damaged vein segment available, which will prevent axial reflux into the calf area.
Prophylactic antibiotics are given during the procedure (e.g., first-generation cephalosporin) but are continued postoperatively for 2 or 3 days by most surgeons.41,44,51 Intraoperative heparin is commonly given when venous occlusion is required during valve repair; a typical dose is 2000 to 10,000 units, which is not generally reversed.38,41,44,51–53
Techniques
Overall Exposure
If reconstruction of the proximal femoral veins (femoral or profunda femoris) is the goal, a groin incision is made in the direction of the vessels to expose the first and second femoral valves.48 Further dissection through the fascia that lies beneath the sartorius muscle will expose the profunda femoris vein if necessary. After exposure of the valve targeted for repair and the adjoining segment of vein, the strip test should be performed to evaluate the competence of the valve This test entails milking blood antegrade past the valve while inflow is occluded, with subsequent application of retrograde pressure against the valve. Reflux is demonstrated by refilling of the vein distally. This incision may also provide exposure for valve transposition or transplantation, if it is required.
After identification of the valve station to be repaired, careful adventitial dissection to identify the valve attachment lines is useful.52 This dissection facilitates proper placement of the venotomy so as not to damage the valve leaflets, when required, and verifies that valve repair is feasible. A lack of valve attachment lines can signify destruction of the valve and suggests the need to consider techniques other than in-situ repair.52
In other situations, a more distal femoral, popliteal, or even tibial vein may be the desired location for valve repair or transplantation. In these situations, the medial exposure is much like that used for exposure of the like-named artery.47 The popliteal vein can be exposed through a posterior S-shaped incision, with the transverse incision made in the posterior knee crease to decrease the chance of scar contraction.47
Internal Valvuloplasty
For decades, the open method of direct valve cusp tightening (reefing) has been the mainstay for correction of primary deep venous valvular reflux. This technique involves venotomy and suturing of the elongated valve leaflets under direct visualization. The redundant valve cusps are plicated to the vein wall with interrupted 6 or 7-0 polypropylene suture to allow proper alignment and later coaptation of the cusps. Kistner in 1968 was the first to report success using a longitudinal venotomy extending through the valve commissure (Fig. 60-4A).54 Raju later described a supracommissural approach in which a transverse venotomy was performed at least 2.5 cm above the valve (Fig. 60-4B).55 Sottiurai described a combination approach in 1988 in which a supravalvular transverse venotomy with distal extension into the valve sinus (a T-shaped venotomy) was used (Fig. 60-4C).56 The “trap door” approach of Tripathi and Ktenidis (2001) involved two transverse incisions on the vein connected by a single vertical incision (Fig. 60-4D).57 Regardless of the approach, suturing of the valve leaflets remains essentially the same (Fig. 60-5). It is estimated that plication of approximately 20% of the length of the valve leaflet can generally restore competency to the valve in the majority of cases.58
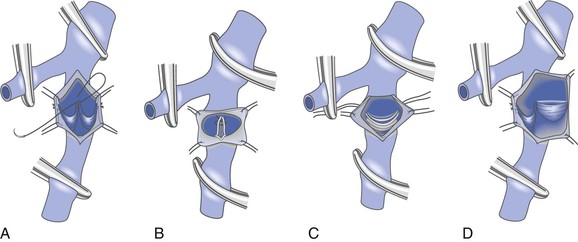
Figure 60-4 Internal valvuloplasty can be accomplished by a variety of techniques used to visualize the incompetent valve leaflets. A, Artist’s representation of the method first proposed by Kistner, in which he opens the vein through the anterior commissure. B, Representation of the method of Raju, who uses a supravalvular transverse venotomy to view the valve from above without incising through the valve commissural angle. C, Representation of the method of Sottiurai, who performs a supracommissural incision with extension toward a cusp sinus to improve visualization. D, Representation of the technique used by Tripathi, who uses a “trap door” incision to provide optimal visualization of the valve cusps for repair. The method of reefing the valve to reestablish a competent valve is essentially the same in each instance.
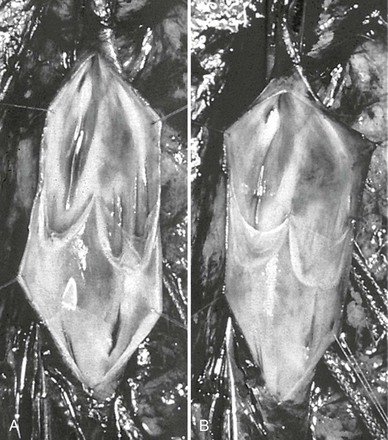
Figure 60-5 The method of Kistner is shown in these operative pictures before valvuloplasty (A) and after valvuloplasty (B). Note the laxity of the incompetent valve before intervention, whereas after reefing of the valve cusps, the normal architecture and tension are reestablished. (Courtesy Dr. Robert Kistner.)
External Valvuloplasty
The technique of external valvuloplasty was pioneered by Kistner and reported in 1990 (Fig. 60-6).59 This approach offers the advantage of valve repair without a venotomy. It is performed by placing interrupted sutures transmurally through the valve attachment lines, which on tying leaves a decreased commissural angle and a competent valve. Others have used a running suture to accomplish a similar effect.52 Both anterior repair and posterior repair can be performed. Another group of investigators combined angioscopy with limited anterior valve sinus plication by interrupted transmural sutures in 15 limbs and achieved improvement in clinical symptoms, hemodynamics, and competence as determined by descending venography.53,60
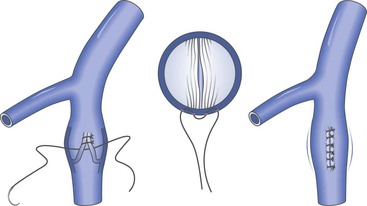
Figure 60-6 Artist’s rendition of the method of external valvuloplasty. The enlarged venous diameter results in valve incompetence. Note how the placement of sutures decreases the diameter of the venous wall but keeps the valve cusps from harm’s way. The sutures lie outside the vein lumen in this approach.
A modification of external valvuloplasty involves the transluminal placement of sutures to reef the valve leaflets and to narrow the vein wall, much like internal valvuloplasty but without opening the vein. Gloviczki and colleagues in 1991 reported using an angioscope to directly view the valve cusps during repair (Fig. 60-7).61 A side branch of the great saphenous vein allows introduction of the angioscope, which is then advanced above the appropriate femoral vein valve for optimal visualization. Interrupted external sutures are seen entering the venous lumen and can be precisely placed to sync up the cusps at the point of attachment on the vein wall. Closure of the valve attachment angle and simultaneous tightening of the valve cusps are realized. Raju contends that use of the angioscope is not necessary after a learning curve but concedes that excellent visualization of the valve is achieved when it is used.52 He believes that identifying the valve cusp externally with the use of adventitial dissection is critical to a technically successful repair and places his sutures as demonstrated in Figure 60-8 (transcommissural valvuloplasty).44 A continuous suture can also be used to accomplish this repair.41 Limited anterior plication, a modification of this method, involves anterior vein dissection and placement of a running mattress suture at the anterior commissure, which runs from a point 3 to 4 mm proximal to the angle of the valve cusp insertion lines up to the angle of the valve cusp insertion.62 About 3 mm of the vein wall is incorporated into the stitch to adequately approximate the cusps.62 Limited anterior plication was developed with the aim of decreasing vein dissection and potentially reducing the progressive dilatation of the postrepair vein that occurs after some cases of valvuloplasty.62 It has been used most commonly in conjunction with saphenous vein stripping and limited to the femoral vein valve station.
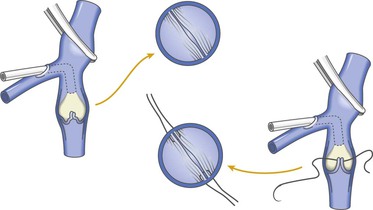
Figure 60-7 As an improvement to “blind” placement of sutures in the method of external valvuloplasty, the use of an angioscope as suggested by Gloviczki and coworkers allows precise suture placement within the vein lumen for actual tightening (reefing) of the valve cusps.
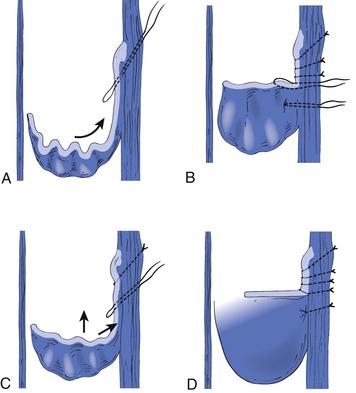
Figure 60-8 The initial through-and-through oblique transluminal suture placed at the commissural apex catches sagging leaflets and resuspends them. A to D, Transluminal sutures, with each successive suture biting deeper and less oblique than the suture above to pull up the valve, tighten the cusp edges, deepen the sinus, and appose the valve attachment lines. Each suture is tied before the next is placed. One or two of the most caudally placed sutures may actually pass through the body of the leaflet rather than through the edge, with no subsequent ill effects. (Redrawn from Raju S, et al: Transcommissural valvuloplasty: technique and results. J Vasc Surg 32:969-976, 2000.)
External Banding
This method has most commonly been used in cases in which dissection vasospasm renders an incompetent valve spontaneously competent. An external sleeve made of polyester (Dacron) or polytetrafluoroethylene is wrapped around the circumference of the vein at the site of the valve. It is tightened to reduce the size of the vein lumen until valve competence is achieved (Fig. 60-9). The sleeve is then anchored in place to the adventitia by sutures to avoid migration. A more aggressive approach of repairing valves that may not spontaneously become competent with simple dissection venoconstriction has been used by one investigator and involves placement of an external valvular stent made specifically for this indication (Venocuff II, Imthage, Sydney, NSW, Australia).51 It is Dacron-reinforced silicone with an adjustable diameter that has been found to be histologically superior to Dacron or polytetrafluoroethylene in animal experimentation. By serially reducing the vein diameter to 30% or less, the valves were rendered competent, but in the rare case when this did not occur, the solution was to go to another valve with the same technique. One report described the use of a spiral device called the Vedensky Spiral that screwed around the outside of the vein to decrease the vein diameter by approximately 30% with endoscopic confirmation of valve competence.63
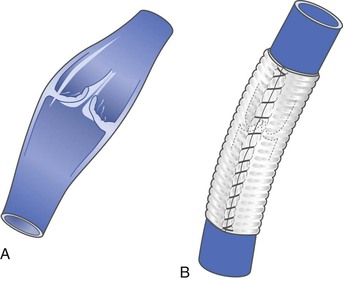
Figure 60-9 Artist’s depiction of external banding to prevent venous valvular incompetence in veins that become competent during the vasoconstriction that occurs at the time of operative dissection. Some surgeons use this technique to prevent dilatation after valve transplantation or other types of repair. A, Incompetent valve before banding. B, After banding, the valve is competent.
Several investigators have added an external band at the conclusion of the valvuloplasty operation (any type) to prevent delayed dilatation.41,44,64 Others have abandoned this approach because of concern for significant scarring and resulting valve failure.45,65
Valve Transplantation
Venous valve transplantation provides a technique that can be used when the valve cusps have been destroyed. This procedure was first described for use in humans by Taheri and colleagues in 1982.66 A 2- to 3-cm segment of upper extremity vein containing a competent valve (or one that can be made competent) is first removed. The incompetent femoral vein system is approached just below the takeoff of the profunda femoris vein, and the axillary vein segment is sutured in place after removal of an appropriate length of femoral vein. The proximal anastomosis is often accomplished first to confirm valve competency and to allow distention and lengthening of the vein or valve to facilitate the distal anastomosis (Fig. 60-10). In trabeculated postthrombotic veins, Raju and coworkers have described excision of intraluminal synechiae to create one lumen suitable for implantation and anastomoses.67 Interrupted sutures are preferred to avoid suture line stenosis.58 Valve competence is determined by the intraoperative strip test. An external sleeve can then be placed around the segment to prevent later dilatation of the segment.52,58,64 Because approximately 40% of axillary vein valves are incompetent at the time of explantation, bench repair may be required.52,58 However, more proximal or distal valves that are competent should be sought before resorting to this added surgical intervention. Should bench repair be necessary, the transcommissural external valvuloplasty technique appears to achieve better results than does the standard external valvuloplasty,52 and some experience and success have been achieved with internal valvuloplasty.68
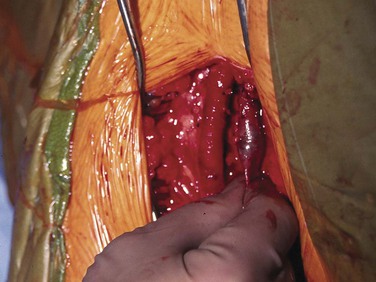
Figure 60-10 This intraoperative picture shows a valve transplant with cephalad anastomosis complete. Any fluid or blood was pushed forward from the distal vein past the valve and the valve is competent allowing vein elongation and therefore proper positioning of the distal anastomosis. A similar maneuver is performed when a “strip test” is used to confirm valve competence. During a “strip test” the vein distal to the valve is occluded (in this case by the surgeon’s fingers but may be by vascular clamp or forceps) and the blood is pushed or milked from the vein distal to the valve-containing vein segment. As blood is allowed to refill the vein, if the valve is competent, blood will not reflux and, therefore, not be present in the vein distal to the valve.
Valve Transposition
Another option in those without architecturally preserved valve leaflets is a valve transposition operation. If a single groin axial venous valve is spared from reflux, a transposition procedure can be performed by placing the incompetent venous system distal to the competent valve. Most commonly, the femoral system is incompetent and the profunda femoris valve remains competent. The incompetent femoral vein can be transected and reimplanted distal to the competent profunda femoris valve (see Fig. 60-11). Alternatively, the incompetent femoral system can be placed below a competent valve in the great saphenous vein. When the profunda femoris valves are incompetent, that segment can be placed distal to a competent valve in either the femoral vein or the great saphenous vein. A technique has also been described for transposition of an ipsilateral valve (competent great saphenous vein to the femoral vein and subsequent ligation of the femoral vein proximally yet distal to the takeoff of the profunda femoris vein) to escape problems with diameter mismatch.69

Postoperative Management
Pneumatic compression devices are applied postoperatively to decrease swelling and the risk of DVT.38,44,53,64,70 This may also increase flow through the valve repair when the patient is sedentary. Because therapeutic or low-dose intravenous heparin or low-molecular-weight heparin is generally administered postoperatively, closed drainage of wounds may be helpful to avoid hematoma formation. One investigator starts warfarin on postoperative day 1 with an initial target international normalized ratio of 2.0 to 2.5 for the first 6 weeks, then subsequently decreased to 1.7 to 2.0 until 4 months, at which point it is stopped.44 One suggested long-term regimen for anticoagulation in these patients is “minidose” warfarin, which involves the administration of daily doses of 1 to 2.5 mg.52,71 Others suggest prescribing oral anticoagulation at therapeutic levels (international normalized ratio of 2.5 to 3.0) for 3 months38,45,64,70,72 or 6 months.41 Adjustments to this regimen should be made to accommodate those with increased risk for thrombosis. Others have used little anticoagulation, but this was generally limited to other than open valvuloplasty.53,62 Although many surgeons encourage the use of compressive support after venous valve reconstruction, many patients do not comply and yet have experienced a good clinical response.11,18
Results
Complications and Initial Results
Valve repair procedures have low morbidity and low (<1%) mortality, with most reporting no associated mortality.40,41,44,45,52,62,64,73 Hematoma and seroma formation is seen in up to 15% of cases, with some expected variation according to the level of anticoagulation necessary.18,38,44,45,58,64,65,70 DVT occurs in less than 10% of cases in most series.18,38,44,51,52,58,64,65 This clinical experience may somewhat underestimate the actual incidence of DVT because in one series using aggressive venographic surveillance at 2 days postoperatively, a 20% rate of DVT was noted, but the clot was often not occlusive or extensive, nor did this event appear to have an impact on clinical results.70 An extensive review of essentially all modalities of venous valve repair noted the incidence of DVT to be 12.4% overall; it was only 6.7% in those with primary disease but 25.4% in patients with secondary deep venous insufficiency.45 Pulmonary embolism can occur but is very rare; in one series with in-depth reporting of results, it occurred in 1 of 129 patients.44 An aggressive approach using catheter-directed thrombolysis did result in complete resolution of thrombosis in 60% of cases (three of five cases) and even salvage of involved valve repairs in 50% of cases (one of two cases).44 Wound infections have been seen in 1% to 7% of cases.18,44,45,52,58,64 Patency and valve competency of all types of repairs within the perioperative period (30 days) are reported as excellent by most investigators. A few series report a less than 1% incidence of early failure.44,52 Valve leaflet trauma can occur, especially early in one’s clinical experience and especially during vertical venotomy, with seven cases reported by one investigator.45 These injuries were successfully repaired with 8-0 suture, and 57.1% of cases (four of seven cases) were competent at 2 years.
Late Results
Internal Valvuloplasty.
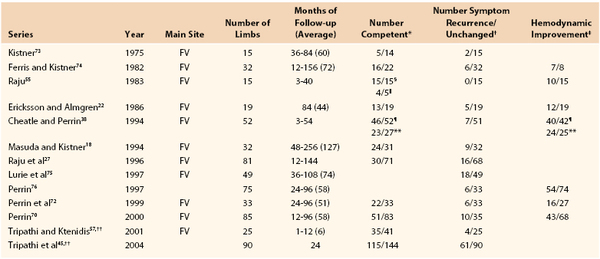
Kistner and colleagues have monitored their patients who required internal valvuloplasty for decades and have reported life-table results of clinical success (Fig. 60-12). Table 60-1 is a compilation of series reporting their success with internal valvuloplasty.* It confirms excellent clinical results in patients who otherwise have experienced unrelenting symptoms as a result of chronic deep venous insufficiency. Valves are competent in 60% to 70% of patients at 5 years in most series. In general, a patent and competent valve translates into clinical improvement, whereas recurrent reflux is associated with clinical failure. A similar comment can be made about all types of venous valvular reconstruction.
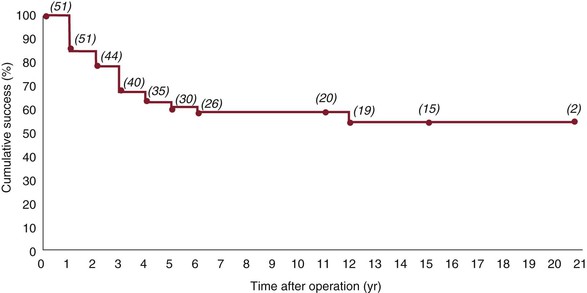
Figure 60-12 Cumulative clinical success rates for all limbs of patients with class 0 or 1 (as defined in the original article but comparable to higher CEAP clinical classifications) disease who have had a venous valve reconstruction. Numbers in parentheses represent total limbs at risk for each time interval. (Redrawn from Masuda EM, et al: Long-term results of venous valve reconstruction: a four- to twenty-one-year follow-up. J Vasc Surg 19:394, 1994.)
Table 60-1
Results of Internal Valvuloplasty
* Determined by phlebography, duplex ultrasonography, or both.
† Includes C3-6 (majority C5/6).
‡ Determined by plethysmography or intravenous pressure (preoperative versus postoperative findings).
§ Determined by ultrasonography.
‖ Determined by phlebography.
¶ Immediately after surgery.
** Twelve months after surgery.
†† More than one valve repair per limb.
FV, Femoral vein.
External Valvuloplasty.
The technique of external valvuloplasty involving the placement of transmural sutures to narrow the diameter of the vein wall may be a less durable repair than the more direct open valvuloplasty.27 Much of the current work involving isolated deep venous reflux surgery by various techniques of external valvuloplasty has involved the repair of multiple valves within the same axial system, which can confuse interpretation of the results. Raju’s group used the transcommissural technique to repair 179 valves in 141 limbs with a competence rate of 63% at 3 years and clinical improvement without recurrence in around 70% of cases, in addition to statistical improvement in various venous hemodynamics.44 Tripathi and colleagues reported an experience in which standard external valvuloplasty was used in the majority of cases. In 12 limbs, 19 repairs were performed with a competency rate of 31.6% (6 of 19) and an ulcer-free rate of 50% (6 of 12) at 2 years.45 One would surmise that six valves in six limbs were still functioning.
The addition of femoral vein external valvuloplasty to superficial saphenous surgery has been an interest of several investigators, probably because of the proximity of the proximal femoral valve during open surgery. Limited anterior plication has been used in combination with superficial venous intervention, and a 10-year follow-up demonstrated improved venous refilling time and decreased ambulatory venous pressure in patients with limited deep venous valvular incompetence.62 An investigation of standard femoral external valvuloplasty in addition to superficial saphenous stripping has demonstrated better clinical and hemodynamic results than achieved with superficial surgery alone.40 None of these patients had venous ulcers. At 3 years of follow-up, 90.9% of valves were competent and all parameters of venous hemodynamics and venous severity scores were statistically improved over those noted after stripping alone. The addition of external banding to external valvuloplasty supported the Chinese experience but suggested that the addition of an external band was statistically beneficial.41 More than 50% of their patients had venous ulcers currently or in the past. At 5 years, the competence rate of those without and with external banding was reported to be 48.5% and 69%, respectively (P = .04), with an ulcer-free rate of approximately 68% and 96% (P = .008). Venous hemodynamics was also significantly improved by 36 months.
External Banding.
The prosthetic sleeve method of valve repair has achieved acceptable results in selected patients with less advanced disease.27 A more aggressive approach involving the use of banding in patients with advanced disease in which venospasm did not necessarily result in a competent valve demonstrated the ability to achieve valve competence in a majority of cases.51 In 42 limbs, 125 valves were repaired, and the repairs were generally in the femoral vein (60) or popliteal vein (53). The investigators reported competence in 90% of patients at 86 months and significantly improved photoplethysmographic estimates of recovery time, but the surgeons did not report competency per valve site. Long-term ulcer healing rates were directly associated with the number of valves repaired: one, 51%; two, 65%; and three, 86%. Another group confined banding to the proximal femoral vein valve in patients with grade 3 or grade 4 reflux and only in those in whom the profunda femoris vein was competent. They reported a 78% competency rate and symptom relief at 50 months, but prevention of recurrent varicose veins was the target.77 It was difficult to interpret the Vedensky Spiral data, but overall the competence for standard bicuspid valves without a wide commissural angle was approximately 90% with a mean 2.4-year follow-up.78
Valve Transplantation.
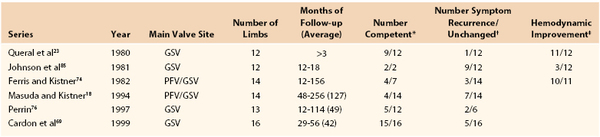
Table 60-2 provides a synopsis of the results that one can anticipate when valve transplantation is required to treat chronic deep venous valvular incompetence.25,26,55,76,79–83 Clinical improvement is seen in about 50% of patients, even at 8 years of follow-up, and it remains a viable option in cases in which valvuloplasty is not possible.15,58,84
Table 60-2
Results of Valve Transplantation
* Determined by phlebography, duplex ultrasonography, or both.
† Includes C3-6 (majority C5/6).
‡ Determined by plethysmography or intravenous pressure (preoperative versus postoperative findings).
§ More than one valve repair per limb.
FV, Femoral vein; POP, popliteal vein.
Valve Transposition.
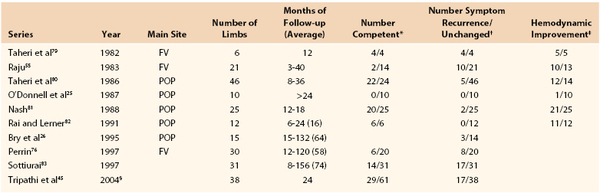
Table 60-3 tabulates the results of transposition operations.18,23,69,74,76,85 Good results with the technique of valve transposition have been observed in 40% to 50% of patients after 5 years of follow-up.18,23,69,74,76,84,85 The method of placing a large femoral system below a competent great saphenous valve with ligation to offset the size discrepancy has resulted in 55% of the patients being free of ulcers at 10 years.69
Multilevel Valve Reconstruction.
There is increasing evidence that multilevel valve reconstruction (more than one valve repair in the same axial system) does improve maintenance of valve competence in at least one of the repaired valves and, as a consequence, improves clinical outcome. Raju and his group have been advocates of this approach for some time.28,44 At 2 years, Tripathi and colleagues found that patients with primary reflux disease undergoing single-level valvuloplasty could expect a 59.4% valve competence rate and 54.7% ulcer healing rate, which was statistically different (P < .05) from multilevel repair, which demonstrated rates of 79.7% and 72.9%, respectively.45 A similar trend was noted in those requiring valve transplantation; valve competence and ulcer healing rates were 38.9% and 46.1%, respectively for single-level repairs versus 55.8% and 57% for multilevel repairs. Rosales and colleagues have accumulated data on external valvuloplasty that suggest improved clinical results, especially in CEAP class 4 patients, with the use of a multilevel (different locations in the same axial system) and multistation (more than one valve in the same location) technique, but statistical significance was not obtained and clear determination of valve competence was not provided.46 Lane and associates found that as the number of external banding repairs per axial system increased, so did long-term ulcer healing.51
Overview.
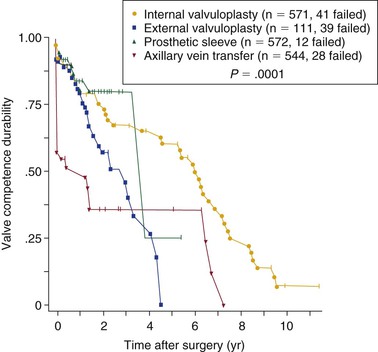
In general, patients with postthrombotic reflux tend to experience reduced healing rates and more recurrent venous ulcers than do those with a primary cause of reflux, as noted from the results of internal valvuloplasty (generally a primary cause) versus transplantation or a transposition operative approach. However, Raju and associates found little difference in the results of repair of postthrombotic and primary disease in their series.16,27 It is possible that this difference simply reflects a delay in the appearance of ulceration after valve failure. These same investigators reported a difference in valve competence based on the method of repair (Fig. 60-13). It would appear that there is decreasing durability as one progresses from internal valvuloplasty, to external valvuloplasty, and finally to the need for transplantation.
Follow-up
Monitoring and Management
A typical method of clinical follow-up includes physical examination at 6 weeks, 3 to 9 months, and then annually, but with considerable variability in the exact timing of visits.* During each visit, duplex Doppler ultrasound is performed to determine valve site patency and valve competence.† Noninvasive testing has generally replaced descending venography, which was often used in earlier series.18,53 Most surgeons include some type of hemodynamic assessment.‡ Some use a visual analogue pain score or assessment for swelling.44,62 Reclassification by the CEAP criteria, venous severity scoring, and use of quality of life assessment tools are encouraged to provide quantifiable parameters of clinical success.
Certainly, reoperative surgery can be difficult but is sometimes required.52 The best approach appears to be through a new incision remote from the original operative site. One optimal site is the femoral vein at the adductor canal because it is accessible and easy to work on. Raju and Hardy52 have found it difficult to perform popliteal valvuloplasty because of an often thick adventitial coat, which makes adventitial dissection difficult and therefore visualization of the valve commissures difficult.
Endovascular Treatment
There is an interest in repair or replacement of venous valves through a minimally invasive percutaneous endovascular approach. An autogenous vein-containing valve placed within a commercially available self-expanding stent that is delivered from a remote access site into the venous system of an animal model can remain open and functional for several weeks.86,87 Some histologic data from these studies suggest a potential compliance mismatch resulting from the metal exoskeleton/autogenous valve design. These designs have not reached clinical evaluation to date.
A balloon-expandable stent with a glutaraldehyde-preserved xenograft valve mounted within performed poorly when it was implanted into canine inferior venae cavae; all six occluded within 2 months.88 Glutaraldehyde-preserved allografts have fared somewhat better in the experimental model, with nearly a fourth patent and competent in early experimental follow-up.89 In a swine model, a percutaneously placed glutaraldehyde-preserved bovine venous segment with a contained valve has demonstrated good early results,90 and clinical investigation was begun.91 Thrombosis became an issue, and no further clinical investigation is ongoing.
A bioprosthetic, bicuspid, square stent-based venous valve has been developed and percutaneously placed in the external jugular vein of sheep in a feasibility study.92 The valve leaflets were made of small intestinal submucosa (SIS) attached to a metal frame, which aids in incorporation of the valve into the vein wall. It appears to be resistant to thrombosis and becomes repopulated with recipient endothelial cells after implantation in animals.92,93 Design changes have been required to aid in proper centering of the valve,94 and a finding of cusp thickening suggested a need to lengthen the valve cusps and thereby improve flow hemodynamics, which might aid in cusp cleansing and result in less turbulent flow. However, fibrosis of the SIS material with use in the clinical arena was recognized as a problem.95 None of the 15 clinically implanted valves was competent at 12 months.96 Retooling to incorporate an autogenous venous valve positioned within the unique metal stent design is being investigated, with fine preliminary success.97 There is also interest in seeding the original SIS with endothelial progenitor outgrowth cells, which can be isolated from the peripheral blood. Early experimental work demonstrates excellent ability of the seeded cells to remain attached to the SIS.98 Clinical investigation has yet to be reported.
The quest for a percutaneous prosthetic venous valve continues, with various designs proposed: a “sail” design,99 polyurethane fiber scaffolds fabricated by electrospinning and attached to a cobalt-chromium stent,100 and a “naturally open” valve design with impregnated anticoagulant compound.101 This is only a representative collection of such studies. Most demonstrate excellent hemodynamic performance, but there are few experimental data and currently no clinical experiences.
Venous Valve Substitutes
Valve substitutes could address difficulties in treating patients with deep venous valvular insufficiency who have no autogenous valves available for repair or transplantation. Various attempts have been studied experimentally without success: fresh allografts,102 umbilical vein molded into a valve,103 liquid Pellethane-molded valve,103 and platinum/pyrolyte-covered titanium valve.104,105 Glutaraldehyde-preserved xenografts have not proved successful in experimental or clinical series.88,89,91
Lyophilized allograft valve–containing vein segments appear to function after processing but have never been studied further.106 A cryopreserved venous valve–containing allograft initially studied in a canine model demonstrated promise.107 However, early results and longer clinical follow-up revealed poor patency rates and minimal clinical improvement.108,109 A cadaveric cryopreserved pulmonary monocusp patch (allograft) has been described as well; it achieved reasonable clinical results, but valve competence was not clearly defined in this small group of patients studied for a period of several years.110 Possibly, retention of a portion of the recipient vein wall (autogenous vein) helps explain the better results noted in this study than when the entire vein is replaced.111
A hybrid approach championed by Opie involves invaginating a cuboidal piece of the vein wall, still attached at its caudal edge, into the vein lumen with two sutures attached to the cephalad edge to prevent complete reflux and to aid in forming a monocusp valve. The opening in the vein wall is repaired with a specially designed and flexible expanded polytetrafluoroethylene patch (Atrium Medical). He reported no incompetent valves in 14 operations at 4 years and excellent clinical improvement.112 Investigators from Russia have reported an 80% clinical improvement and no recurrent reflux at 8 months of follow-up using this technique.113
Valves constructed by invaginating autogenous vein into itself by the method of Eiseman and Mallette have shown experimental promise but have not been studied clinically.114,115 However, use of autogenous tissue to reconstruct valves has been relatively successful in several select series. A small series of patients who underwent de novo valve reconstruction procedures have been studied.52 These procedures involve the use of a piece of autogenous vein as a donor. Semilunar cusps are fashioned out of donor vein after trimming of the adventitia and part of the media, and the tissue is sutured into the recipient vein with the nonendothelial surface directed toward the lumen.52 The study has not been repeated, but good clinical results were noted in this small series. Another attempt to use autogenous vein as a valve substitute has been reported by Plagnol and associates. In this approach, a stump of the great saphenous vein is invaginated into the femoral vein to fashion a bicuspid valve. Both experimental and clinical results have been reported,116 with 19 of 20 reconstructions being patent and competent at a mean of 10 months. One valve demonstrated reflux because of insufficient valve length at the time of reconstruction. Invagination of an adventitial surface into the venous lumen is of some concern but was not substantiated in this study.
Maleti and colleagues reported a technique for constructing a bicuspid or monocusp venous valve by dissecting the intimal-medial wall of the thickened postphlebitic vein to form the cusp or cusps. An ophthalmic knife is used to divide the vein wall into one or two sheets to fashion the valve cusps. The initial seven cases did well.117 By 2006, 18 venous valves were constructed in 16 patients with recurrent or nonhealing venous ulcers to treat chronic deep venous insufficiency secondary to the postthrombotic process.118 The patients received anticoagulation for 6 months. Early thrombosis below the valve occurred in two patients, and there was one late occlusion shortly after starting oral contraceptives. Therefore, 95% of treated segments remained primarily patent and competent, with significantly improved duplex and air plethysmographic results at a mean 22 months of follow-up. Ulcer healing occurred in 16 cases (88.9%) at a median of 12 weeks with no recurrences. There was no associated mortality. Maleti’s most recent improvement has been to place two sutures on the cusp or cusps to hold the valve in the semiopen position and thereby prevent valve collapse (Fig. 60-14) and improve neovalve competence.119 This modification was needed because follow-up (mean of 57 months) of 19 operations demonstrated valve competence in 13 of 19, or 68%. The one case added to the 2006 report included an episode of DVT, and the long-term ulcer healing rate was now 84% with two recurrences. The second group studied (modification included) consisted of 21 operations with a mean 11 months of surveillance. All valves were competent, and there was a 95% ulcer healing rate and two recurrences (9.5%). Some excellent intraoperative images and illustrations can be found in a review article by Maleti and Perrin.120 This interesting early work has been verified by at least one investigator to date.121
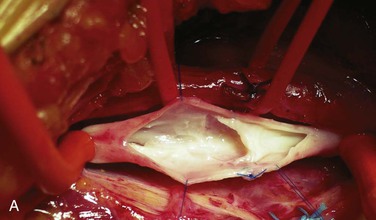
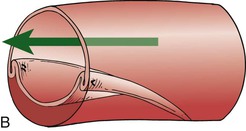
Figure 60-14 A, This intraoperative photograph shows a monocusp valve made from the inner wall of a postthrombotic vein with a fine ophthalmic knife. Two sutures (blue color) are placed near the outer edges to keep the valve from collapsing while at rest. B, Artist’s depiction of how the monocusp valve does not completely collapse against the nonluminal wall during antegrade venous flow. The arrow demonstrates the direction of normal venous blood flow toward the heart during exercise. (Courtesy Dr. Oscar Maleti.)
Selected Key References
Kistner RL. Surgical repair of a venous valve. Straub Clin Proc. 1968;24:41–43.
Those who have the courage to be the first should be recognized for the effort, and this is one of those articles.
Kistner RL, Ferris EB, Randhawa G, Kamida C. A method of performing descending venography. J Vasc Surg. 1986;4:464–468.
One of the initial articles to look critically at deep venous reflux and to quantify it on the basis of venographic imaging. It is a commonly quoted article when venous reflux and valve repair are discussed.
Lugli M, Guerzoni S, Garofalo M, Smedile G, Maleti O. Neovalve construction in deep venous incompetence. J Vasc Surg. 2009;49:156–163.
The most recent innovative approach to treatment of the postthrombotic insufficient venous system. It was selected because it is innovative and cutting edge in the care of these patients.
Masuda EM, Kistner RL. Long-term results of venous valve reconstruction: a four to twenty-one year follow-up. J Vasc Surg. 1994;19:391–403.
This group was the first to report on the repair of venous valves to prevent deep venous reflux, and this study still stands as the longest follow-up of such patients.
Raju S, Fredericks RK, Neglèn PN, Bass JD. Durability of venous valve reconstruction techniques for “primary” and postthrombotic reflux. J Vasc Surg. 1996;23:357–367.
This report compares various methods of valve repair in terms of valve competence and clinical result. It is from one of the few centers that have sufficient numbers to make such a comparison with statistical validity.
Raju S, Hardy JD. Technical options in venous valve reconstruction. Am J Surg. 1997;173:301–307.
This article provides excellent technical points on the various types of venous valve repair from a group with possibly the largest experience in the world. They have the experience to teach us all something.
Sottiurai VS. Results of deep-vein reconstruction. Vasc Surg. 1997;31:276–278.
A large experience from a surgeon who invented one approach to open valvuloplasty.
Taheri SA, Elias SM, Yacobucci GN, Heffner R, Lazar L. Indications and results of vein valve transplant. J Cardiovasc Surg. 1986;27:163–168.
A landmark article on a new approach to treatment of the postthrombotic insufficient lower leg venous system.
Tripathi R, Sieunarine K, Abbas M, Durrani N. Deep venous valve reconstruction for non-healing leg ulcers: techniques and results. Aust N Z J Surg. 2004;74:34–39.
A large study of various methods of valve repair highlighting the use of multiple valve repairs in the same axial system to decrease clinical recurrence.
The reference list can be found on the companion Expert Consult website at www.expertconsult.com.
References
1. Coon WW, et al. Venous thromboembolism and other venous disease in the Tecumseh community health study. Circulation. 1973;48:839–846.
2. Baker SR, et al. Epidemiology of chronic venous ulcers. Br J Surg. 1988;78:864–867.
3. Heit JA, et al. Trends in the incidence of venous stasis syndrome and venous ulcer: a 25-year population-based study. J Vasc Surg. 2001;33:1022–1027.
4. Nicolaides AN. Investigation of chronic venous insufficiency: a consensus statement. Circulation. 2000;102:e126–e163.
5. Mayberry JC, et al. Fifteen-year results of ambulatory compression therapy for chronic venous ulcers. Surgery. 1991;109:575–581.
6. Erickson CA, et al. Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance. J Vasc Surg. 1995;22:629–636.
7. Kalra M, et al. Surgical treatment of venous ulcers: role of subfascial endoscopic perforator vein ligation. Surg Clin North Am. 2003;83:671–705.
8. Neglen P, et al. Venous outflow obstruction: an underestimated contributor to chronic venous disease. J Vasc Surg. 2003;38:879–885.
9. Raju S, et al. The clinical impact of iliac venous stents in the management of chronic venous insufficiency. J Vasc Surg. 2002;35:8–15.
10. Plate G, et al. Physiologic and therapeutic aspects in congenital vein valve aplasia of the lower limb. Ann Surg. 1983;198:229–233.
11. Raju S, et al. Venous valve station changes in “primary” and post-thrombotic reflux: an analysis of 149 cases. Ann Vasc Surg. 2000;14:193–199.
12. Budd TW, et al. Histopathology of veins and venous valves of patients with venous insufficiency syndrome: ultrastructure. J Med. 1990;21:181–199.
13. Sandri JL, et al. Diameter-reflux relationship in perforating veins of patients with varicose veins. J Vasc Surg. 1999;30:867–875.
14. Clarke H, et al. Role of venous elasticity in the development of varicose veins. Br J Surg. 1989;76:577–580.
15. O’Donnell TF. Chronic venous insufficiency: an overview of epidemiology, classification, and anatomic considerations. Semin Vasc Surg. 1988;1:60–65.
16. Kistner RL, et al. Deep venous valve reconstruction. Cardiovasc Surg. 1995;3:129–140.
17. Danielson G, et al. Reflux from thigh to calf, the major pathology in chronic venous ulcer disease: surgery indicated in the majority of patients. Vasc Endovasc Surg. 2004;38:209–219.
18. Masuda EM, et al. Long-term results of venous valve reconstruction: a four to twenty-one year follow-up. J Vasc Surg. 1994;19:391–403.
19. Killewich LA, et al. Spontaneous lysis of deep venous thrombi: rate and outcome. J Vasc Surg. 1989;9:89–97.
20. Masuda EM, et al. The natural history of calf vein thrombosis: lysis of thrombi and development of reflux. J Vasc Surg. 1998;28:67–73.
21. McLafferty RB, et al. Late clinical and hemodynamic sequelae of isolated calf vein thrombosis. J Vasc Surg. 1998;27:50–56.
22. Eriksson I, et al. Influence of the profunda femoris vein on venous hemodynamics of the limb: experience from thirty-one deep vein valve reconstructions. J Vasc Surg. 1986;4:390–395.
23. Queral LA, et al. Surgical correction of chronic deep venous insufficiency by valvular transposition. Surgery. 1980;87:688–695.
24. Raju S, et al. Axial transformation of the profunda femoris vein. J Vasc Surg. 1998;27:651–659.
25. O’Donnell TF, et al. Clinical, hemodynamic, and anatomic follow-up of direct venous reconstruction. Arch Surg. 1987;122:474–482.
26. Bry JD, et al. The clinical and hemodynamic results after axillary-to-popliteal vein valve transplantation. J Vasc Surg. 1995;21:110–119.
27. Raju S, et al. Durability of venous valve reconstruction techniques for “primary” and post-thrombotic reflux. J Vasc Surg. 1996;23:357–367.
28. Raju S. Multiple-valve reconstruction for venous insufficiency: indications, optimal technique, and results. Veith FJ. Current critical problems in vascular surgery. ed 4. Quality Medical Publishing: St. Louis; 1992:122–125.
29. Nicolaides AN (chair) and the Executive Committee of the Ad Hoc Committee, American Venous Forum. Classification and grading of chronic venous disease in the lower limbs: a consensus statement. [6th annual meeting, February 22–25, 1994, Maui, Hawaii] Gloviczki P, Yao JST. Handbook of venous disorders. Chapman & Hall: London, England; 2001:653–656.
30. Vasquez MA, et al. Revision of the venous clinical severity score: venous outcomes consensus statement: Special communication of the American Venous Forum Ad Hoc Outcomes Working Group. J Vasc Surg. 2010;52:1387–1396.
31. Rutherford RB, et al. Outcome assessment in chronic venous disease. Gloviczki P. Handbook of venous disorders: guidelines of the American Venous Forum. ed 3. Hodder Arnold: London; 2009:684–693.
32. Labropoulos N, et al. Definition of venous reflux in lower-extremity veins. J Vasc Surg. 2003;38:793–798.
33. Gloviczki P, et al. The care of patients with varicose veins and associated chronic venous diseases; clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011;53:2S–48S.
34. Raju S. New approaches to the diagnosis and treatment of venous obstruction. J Vasc Surg. 1986;4:42–54.
35. Nicolaides AN, et al. The relation of venous ulceration with ambulatory venous pressure measurements. J Vasc Surg. 1993;17:414–419.
36. Neglen P, et al. Proximal lower extremity chronic venous outflow obstruction: recognition and treatment. Semin Vasc Surg. 2002;15:57–64.
37. Kistner RL, et al. A method of performing descending venography. J Vasc Surg. 1986;4:464–468.
38. Cheatle TR, et al. Venous valve repair: early results in fifty-two cases. J Vasc Surg. 1994;19:404–413.
39. Kistner RL, et al. Surgery in acute and chronic venous disease. Surgery. 1979;85:31–43.
40. Wang S, et al. Effect of external valvuloplasty of the deep vein in the treatment of chronic venous insufficiency of the lower extremity. J Vasc Surg. 2006;44:1296–1300.
41. Us M, et al. The use of external banding increases the durability of transcommissural external deep venous valve repair. Eur J Vasc Endovasc Surg. 2007;33:494–501.
42. Meissner MH, et al. Secondary chronic venous disorders. J Vasc Surg. 2007;46:68S–83S.
43. Camilli S, et al. External banding valvuloplasty of the superficial femoral vein in the treatment of primary deep valvular incompetence. Int Angiol. 1994;13:218–222.
44. Raju S, et al. Transcommissural valvuloplasty: technique and results. J Vasc Surg. 2000;32:969–976.
45. Tripathi R, et al. Deep venous valve reconstruction for non-healing leg ulcers: techniques and results. Aust N Z J Surg. 2004;74:34–39.
46. Rosales A, et al. External venous valve plasty (EVVP) in patients with primary chronic venous insufficiency (PCVI). Eur J Endovasc Surg. 2006;32:570–576.
47. Valentine RJ, et al. Vessels of the leg. Valentine RJ, Wind GG. Anatomic exposures in vascular surgery. ed 2. Lippincott Williams & Wilkins: Philadelphia; 2003:467–522.
48. Sun J, et al. Anatomic and histologic studies on the valves of the venous system in lower extremities. Vasc Surg. 1990;24:85–90.
49. Powell T, et al. The valves of the external iliac, femoral, and upper third of the popliteal veins. Surg Gynecol Obstet. 1951;92:453–455.
50. Basmajian JV. The distribution of valves in the femoral, external iliac, and common iliac veins and their relationship to varicose veins. Surg Gynecol Obstet. 1952;95:537–542.
51. Lane JL, et al. Intermediate to long-term results of repairing incompetent multiple deep venous valves using external valvular stenting. Aust N Z J Surg. 2003;73:267–274.
52. Raju S, et al. Technical options in venous valve reconstruction. Am J Surg. 1997;173:301–307.
54. Kistner RL. Surgical repair of a venous valve. Straub Clin Proc. 1968;24:41–43.
55. Raju S. Venous insufficiency of the lower limb and stasis ulceration: changing concepts and management. Ann Surg. 1983;197:688–697.
56. Sottiurai VS. Technique in direct venous valvuloplasty. J Vasc Surg. 1988;8:646–648.
57. Tripathi R, et al. Trapdoor internal valvuloplasty: a new technique for primary deep vein valvular incompetence. Eur J Vasc Endovasc Surg. 2001;22:86–89.
58. Raju S, et al. Valve reconstruction procedures for nonobstructive venous insufficiency: rationale, techniques, and results in 107 procedures with two- to eight-year follow-up. J Vasc Surg. 1988;7:301–310.
59. Kistner RL. Surgical technique of external venous valve repair. Straub Found Proc. 1990;55:15–16.
60. Nishibe T, et al. Intermediate-term results of angioscopy-assisted anterior valve sinus plication for primary deep venous insufficiency. J Cardiovasc Surg (Torino). 2007;48:21–25.
61. Gloviczki P, et al. Femoral vein valve repair under direct vision without venotomy: a modified technique with use of angioscopy. J Vasc Surg. 1991;14:645–648.
62. Belcaro G, et al. External femoral vein valvuloplasty with limited anterior plication (LAP): a 10-year randomized, follow-up study. Angiology. 1999;50:531–536.
63. Makhatilov G, et al. Endoscopically directed external support of femoral vein valves. J Vasc Surg. 2009;49:676–680.
64. Jamieson WG, et al. Clinical results of deep venous valvular repair for chronic venous insufficiency. Can J Surg. 1997;40:294–299.
65. Welch H, et al. Femoral vein valvuloplasty: intraoperative angioscopic evaluation and hemodynamic improvement. J Vasc Surg. 1992;16:694–700.
66. Taheri SA, et al. Vein valve transplant. Surgery. 1982;91:28–33.
67. Raju S, et al. Axillary vein transfer in trabeculated post-thrombotic veins. J Vasc Surg. 1999;29:1050–1064.
68. Sottiurai VS. Supravalvular incision for valve repair in primary valvular insufficiency. Bergan JJ, Kistner RL. Atlas of venous surgery. WB Saunders: Philadelphia; 1992:137–138.
69. Cardon JM, et al. Use of ipsilateral greater saphenous vein as a valved transplant in management of post-thrombotic deep venous insufficiency: long-term results. Ann Vasc Surg. 1999;13:284–289.
70. Perrin M. Reconstructive surgery for deep venous reflux: a report on 144 cases. Cardiovasc Surg. 2000;8:246–255.
71. Poller L, et al. Fixed minidose warfarin: a new approach to prophylaxis against venous thrombosis after major surgery. Br Med J (Clin Res Ed). 1987;295:1309–1312.
72. Perrin M, et al. Results of valvuloplasty in patients presenting with deep venous insufficiency and recurring ulceration. Ann Vasc Surg. 1999;13:524–532.
73. Kistner RL. Surgical repair of the incompetent femoral vein valve. Arch Surg. 1975;110:1336–1342.
74. Ferris EB, et al. Femoral vein reconstruction in the management of chronic venous insufficiency: a 14-year experience. Arch Surg. 1982;117:1571–1579.
75. Lurie F, et al. Results of deep-vein reconstruction. Vasc Surg. 1997;31:275–276.
76. Perrin MR. Results of deep-vein reconstruction. Vasc Surg. 1997;31:273–275.
77. Guarnera G, et al. External banding of the superficial femoral vein in the treatment of recurrent varicose veins. Int Angiol. 1998;17:268–271.
78. Makhatilov G, et al. Endoscopically directed external support of femoral vein valves. J Vasc Surg. 2009;49:676–680.
79. Taheri SA, et al. Vein valve transplant. Surgery. 1982;91:28–33.
80. Taheri SA, et al. Indications and results of vein valve transplant. J Cardiovasc Surg. 1986;27:163–168.
81. Nash T. Long-term results of vein valve transplants placed in the popliteal vein for intractable post-phlebitic venous ulcers and pre-ulcer skin changes. J Cardiovasc Surg. 1988;29:712–716.
82. Rai DB, et al. Chronic venous insufficiency disease: its etiology: a new technique for vein valve transplantation. Int Surg. 1991;76:174–178.
83. Sottiurai VS. Results of deep-vein reconstruction. Vasc Surg. 1997;31:276–278.
84. Eklof BG, et al. Venous bypass and valve reconstruction: long-term efficacy. Vasc Med. 1998;3:157–164.
85. Johnson ND, et al. Late objective assessment of venous valve surgery. Arch Surg. 1981;116:1461–1466.
86. Dalsing MC, et al. An early experience with endovascular venous valve transplantation. J Vasc Surg. 1996;24:903–905.
87. Ofenloch JC, et al. Endoscopic venous valve transplantation with a valve-stent device. Ann Vasc Surg. 1997;11:62–67.
88. Boudjemline Y, et al. Is percutaneous implantation of a bovine venous valve in the inferior vena cava a reliable technique to treat chronic venous insufficiency syndrome? Med Sci Monit. 2004;10:61–66.
89. Kaya M, et al. Glutaraldehyde-preserved venous valve transplantation in the dog. J Surg Res. 1988;45:294–297.
90. Gomez-Jorge J, et al. Percutaneous deployment of a valved bovine jugular vein in the swine venous system: a potential treatment for venous insufficiency. J Vasc Interv Radiol. 2000;11:931–936.
91. Gale SS, et al. Percutaneous venous valve bioprosthesis: initial observations. Vasc Endovasc Surg. 2004;38:221–224.
92. Pavcnik D, et al. Percutaneous bioprosthetic venous valve: a long-term study in sheep. J Vasc Surg. 2002;35:598–602.
93. Brountzos E, et al. Remodeling of suspended small intestinal submucosa venous valve: an experimental study in sheep to assess the host cells’ origin. J Vasc Interv Radiol. 2003;14:349–356.
94. Pavcnik D, et al. Second-generation percutaneous bioprosthetic valve: a short-term study in sheep. J Vasc Surg. 2004;40:1223–1227.
95. Pavcnik D. Update on venous valve replacement: long-term clinical results. Vascular. 2006;14(Suppl 1):S106.
96. Pavcnik D, et al. Percutaneous management of chronic deep venous reflux: review of experimental work and early clinical experience with bioprosthetic valve. Vasc Med. 2008;13:75–84.
97. Pavcnik D, et al. Percutaneous autologous venous valve transplantation: short-term feasibility study in an ovine model. J Vasc Surg. 2007;46:338–345.
98. Jones CM, et al. Retention of an autologous endothelial layer on a bioprosthetic valve for the treatment of chronic deep venous insufficiency. J Vasc Interv Radiol. 2012;23:697–703.
99. de Borst GJ, et al. Percutaneous venous valve designs for treatment of deep venous insufficiency. J Endovasc Ther. 2012;19:291–302.
100. Moriyama M, et al. Evaluation of prosthetic venous valve, fabricated by electrospinning, for percutaneous treatment of chronic venous insufficiency. J Artif Organs. 2011;14:294–300.
101. Ku DN, et al: Design of a vein valve replacement. Presented at the 24th annual meeting of the American Venous Forum, Orlando, Florida, February 8–11, 2012.
102. Calhoun AD, et al. Fresh and cryopreserved venous allografts in genetically characterized dogs. J Surg Res. 1977;22:687–696.
103. Hill R, et al. Development of a prosthetic venous valve. J Biomed Mater Res. 1985;19:827–832.
104. Taheri SA, et al. Experimental prosthetic vein valve. Am J Surg. 1988;156:111–114.
105. Taheri SA, et al. Experimental prosthetic vein valve: long-term results. Angiology. 1995;46:299–303.
106. Reeves TR, et al. Mechanical characteristics of lyophilized human saphenous vein valves. J Vasc Surg. 1997;26:823–828.
107. Burkhart HM, et al. Experimental repair of venous valvular insufficiency using a cryopreserved venous valve allograft aided by a distal arteriovenous fistula. J Vasc Surg. 1997;26:817–822.
108. Dalsing MC, et al. A multicenter, phase I evaluation of cryopreserved venous valve allografts for the treatment of chronic deep venous insufficiency. J Vasc Surg. 1999;30:854–866.
110. Garcia-Rinaldi R, et al. Implantation of cryopreserved allograft pulmonary monocusp patch to treat nonthrombotic femoral vein incompetence. Tex Heart Inst J. 2002;29:92–99.
111. Garcia-Rinaldi R. Regarding “Venous reflux repair with cryopreserved vein valves.”. J Vasc Surg. 2003;38:1139–1140.
112. Opie JC, et al. Monocusp—novel common femoral vein monocusp surgery uncorrectable chronic venous insufficiency with aplastic/dysplastic valves. Phlebology. 2008;23:158–171.
113. Ignat’ev IM, et al. First experience in forming a multi-flap valve of the common femoral vein in avalvulation of the deep veins of lower extremities. Angiol Sosud Khir. 2010;16:77–79.
114. Dalsing MC, et al. Venous valvular insufficiency: influence of a single venous valve (native and experimental). J Vasc Surg. 1991;14:576–587.
115. Rosenbloom MS, et al. Early experimental experience with a surgically created, totally autogenous venous valve: a preliminary report. J Vasc Surg. 1988;7:642–646.
116. Plagnol P, et al. Autogenous valve reconstruction technique for post-thrombotic reflux. Ann Vasc Surg. 1999;13:339–342.
117. Maleti O. Venous valvular reconstruction in post-thrombotic syndrome. A new technique. J Mal Vasc. 2002;27:218–221.
118. Maleti O, et al. Neovalve construction in postthrombotic syndrome. J Vasc Surg. 2006;43:794–799.
119. Lugli M, et al. Neovalve construction in deep venous incompetence. J Vasc Surg. 2009;49:156–163.
120. Maleti O, et al. Reconstructive surgery for deep vein reflux in the lower limbs: techniques, results and indications. Eur J Vasc Surg. 2011;41:837–848.
121. Corcos L, et al. A new autologous venous valve by intimal flap. One case report. Minerva Cardioangiol. 2003;51:395–404.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]Chapter 60
Chronic Venous Insufficiency
Deep Vein Valve Reconstruction
Michael C. Dalsing
Chronic venous insufficiency (CVI) can be asymptomatic or advance to a state of chronic, unrelenting venous ulceration. Skin changes such as hyperpigmentation consistent with CVI of the lower extremity have been reported in 6 to 7 million U.S. citizens, with progression to venous ulceration occurring in up to 2%.1–3 It is estimated that the cost of venous ulcer care alone is more than $1 billion annually.4 The excellent early success of ulcer healing with compression is marred by the risk of recurrence in up to 40% of compliant patients but approaching 100% in noncompliant patients.5,6 Treating all superficial and perforator vein insufficiency can reduce the recurrence risk, but it still is noted in up to 33% of patients with primary deep CVI and 70% of those with the postthrombotic syndrome. These facts demonstrate the importance of deep venous disease in the pathophysiologic process of CVI.7 Deep venous obstructive disease in combination with venous insufficiency has been noted in up to 55% of patients with CVI, especially in those with the most severe symptoms.8 Correcting iliac obstruction while ignoring the deep venous insufficiency can result in a long-term ulcer-free rate of nearly 60%.9 What patients remain are a select but finite cohort with chronic deep venous insufficiency who will benefit from valve reconstruction.
Pathogenesis
Etiology
Rarely patients are observed with congenital absence of lower extremity venous valves, venous aplasia or dysplasia.10 More commonly patients with primary venous insufficiency have either floppy, redundant, elongated valve cusps or an enlarged venous diameter, both of which prevent normal valve cusp apposition.11–14 In these cases, there is no apparent inciting event that caused the anatomic changes observed. As a consequence of these pathologic changes, spontaneously with standing or with additional stresses, reflux occurs in the affected valves. Except in the case of aplasia or dysplasia, in-situ tightening (repair) of the structurally intact valve can render it competent and functional.
Secondary venous insufficiency is often the result of acute deep venous thrombosis (DVT) and in 40% to 70% of all affected patients may be the cause of chronic deep venous valvular incompetence.11,15–17 The resulting inflammation and scarring with or without recanalization can cause foreshortening and fibrosis of the valve leaflets, small perforations, or valve adhesion and luminal narrowing.11 The valves are generally so damaged that in-situ repair is not feasible. The options remaining to prevent complete system reflux are transplantation of a competent valve from a distant location, transposition of the incompetent venous system to a position distal to a local competent valve, or the use of less traditional valve substitutes.
This standard differentiation between “primary” and “secondary” (postthrombotic) venous disease has been challenged by clinical imaging studies and by direct observation of the veins and valves at surgery. The simultaneous occurrence of both pathologic processes within the same patient is a clinical observation made decades ago.18 During attempted surgical repair of venous valve reflux, 6 of 11 excised veins demonstrated typical postthrombotic pathologic changes, but nonthrombotic phlebosclerosis was noted in the remaining 5.11 Phlebosclerosis was defined as vein wall thickening or fibrosis at the valve station or thickening of the valve cusps or intima (or both). One theory suggested to explain the thickened yet preserved normal valve architecture is that primary reflux with the associated sustained high venous wall pressure might cause the pathologic picture. DVT could also be the cause with rapid resolution of venous thrombi, an event documented by investigators studying acute DVT,19 allowing the involved valves to escape the severe damage usually associated with thrombosis. Alternatively, the valve itself may not be directly involved in the thrombotic process. Venous reflux has been documented proximal to an isolated distal thrombosis.19–21 In this case, the fibrotic process in the vein wall may involve the valve station only during thrombus resolution; the resultant thickened, noncompliant vein wall could cause the cusps to become floppy by virtue of a decrease in wall diameter.11 The valve remains architecturally intact, thin, and compliant and can be made competent by standard reefing of the cusps.
Hemodynamics
To realize the goal of controlling lower limb venous hypertension, correction of deep axial reflux proximal to the calf and ankle area is required (see Chapters 11 and 12). If one disregards this axiom, most commonly by ignoring profunda femoris vein reflux, isolated femoral vein valve reconstruction will be clinically unsuccessful because the offending hemodynamic effects will not be altered.22 Alternatively, when the profunda system is competent, repair of femoral vein incompetence does improve lower limb venous hemodynamics by preventing total axial reflux.22,23 In some cases of femoral vein thrombosis with occlusion, there is tremendous dilatation of the profunda femoris vein such that repair of valvular reflux in this vein will adequately reverse overall pathologic venous hemodynamics (Fig. 60-1).24 An alternative method of correcting significant axial reflux when both femoral systems are incompetent is to position a competent valve in the popliteal vein.25–27 At least one investigator has performed multiple tibial vein valve repairs to accomplish the same goal.28
Diagnostic Evaluation
History and Physical Examination
Patients with CVI may present initially with dependent edema, leg fatigue, itching, telangiectases, a feeling of overall fullness, or any combination thereof. Progression in severity may be noted by the presence of varicose veins, increasing pain, intractable edema, and skin changes (such as eczema, cellulitis, hyperpigmentation, lipodermatosclerosis, and stasis ulcers). A careful history should take note of previous episodes of DVT, known hypercoagulable conditions, and any limitations in physical and occupational activity resulting from venous insufficiency. In addition, the physical examination can eliminate other causes of the presenting signs and symptoms, such as ischemic ulcers, diabetic ulcers, dermatologic disorders, and even skin or soft tissue cancer. Each patient should ultimately be stratified according to the CEAP system to clearly define the venous disease present, which will allow the formation of a focused and appropriate management strategy.29 Candidates for deep venous valvular reconstruction typically have class 5/6 disease or disabling symptoms, such as severe edema (C4). An in-depth extension of the clinical classification (Venous Clinical Severity Score) provides a quantification of disease severity and is a useful evaluation tool to determine a patient’s response to treatment.30 Quality of life surveys provide an estimation of the impact of venous disease on the patient’s life and the effect that therapy has on the patient’s overall well-being.31 Application of these surveys before and after surgery will demonstrate those patients most improved by the intervention.
Noninvasive Evaluation
The noninvasive evaluation of patients with chronic deep venous insufficiency begins with a complete venous duplex study (see Chapter 18). It is essential to clarify the extent and anatomic location of all venous disease (specific veins can be imaged to determine the precise location of reflux), and it will provide some indication of the etiology (congenital, primary, or secondary) and aid in determining the pathophysiologic mechanism (reflux, obstruction, or both) of the disease present. The imaging is often so clear that venous valve cusps can be seen moving in the venous stream (Fig. 60-2). Insufficiency within any segment of the deep venous system is defined as a prolonged reflux time through the valve after a provocative test. A reflux time of longer than 0.5 second is considered abnormal in the tibial and deep femoral veins but is somewhat longer, more than 1 second, for the femoral and popliteal veins.32 Venous obstruction is seen as thickened, scarred, and constricted veins or valves with poor flow and diminished augmentation after distal or proximal compression. Respiratory variation can be lost as a consequence of local disease or proximal obstruction or stenosis. Similar imaging and spectral analysis will determine obstruction or, more commonly, insufficiency of the superficial and perforator veins. This is all the diagnostic evaluation needed if only the superficial and perforator veins are found to be pathologic.
I use air plethysmography (see Chapter 17) to provide an overall quantification of the impact of deep venous insufficiency before deep venous valvular reconstruction and to provide some insight into the effectiveness of treatment. Currently, this diagnostic modality is used for specific indications or as a research tool only.33
Invasive Evaluation
For patients being considered for deep venous valvular repair, venography is required for precise operative planning. Ascending venography (see Chapter 20) defines deep venous system anatomy, helps eliminate obvious obstruction as an etiologic factor, and provides a means of selecting the most disease-free portion of the incompetent and postthrombotic venous system when valve transplantation is an option.11,34 Ambulatory venous pressure has been shown to correlate with the presence of venous ulceration and is one method available to estimate the degree of venous hypertension.35 A venous reflux time of less than 20 seconds confirms that valvular reflux is present in the limb being evaluated. Intravenous hemodynamic study, although useful, can be provided by less invasive means, so it is not always a component of an ascending venographic evaluation. Similarly, the practice of directly measuring lower limb intravenous pressure before and after thigh cuff occlusion has not proved to be a reliable determinant of significant proximal venous occlusion.11,34,36 The importance of significant iliac vein occlusive disease is determined best by the use of intravenous ultrasonography.36 Descending venography (see Chapter 20) is used to determine valve leaflet integrity, anatomic location, and extent or degree of reflux (Fig. 60-3).37 Assessment of the competence of the profunda femoris venous system in addition to the femoral system is imperative because it will affect the choice and location of venous valve repair and the potential for valve transposition.27,38,39 Descending venography does not have absolute accuracy in determining the presence or absence of a normal valve.11 Raju and colleagues reported that descending venography had a false-positive rate of 11% (a valve considered present was absent at surgery) and false-negative rate of 25% (a valve thought absent was present on direct inspection) when direct inspection at operation was the “gold standard.”11 However, when it is combined with a well-performed venous duplex examination, it is the best method available to determine preoperatively whether in-situ reconstruction will be possible.
Treatment Selection
Natural History and Patient Risk Assessment
The natural history of patients being considered for deep venous valvular repair has generally been extensive because all less invasive interventions to solve the patient’s problems have been attempted and have failed. With the traditional approach of treating all superficial and perforator disease first regardless of the status of the deep system, about 33% of patients with primary deep venous incompetence and 70% of those with postthrombotic syndrome will experience ulcer recurrence, thus emphasizing that deep venous disease must eventually be treated in select patients.7 Separate investigators have added external valvuloplasty of the femoral vein to high ligation and saphenous vein stripping to improve the clinical durability in advanced disease, with gratifying results.40,41 Iliac vein occlusive disease has been treated with the knowledge that symptoms may resolve in about 60% of patients.9 For the remaining 40%, deep venous reflux will require intervention to alleviate symptoms.
Patient risk assessment must follow the tenets of any open operative intervention (see Chapter 31). Hemodynamic instability from the operation is minimal, but because the operative intervention is time-consuming and technically challenging, general anesthesia is typically required. An acceptable cardiac and pulmonary status is required. Systemic infection should be treated before intervention. Systemic disease that might have an impact on healing, such as collagen vascular disease, diabetes, chronic renal insufficiency, or lower extremity arterial occlusive disease, will influence the surgeon’s decision to perform a venous intervention.42 These conditions are relative contraindications to aggressive venous intervention unless they are corrected or medically optimized before venous valve repair.
Treatment Options
The treatment options available to correct deep venous valvular reflux are determined by the availability of complete and structurally intact venous valves. Selection of the operative technique when the valve cusps are architecturally preserved is somewhat determined by the degree of cusp prolapse, the surgeon’s preference, and the reported long-term success. In the case of valve prolapse secondary to vein wall dilatation only, vasospasm alone may reestablish a competent valve, and in such cases simple external banding of the vein will provide a workable solution to prevent reflux.43 When wall dilatation with more pronounced cusp prolapse is present, external valvuloplasty will provide a way to decrease wall diameter, and the use of certain techniques will also enable reefing of the valve cusps into a functional position. With pronounced valve leaflet prolapse, internal valvuloplasty allows direct and extensive cusp shortening and reduction of wall diameter. When there is no identifiable valve structure within an incompetent system, two potential options are available. If a parallel axial system has a competent valve or one that can be made so, a transposition procedure is an option. When this is not feasible, valve transplantation of a competent valve from a distant location remains an option. Valve substitutes are being investigated, with some autogenous options showing promise. The quest for a percutaneous option has provided few answers to date. In some instances, intervention in two or more separate axial venous systems (e.g., the femoral and profunda femoris veins) or into the popliteal location will be required to prevent axial reflux into the calf and ankle soft tissues. Multiple valve repairs in the same incompetent axial system (e.g., two or more in the femoral vein) are being investigated in the hope of decreasing recurrent reflux and thus symptoms28,44–46; however, many surgeons have reported success when only one valve per incompetent system is repaired.
Surgical Treatment
Relevant Anatomy
The common femoral, profunda femoris, and femoral veins are covered by skin, soft tissue, and fascia in the groin and by the sartorius muscle more distally. More caudally, the femoral vein occupies the adductor [Hunter’s] canal, which places it deep to the sartorius and flanked by the vastus medialis and adductor longus fascia muscles. As the femoral vein exits the adductor canal, it is called the popliteal vein and lies between the heads of the gastrocnemius muscle distally but is covered only by skin, soft tissue, and fascia directly behind the knee. The anterior tibial veins lie in the anterior calf compartment deep to the anterior tibialis muscle. The posterior tibial and peroneal veins lie in the deep posterior compartment and are covered by the soleus and gastrocnemius muscles, which form the superficial posterior compartment.47
Valves are universally present in the paired tibial and peroneal veins, with 3 to 12 valves rather evenly distributed in each vein.48 The majority of popliteal veins (>90%) have one to three valves with a slight trend to be located more caudal in the leg.48 The femoral veins have one to five valves.48,49 The most constant valve occurring in about 90% of patients is found in the femoral vein 1 to 2 cm distal to joining the profunda femoris vein.48–50 In 88% of patients, the profunda femoris vein has one to four valves.48 The common femoral vein may (30%-50% of patients) have one or two valves within a few centimeters of the inguinal ligament.48–50
Operative Planning
In the event that an intact valve has been confirmed by preoperative duplex and venographic studies, most experienced surgeons choose the proximal femoral vein for valvuloplasty or to repair both the femoral and profunda femoris valves if both systems are incompetent. This decision is based on the ease of exposure, familiarity with the approach, and size of the veins available for repair. When both proximal femoral axial systems are incompetent, some have chosen repair of the popliteal vein valve, which is considered the “gateway” to the lower leg venous system. However, mid or distal femoral vein valves can be repaired if they are surgically accessible and amenable to valvuloplasty by virtue of retained architecture. As one proceeds down the venous system, vein diameters and valve leaflets become smaller and therefore more difficult to repair. Nevertheless, even tibial vein valves have been successfully repaired. If a transposition operation is planned, duplex ultrasound and descending venography must have identified the presence of a competent valve. Valve transplantation requires having identified a valve in the axillary or brachial vein by duplex ultrasonography or venography. Ligation of upper extremity veins is well tolerated. The optimal place for implantation into the lower extremity is into the least damaged vein segment available, which will prevent axial reflux into the calf area.
Prophylactic antibiotics are given during the procedure (e.g., first-generation cephalosporin) but are continued postoperatively for 2 or 3 days by most surgeons.41,44,51 Intraoperative heparin is commonly given when venous occlusion is required during valve repair; a typical dose is 2000 to 10,000 units, which is not generally reversed.38,41,44,51–53
Techniques
Overall Exposure
If reconstruction of the proximal femoral veins (femoral or profunda femoris) is the goal, a groin incision is made in the direction of the vessels to expose the first and second femoral valves.48 Further dissection through the fascia that lies beneath the sartorius muscle will expose the profunda femoris vein if necessary. After exposure of the valve targeted for repair and the adjoining segment of vein, the strip test should be performed to evaluate the competence of the valve This test entails milking blood antegrade past the valve while inflow is occluded, with subsequent application of retrograde pressure against the valve. Reflux is demonstrated by refilling of the vein distally. This incision may also provide exposure for valve transposition or transplantation, if it is required.
After identification of the valve station to be repaired, careful adventitial dissection to identify the valve attachment lines is useful.52 This dissection facilitates proper placement of the venotomy so as not to damage the valve leaflets, when required, and verifies that valve repair is feasible. A lack of valve attachment lines can signify destruction of the valve and suggests the need to consider techniques other than in-situ repair.52
In other situations, a more distal femoral, popliteal, or even tibial vein may be the desired location for valve repair or transplantation. In these situations, the medial exposure is much like that used for exposure of the like-named artery.47 The popliteal vein can be exposed through a posterior S-shaped incision, with the transverse incision made in the posterior knee crease to decrease the chance of scar contraction.47
Internal Valvuloplasty
For decades, the open method of direct valve cusp tightening (reefing) has been the mainstay for correction of primary deep venous valvular reflux. This technique involves venotomy and suturing of the elongated valve leaflets under direct visualization. The redundant valve cusps are plicated to the vein wall with interrupted 6 or 7-0 polypropylene suture to allow proper alignment and later coaptation of the cusps. Kistner in 1968 was the first to report success using a longitudinal venotomy extending through the valve commissure (Fig. 60-4A).54 Raju later described a supracommissural approach in which a transverse venotomy was performed at least 2.5 cm above the valve (Fig. 60-4B).55 Sottiurai described a combination approach in 1988 in which a supravalvular transverse venotomy with distal extension into the valve sinus (a T-shaped venotomy) was used (Fig. 60-4C).56 The “trap door” approach of Tripathi and Ktenidis (2001) involved two transverse incisions on the vein connected by a single vertical incision (Fig. 60-4D).57 Regardless of the approach, suturing of the valve leaflets remains essentially the same (Fig. 60-5). It is estimated that plication of approximately 20% of the length of the valve leaflet can generally restore competency to the valve in the majority of cases.58
Figure 60-4 Internal valvuloplasty can be accomplished by a variety of techniques used to visualize the incompetent valve leaflets. A, Artist’s representation of the method first proposed by Kistner, in which he opens the vein through the anterior commissure. B, Representation of the method of Raju, who uses a supravalvular transverse venotomy to view the valve from above without incising through the valve commissural angle. C, Representation of the method of Sottiurai, who performs a supracommissural incision with extension toward a cusp sinus to improve visualization. D, Representation of the technique used by Tripathi, who uses a “trap door” incision to provide optimal visualization of the valve cusps for repair. The method of reefing the valve to reestablish a competent valve is essentially the same in each instance.
Figure 60-5 The method of Kistner is shown in these operative pictures before valvuloplasty (A) and after valvuloplasty (B). Note the laxity of the incompetent valve before intervention, whereas after reefing of the valve cusps, the normal architecture and tension are reestablished. (Courtesy Dr. Robert Kistner.)
External Valvuloplasty
The technique of external valvuloplasty was pioneered by Kistner and reported in 1990 (Fig. 60-6).59 This approach offers the advantage of valve repair without a venotomy. It is performed by placing interrupted sutures transmurally through the valve attachment lines, which on tying leaves a decreased commissural angle and a competent valve. Others have used a running suture to accomplish a similar effect.52 Both anterior repair and posterior repair can be performed. Another group of investigators combined angioscopy with limited anterior valve sinus plication by interrupted transmural sutures in 15 limbs and achieved improvement in clinical symptoms, hemodynamics, and competence as determined by descending venography.53,60
Figure 60-6 Artist’s rendition of the method of external valvuloplasty. The enlarged venous diameter results in valve incompetence. Note how the placement of sutures decreases the diameter of the venous wall but keeps the valve cusps from harm’s way. The sutures lie outside the vein lumen in this approach.
A modification of external valvuloplasty involves the transluminal placement of sutures to reef the valve leaflets and to narrow the vein wall, much like internal valvuloplasty but without opening the vein. Gloviczki and colleagues in 1991 reported using an angioscope to directly view the valve cusps during repair (Fig. 60-7).61 A side branch of the great saphenous vein allows introduction of the angioscope, which is then advanced above the appropriate femoral vein valve for optimal visualization. Interrupted external sutures are seen entering the venous lumen and can be precisely placed to sync up the cusps at the point of attachment on the vein wall. Closure of the valve attachment angle and simultaneous tightening of the valve cusps are realized. Raju contends that use of the angioscope is not necessary after a learning curve but concedes that excellent visualization of the valve is achieved when it is used.52 He believes that identifying the valve cusp externally with the use of adventitial dissection is critical to a technically successful repair and places his sutures as demonstrated in Figure 60-8 (transcommissural valvuloplasty).44 A continuous suture can also be used to accomplish this repair.41 Limited anterior plication, a modification of this method, involves anterior vein dissection and placement of a running mattress suture at the anterior commissure, which runs from a point 3 to 4 mm proximal to the angle of the valve cusp insertion lines up to the angle of the valve cusp insertion.62 About 3 mm of the vein wall is incorporated into the stitch to adequately approximate the cusps.62 Limited anterior plication was developed with the aim of decreasing vein dissection and potentially reducing the progressive dilatation of the postrepair vein that occurs after some cases of valvuloplasty.62 It has been used most commonly in conjunction with saphenous vein stripping and limited to the femoral vein valve station.
Figure 60-7 As an improvement to “blind” placement of sutures in the method of external valvuloplasty, the use of an angioscope as suggested by Gloviczki and coworkers allows precise suture placement within the vein lumen for actual tightening (reefing) of the valve cusps.
Figure 60-8 The initial through-and-through oblique transluminal suture placed at the commissural apex catches sagging leaflets and resuspends them. A to D, Transluminal sutures, with each successive suture biting deeper and less oblique than the suture above to pull up the valve, tighten the cusp edges, deepen the sinus, and appose the valve attachment lines. Each suture is tied before the next is placed. One or two of the most caudally placed sutures may actually pass through the body of the leaflet rather than through the edge, with no subsequent ill effects. (Redrawn from Raju S, et al: Transcommissural valvuloplasty: technique and results. J Vasc Surg 32:969-976, 2000.)
External Banding
[/not-level-membership-for-surgery-category]
