[level-membership-for-anesthesiology-category]
25 Cervical Plexus Block
Placement
Anatomy
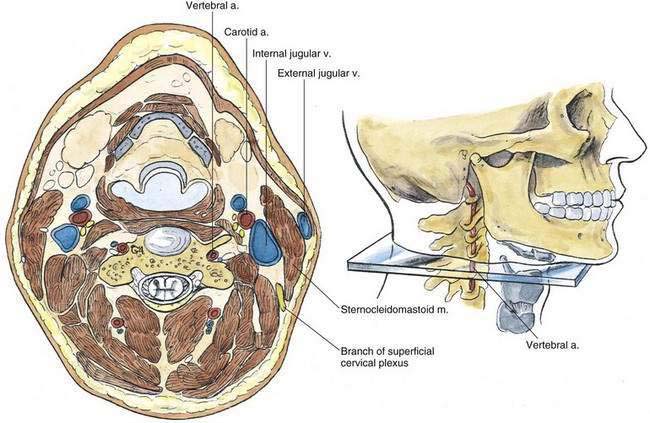
Cervical plexus block can be divided into superficial and deep techniques. The cutaneous innervation of the cervical nerves is schematically illustrated in Figure 25-1. The cervical nerves have both dorsal and ventral rami, and those illustrated in Figure 25-2 represent the ventral rami of C1-C4. In addition, there are both sensory and motor branches from the dorsal rami of C1-C4 that are not shown. Before regrouping to form the cervical plexus, the cervical nerves exit from the cervical vertebrae through a gutter in the transverse process in an anterocaudolateral direction, immediately posterior to the vertebral artery.
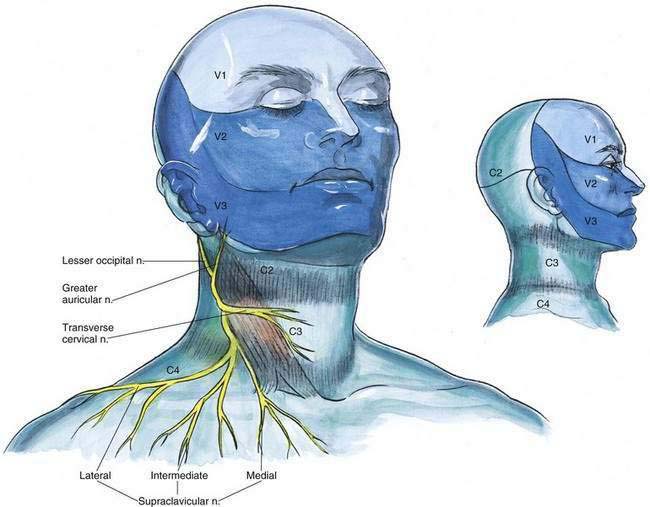
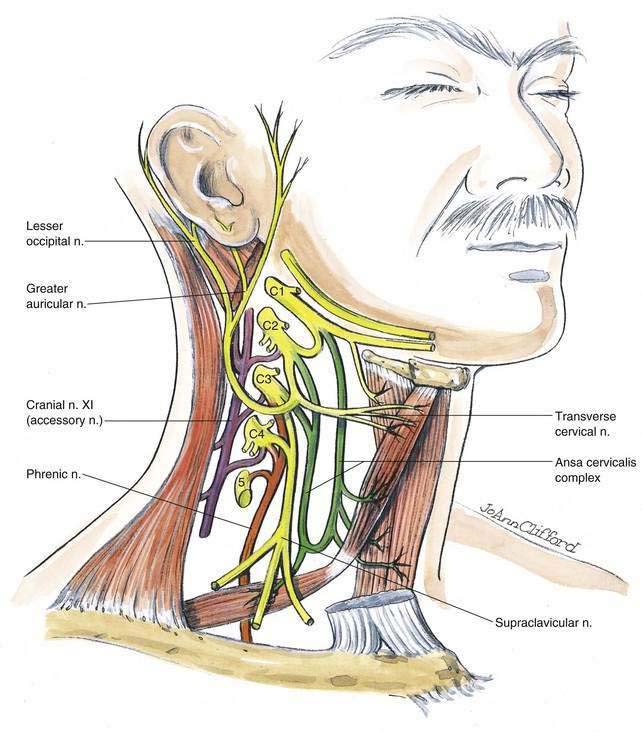
To simplify understanding the cervical plexus, it can be divided into (1) cutaneous branches of the plexus, (2) the ansa cervicalis complex, (3) the phrenic nerve, (4) contributions to the accessory nerve, and (5) direct muscular branches (see Fig. 25-2). The cutaneous branches of the plexus are the lesser occipital, greater auricular, transverse cervical, and supraclavicular nerves (see Fig. 25-1). The first three arise from the second and third cervical nerves, and the supraclavicular nerves arise from the third and fourth cervical nerves. The ansa cervicalis complex provides innervation to the infrahyoid and geniohyoid muscles. The phrenic nerve is the sole motor nerve to the diaphragm and also provides sensation to its central portion. The nerve arises by a large root from the fourth cervical nerve, reinforced by smaller contributions from the third and fifth nerves. Its course takes it to the lateral border of the anterior scalene muscle before it descends vertically over the ventral surface of this muscle and enters the chest along its medial border. The accessory nerve (cranial nerve XI) receives contributions from the cervical plexus at several points and provides innervation to the sternocleidomastoid muscle as well as the trapezius muscles. The direct muscular branches of the plexus supply prevertebral muscles in the neck. The superficial plexus becomes subcutaneous at the midpoint of the posterior border of the sternocleidomastoid muscle (Fig. 25-3, and see Fig. 25-5).
Needle Puncture: Deep Cervical Plexus Block
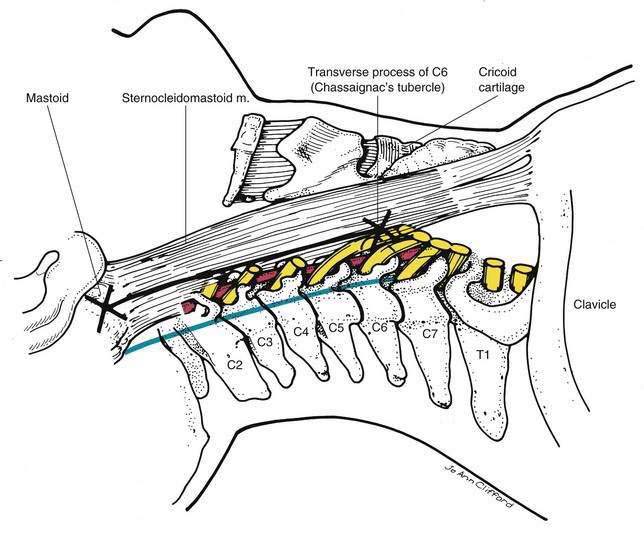
The patient should be positioned with the neck slightly extended and the head turned away from the side to be blocked. A line should be drawn on the skin between the tip of the mastoid process and Chassaignac’s tubercle (i.e., the most easily palpable transverse process of the cervical vertebra, C6). A second line should be drawn parallel and 1 cm posterior to the first line, as illustrated in blue in Figure 25-4. The C4 transverse process should be located by first finding the C2 transverse process 1 to 2 cm caudal to the mastoid process and then identifying C3 and subsequently C4. Each of these transverse processes is palpable approximately 1.5 cm caudal to the immediately more cephalad process. Ultrasonographic guidance can also assist in locating the C4 transverse process. Once the C4 transverse process is identified, a 22-gauge, 5-cm needle is inserted immediately over the C4 transverse process so that it will contact that process at a depth of approximately 1.5 to 3 cm. If a paresthesia is obtained, 10 to 12 mL of local anesthetic is injected at this site. It is helpful to obtain a paresthesia with this technique before injection because one is relying on the continuity of the paravertebral space in the neck to facilitate local anesthetic spread. If a paresthesia is not elicited on the first pass, the needle should be withdrawn and “walked” in a stepwise fashion in an anteroposterior manner. Again, ultrasonographic guidance will also allow you to observe the spread of local anesthetic in the paravertebral space.
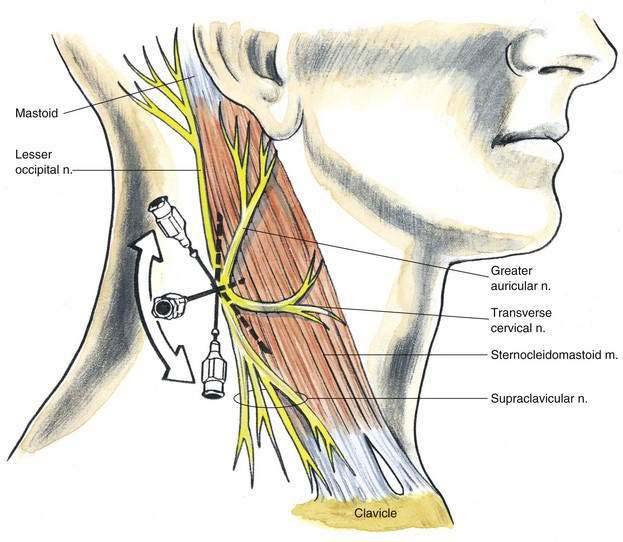
Needle Placement: Superficial Cervical Plexus Block
The superficial cervical plexus block, as illustrated in Figure 25-5, relies on local anesthetic “volume” to be effective. At the midpoint on the posterior border of the sternocleidomastoid muscle, the superficial cervical plexus is arranged such that infiltration deep to the posterior border of the sternocleidomastoid muscle will produce a block. To perform the block, a 22-gauge, 4-cm needle is inserted subcutaneously posterior and immediately deep to the sternocleidomastoid muscle, and 5 mL of local anesthetic is injected. The needle is then redirected both superiorly and inferiorly along the posterior border of the sternocleidomastoid, and 5 mL of solution is injected along each of these sites. In this fashion, a field block of the superficial plexus is created.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
25 Cervical Plexus Block
Placement
Anatomy
Cervical plexus block can be divided into superficial and deep techniques. The cutaneous innervation of the cervical nerves is schematically illustrated in Figure 25-1. The cervical nerves have both dorsal and ventral rami, and those illustrated in Figure 25-2 represent the ventral rami of C1-C4. In addition, there are both sensory and motor branches from the dorsal rami of C1-C4 that are not shown. Before regrouping to form the cervical plexus, the cervical nerves exit from the cervical vertebrae through a gutter in the transverse process in an anterocaudolateral direction, immediately posterior to the vertebral artery.
To simplify understanding the cervical plexus, it can be divided into (1) cutaneous branches of the plexus, (2) the ansa cervicalis complex, (3) the phrenic nerve, (4) contributions to the accessory nerve, and (5) direct muscular branches (see Fig. 25-2). The cutaneous branches of the plexus are the lesser occipital, greater auricular, transverse cervical, and supraclavicular nerves (see Fig. 25-1
[/not-level-membership-for-anesthesiology-category]
