Chapter 69 Cardiac Trauma
3 What is the pattern of injury in BCI?
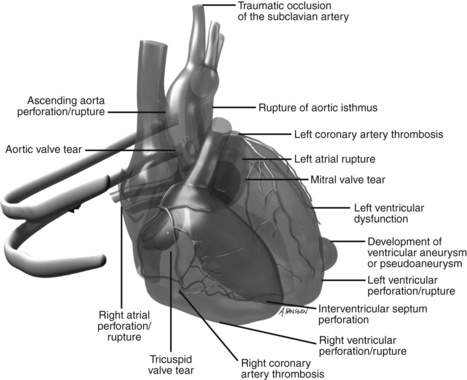
The right side of the heart has the most anterior surface area and therefore is the most commonly injured chamber. Injuries may include rupture of the interventricular septum, a valve, or the ventricle (Fig. 69-1). Patients with a ruptured chamber will rarely reach the hospital alive. Less commonly, injury to coronary arteries occurs that may lead to myocardial infarction. Arrhythmias and decreased contractility may follow myocardial contusion or the previously mentioned injuries.
8 How is echocardiography used in the diagnosis of BCI?
Either form of echocardiography is indicated only if the patient is hemodynamically unstable.
12 When should penetrating cardiac injury (PCI) be suspected?
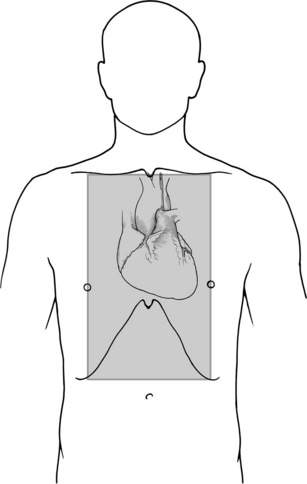
The presentation of PCI is variable and depends on the location of the wound and cardiorespiratory compensation. Any gunshot wound or stab wound to the cardiac box, defined as the region medial to the midclavicular lines, inferior to the clavicles, and superior to the costal margin, is highly concerning for cardiac injury (Fig. 69-2). Of note, an injury outside of the box does not exclude PCI; mortality has been reported as higher for cardiac injuries through wounds outside of the box, possibly because of delayed diagnosis.
16 Describe factors associated with survival in PCI
Key Points Cardiac trauma
1. A sternal fracture should raise the suspicion of cardiac injury, but its absence does not exclude injury.
2. Echocardiography, transthoracic or transesophageal, is a useful diagnostic tool in hemodynamically unstable patients with suspected blunt cardiac injury.
3. Patients with no symptoms and with negative ECG findings during a short observation period may be safely discharged home.
4. Any penetrating injury to the thorax or upper abdomen should raise the suspicion of cardiac injury.
5. FAST examination is the method of choice for diagnosing hemopericardium.
1 Bansal M.K., Maraj S., Chewaproug D., et al. Myocardial contusion injury: redefining the diagnostic algorithm. Emerg Med J. 2005;22:465–469.
2 Chirillo F., Totis O., Cavarzerani A., et al. Usefulness of transthoracic and transoesophageal echocardiography in recognition and management of cardiovascular injuries after blunt chest trauma. Heart. 1996;75:301–306.
3 Degiannis E., Loogna P., Doll D., et al. Penetrating cardiac injuries: recent experience in South Africa. World J Surg. 2006;30:1258–1264.
4 Kang N., Hsee L., Rizoli S., et al. Penetrating cardiac injury: overcoming the limits set by Nature. Injury. 2009;40:919–927.
5 O’Connor J., Ditillo M., Scalea T. Penetrating cardiac injury. J R Army Med Corps. 2009;155:185–190.
6 Prêtre R., Chilcott M. Blunt trauma to the heart and great vessels. N Engl J Med. 1997;336:626–632.
7 Schultz J.M., Trunkey D.D. Blunt cardiac injury. Crit Care Clin. 2004;20:57–70.
8 Türk E.E., Tsokos M. Blunt cardiac trauma caused by fatal falls from height: an autopsy-based assessment of the injury pattern. J Trauma. 2004;57:301–304.
9 Velmahos G.C., Karaiskakis M., Salim A., et al. Normal electrocardiography and serum troponin I levels preclude the presence of clinically significant blunt cardiac injury. J Trauma. 2003;54:45–51.
