Chapter 66 Burns and Frostbite
3 How are thermal injuries classified?




9 Who should be referred to a verified burn center?










11 What is burn-induced hypermetabolism?








12 What are the four main advances in burn care that have dramatically reduced mortality over the last 50 years?




14 How are electrical injuries treated?



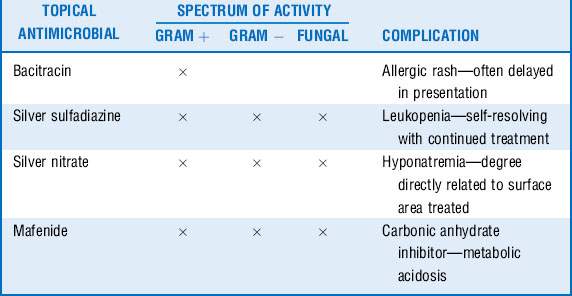
16 What are the known and common complications of topical antimicrobials?
Topical antimicrobial therapy is the mainstay of the treatment for small and large thermal injuries. Although most antimicrobials have a broad range of activity against gram-positive and gram-negative organisms (silver sulfadiazine [Silvadene], silver nitrate, mafenide [Sulfamylon]), some have a narrow spectrum of activity but work well on minor thermal injuries (bacitracin, mupirocin [Bactroban]). As with any pharmacologic agent, a physician must know the indications and potential complications of the agent being prescribed. Although most topical antimicrobials are well tolerated, several have known complications associated with them. See Table 66-1.
Key Points Burns and frostbite
1. Thermal injuries are classified by the extent of damage to the skin’s underlying structure; the physiologic impact is dependent on the extent of second- and third-degree injury.
2. All patients who have a thermal injury should have a complete primary and secondary survey performed with particular attention to airway (potential obstruction) and circulation (potential compartment syndrome).
3. Burn shock is not simply a state of hypovolemia; appropriate resuscitation is mandatory to avoid morbidity and mortality.
4. Burn-induced hypermetabolism is a significant metabolic disturbance following a major thermal injury. Proper nutrition coupled with early excision, grafting, and exercise is the best treatment.
5. Hypocalcemia can develop after exposure to concentrated hydrofluoric acid.
6. Frostbite injuries should be treated with rapid rewarming and potential catheter-directed thrombolysis.
1 American Burn Association. Advanced burn life support providers manual. Chicago: American Burn Association; 2005.
2 Barrow R.E., Jeschke M.G., Herndon D.N. Early fluid resuscitation improves outcomes in severely burned children. Resuscitation. 2000;45:91–96.
3 Bruen K.J., Ballard J.R., Morris S.E., et al. Reduction of the incidence of amputation in frostbite injury with thrombolytic therapy. Arch Surg. 2007;142:546–551.
4 Greenhalgh D.G. Topical antimicrobial agents for burn wounds. Clin Plast Surg. 2009;36:597–606.
5 Hart D.W., Wolf S.E., Chinkes D.L., et al. Effects of early excision and aggressive enteral feeding on hypermetabolism, catabolism, and sepsis after severe burn. J Trauma. 2003;54:755–761.
6 Herndon D.N., Tompkins R.G. Support of the metabolic response to injury. Lancet. 2004;363:1895–1902.
7 Jeschke M.G., Chinkes D.L., Finnery C.C., et al. Pathophysiologic response to severe burn injury. Ann Surg. 2008;248:387–401.
8 Kirkpatrick J.J., Enion D.S., Burd D.A. Hydrofluoric acid burns: a review. Burns. 1995;21:483–493.
9 Klein M.B., Hayden D., Elson C. The association between fluid administration and outcome following major burn: a multicenter study. Ann Surg. 2007;245:622–628.
10 Krammer G.C., Lund T., Beckum O.L. Pathophysiology of burn shock and burn edema. In: Herndon D.N., ed. Total Burn Care. 3rd ed. Philadelphia: Saunders; 2007:93–106.
11 Pham T.N., Gibran N.S., Heimbach D.M. Evaluation of the burn wound: management decisions. In: Herndon D.N., ed. Total Burn Care. 3rd ed. Philadelphia: Saunders; 2007:119–126.
12 Rosen C.L., Adler J.N., Rabban J.T., et al. Early predictors of myoglobinuria and acute renal failure following electrical injury. J Emerg Med. 1999;17:783–789.
13 Sheridan R.L. Comprehensive treatment of burns. Curr Probl Surg. 2001;38:657–756.
14 Sheridan R.L., Ryan C.M., Quinby W.C.Jr. et al: Emergency management of major hydrofluoric acid exposures. Burns. 1995;21:62–64.
15 Sullivan S.R., Ahmadi A.J., Singh C.N., et al. Elevated orbital pressure: another untoward effect of massive resuscitation after burn injury. J Trauma. 2006;60:72–76.
