[level-membership-for-surgery-category]
CHAPTER 22 Breast Reconstruction
INDICATIONS FOR BREAST RECONSTRUCTION
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Patient Positioning and Preparation
Skin-Sparing Mastectomy
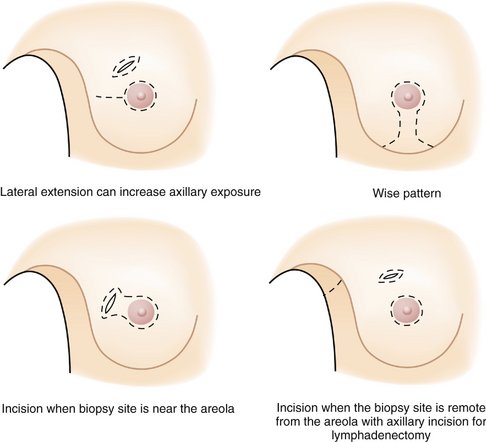
Mastectomy techniques have a significant effect on the outcome of autologous breast reconstruction. Since 1996, the skin-sparing mastectomy has been increasingly used in conjunction with immediate autologous breast reconstruction. A skin-sparing mastectomy is typically performed with a periareolar incision and is so named because the skin envelope of the breast is kept intact during the procedure (Fig. 22-1). Thus, the reconstructive surgeon must simply replace the volume of the mastectomy specimen with either autologous tissue or an implant. This approach avoids the challenges associated with shaping the breast during traditional delayed reconstruction.
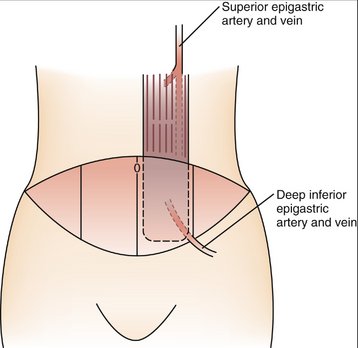
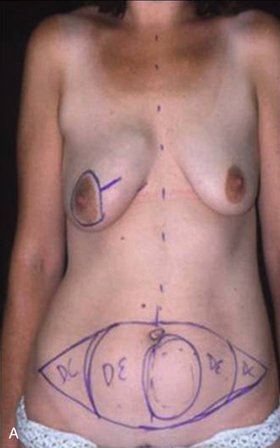
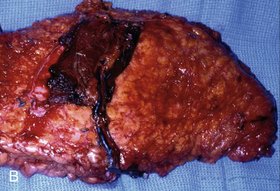
Autologous Reconstruction: TRAM Flap


Implant Reconstruction
Nipple–Areolar Reconstruction
Nipple–areolar reconstruction is usually the final stage of either autologous or implant-based breast reconstruction. Typically, the nipple and areola are fashioned from local tissues. Numerous techniques exist for recreating a nipple. The most commonly performed procedure is the star flap shown in Figure 22-7. The areola can be recreated with either a skin graft taken from the lower abdominal incision or postoperative tattooing.
POSTOPERATIVE COURSE
COMPLICATIONS
Kanchwala SK, Bucky LP. Precision transverse rectus abdominis muscle flap breast reconstruction: A reliable technique for efficient preoperative planning. Ann Plast Surg. 2008;60:521-526.
Serletti JM. Breast reconstruction with the TRAM flap: pedicled and free. J Surg Oncol. 2006;94:532-537.
Sigurdson L, Lalonde DH. Breast reconstruction. Plast Reconstr Surg. 2008;121(1 Suppl):1-12.
Thorne CH, Beasley RW, Aston SJ, et al. Grabb and Smith’s Plastic Surgery, 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 22 Breast Reconstruction
INDICATIONS FOR BREAST RECONSTRUCTION
PREOPERATIVE EVALUATION
COMPONENTS OF THE PROCEDURE AND APPLIED ANATOMY
Patient Positioning and Preparation
Skin-Sparing Mastectomy
Mastectomy techniques have a significant effect on the outcome of autologous breast reconstruction. Since 1996, the skin-sparing mastectomy has been increasingly used in conjunction with immediate autologous breast reconstruction. A skin-sparing mastectomy is typically performed with a periareolar incision and is so named because the skin envelope of the breast is kept intact during the procedure (Fig. 22-1). Thus, the reconstructive surgeon must simply replace the volume of the mastectomy specimen with either autologous tissue or an implant. This approach avoids the challenges associated with shaping the breast during traditional delayed reconstruction.
[/not-level-membership-for-surgery-category]
