Chapter 38 Brain Death and Organ Donation
Brain death is a clinical syndrome in which there is complete and irreversible loss of cortical and brainstem function. Organ donation by deceased donors requires confirmation of brain death, and is clinically, contextually, and temporally separate from transplantation. Donation takes place after the death of a person in an intensive care unit (ICU), most commonly following an intracranial catastrophe, and it involves the patient’s family and the healthcare professionals who have cared for the patient.1 Organ donation is thus an integral part of end-of-life care in the ICU.2 Intensive care physicians are generally supportive of organ donation3 and are obliged to provide leadership in it4 as part of their responsibility for the care of dying patients and their families.
DIAGNOSING BRAIN DEATH
The syndrome of brain death was recognized soon after the establishment of ICUs and before transplantation was established. Despite a number of guidelines for the determination of brain death,5 there remains no single accepted international consensus definition of this syndrome, and codes of practice for the determination of brain death vary slightly internationally, particularly in terms of requirements for repetition and for confirmatory tests (see subsequent material). Nevertheless, all codes of practice contain the following essential common features:
Clinical neurologic examination is the standard for the determination of brain death (Table 38-1). This cannot proceed until the following prerequisites are met:
| Clinical criteria for brain death | Coma of known cause |
| Absence of motor responses | |
| Absence of pupillary responses to light | |
| Absence of corneal reflexes | |
| Absence of caloric reflexes | |
| Absence of gag reflex | |
| Absence of coughing in response to endotracheal suctioning | |
| Absence of sucking and rooting reflexes | |
| Absence of respiratory drive at a PaCO2 >8 kPa (60 mmHg) or 2.7 kPa (20 mmHg) above normal baseline values | |
| Interval between two evaluations according to age |
0 to 2 months: 48 hr |
| 2 months to 1 year: 24 hr | |
| 1 to 18 years: optional | |
| >18 years: optional |
From Wijdicks EF: The diagnosis of brain death. N Engl J Med 344:1215-1221, 2001.
Some codes of practice require that additional special tests (e.g., electroencephalogram and tests of cerebral blood flow) be performed,6 whereas others do not, so brain death should be determined according to locally appropriate codes of practice. When clinical examination cannot be performed (e.g., because of bilateral eye damage) or is confounded (e.g., by prior therapeutic use of high-dose barbiturates), it is necessary to establish that there is no cerebral blood flow by using a confirmatory test such as cerebral angiography, radionuclide cerebral angiography, or a suitably robust alternative method.7
Physiologic Changes in Brain Death
Severe hypertension, tachycardia, and sometimes arrhythmias occur during the final phase of brainstem compression prior to brain death, and although these phenomena may cause temporary reduction of cardiac contractility, treatment is usually not required.8 Should treatment be necessary, a short-acting intravenous β blocker such as esmolol is recommended. A degree of neurogenic pulmonary edema is common with intracranial injuries and should be managed conservatively, by adequate ventilation, cardiovascular support, and the judicious use of diuretics. Neurogenic pulmonary edema usually resolves within 48 to 72 hours and it will be aided by the diuresis, which occurs if diabetes insipidus (see subsequent material) develops.
Pulmonary edema and myocardial dysfunction do not necessarily preclude good subsequent cardiac graft function. Hypertension is soon followed by hypotension (which may be profound if hypovolemia or cardiac dysfunction is also present) and should be promptly treated by volume expansion and vasopressor support. Diabetes insipidus (see Chapter 32) is common and if untreated will rapidly lead to hyperosmolality, hypernatremia, and hypovolemia. Other hormone alterations8,9 do not have therapeutic implications. Oxygen consumption and carbon dioxide production fall by about 40% during the development of brain death,10 and minute ventilation should be reduced accordingly. Hypothermia can occur as the result of the combined effects of cool intravenous fluid infusion, reduced heat production, and loss of both vasomotor tone and shivering-induced thermogenesis. Spontaneous movements and spinal motor reflexes (including bizarre movements) may persist after brain death.5,11 Sympathetic spinal cord reflexes elicited in response to surgical stimulation12 justify the use of anesthetic agents during organ removal.13 A degree of vasoplegia develops because of the reduction in sympathetic tone, and vasopressor support (usually at a low level) is often required to maintain an adequate blood pressure.
STRATEGIES FOR MAINTAINING PHYSIOLOGIC STABILITY
Signs of impending brain death (rising intracranial pressure, progressive coma, pupillary dilatation) should lead to preparation for specific support, including central venous access for inotropic and vasopressor support and pressure measurement, additional intravenous access for rapid volume infusion, and the obtaining of a warming blanket as a source of external heat. Each ICU should have a standardized donor management protocol because, as well as aggressive pharmacologic management of the donor, results in an increased number of transplanted organs.14,15
Ventilatory Management
Ventilatory management should maintain normoxemia and normocarbia, minimize hemodynamic depression and, if possible, preserve the possibility of lung donation. Some oxygenation impairment (e.g., Pao2/FIo2 ratio >33 kPa or 250 mmHg) is tolerable for potential lung donors.16 Moderate tidal volumes (8 ml/kg) and positive end-expiratory pressure (5 cm H2O) may prevent atelectasis, but peak airway pressures above 30 cm H2O should be avoided. Changes of patient position and endotracheal suctioning should continue. Higher levels of positive end-expiratory pressure (10 to 12 cm H2O) may be required to prevent pulmonary edema or provide adequate oxygenation when lung dysfunction is severe. Testing such patients for apnea without producing hypoxemia may require prior mechanical hypoventilation to raise the Paco2 as well as continuous positive airway pressure to maintain Pao2 during the period of apnea.
Hemodynamic Management
Hemodynamic management should maintain adequate organ perfusion and arterial pressure without fluid overload or excessive vasoconstriction and should preserve the possibility of cardiac donation. Reasonable hemodynamic goals include a mean arterial pressure above 65 mmHg, a heart rate of 100 or less, and central venous pressure of 8 mmHg. Some inotropic support (with pressor activity) is usually required. Norepinephrine (usually less than 0.1 μg/kg/min) is widely used for this purpose. After an acceptable mean arterial pressure has been obtained, the hemodynamic response to a volume challenge should be assessed. Dopamine may produce an unwanted polyuria and epinephrine unwanted metabolic effects (see Chapter 3). Low-dose vasopressin (0.5 to 1 unit/hr; compare this to the dosage used to treat vasoplegic shock, described in Chapter 3) is effective in reducing catecholamine requirements17,18 without apparent detriment to subsequently transplanted organs,17 and it should be used after adequate volume loading if catecholamine requirements are high.
Hypovolemia and hemoconcentration should be corrected with resuscitation fluids.19 Crystalloid infusion may worsen pulmonary function20 and somewhat larger volumes (1.3 times more21) may be required than if colloid is used. The effects of hydroxyethylstarch on subsequent kidney graft function are debated,22,23 but moderate volumes are commonly given. Anemia is well tolerated in brain death, but red blood cells may be given to maintain the hematocrit at about 0.25, pending organ retrieval. Hyperosmolarity (>310 mOsm/l, corresponding to serum sodium >155 mmol/l) should be prevented by the administration of free water (1 to 2 ml/kg/hr as 5% dextrose) because severe donor hyperosmolality is associated with poor liver graft function.
Metabolic Management
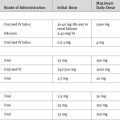
Control of diabetes insipidus minimizes the risks for developing hyperosmolality,24 hypovolemia, or hyperglycemia (secondary to the infusion of large volumes of 5% dextrose). Between 4 and 8 μg of desmopressin, a synthetic analogue of vasopressin, administered intravenously, provides effective control of diabetes insipidus for 6 to 8 hours. Treatment is usually commenced when urine output exceeds 200 to 300 ml/hr and may be repeated if necessary. Effective antidiuresis is also provided by low-dose intravenous vasopressin described earlier. Failure to control diabetes insipidus leads to an increased requirement for free water to control osmolarity, and if 5% dextrose is used as replacement fluid, a hyperglycemic diuresis may result.
Hypothermia develops easily after brain death. Maintaining a high ambient temperature (24°C), warming infused fluids, and using heated humidifiers and external warming systems are useful preventive strategies. Core temperature should be kept above the 35°C to 36.5°C required to confirm brain death. Low-dose insulin infusion may be required to prevent hyperglycemia. Potassium should be supplemented to keep the plasma potassium concentration above 3.5 mmol/l, but hyperkalemia is not uncommon and may be more easily produced after brain death. Correction of hypophosphatemia does not improve hemodynamics in brain death.25
Hormonal resuscitation using an intravenous bolus of methylprednisolone, infusions of vasopressin, and either triiodothyronine or l-thyroxine have been reported to increase the number of transplanted hearts and significantly improve short-term graft function.26 This strategy should be considered in donors who fail conventional resuscitation measures using fluid and low-dose (less than 10 μg/kg/min of dopamine equivalent) vasopressor support. However, combined hormonal treatment remains controversial, and prospective randomized trials are needed.27
CONTRAINDICATIONS TO ORGAN DONATION
Organ donation is possible in most situations in which brain death has been confirmed. Absolute contraindications to organ donation are confined to situations where there is an unacceptably high risk for transmission of malignancy or infection and where the functioning of all possible donor organs is unacceptably poor. Although infection by human immunodeficiency virus infection is likely to remain an absolute contraindication, advanced age, recent bacterial sepsis, positive hepatitis B or C serology, and some prior extracranial malignancies are not. Issues specific to the lungs and the heart are discussed in Chapters 13 and Chapter 14, respectively.
INTERACTIONS WITH FAMILIES
Most ICUs admit patients with very severe brain damage and low probabilities of survival, some of whom become brain dead. The primary indication for ICU admission is to identify that small subgroup of patients who may do well and to treat them accordingly. For those patients who go on to die, this short time in the ICU allows for compassionate end-of-life care, which is much appreciated by families (see Chapter 39).28
The intensivist must convey the fact of brain death and its implications to the family. It can be difficult for families to accept brain death as death, given the appearance of the skin, the movement of the chest, and the warmth of the hands during continued ventilatory and circulatory support. Intensive care physicians should be open to offering family members the opportunity to view the (perhaps second) clinical examination for brain death or the images of the cerebral arteriogram where clinical examination is confounded. Such visual experiences may help family to understand and accept the final implication of the diagnosis of brain death.
The intensivist should initiate a discussion about organ donation after this acceptance has occurred. Defining the discussion as “offering the option of organ donation” rather than “obtaining consent” or “persuasion” is not coercive in language and frees the intensivist to provide complete and unbiased information and to support the family in the decision-making process. They may take into account previously expressed wishes, previous family discussions, personal and family values, and cultural and religious beliefs.4
Some countries, particularly in Europe, “presume consent,” and the discussion may focus on whether the patient had expressed an objection during life29 or on whether the family objects. However, there is no evidence that such “opting-out” systems guarantee higher donation rates.30
Should organ donation proceed, physiologic stability will have to be maintained, often for a period of about 12 hours, until organ removal in the operating room. An opportunity should be made for the family to spend time with the patient after organ removal.31
1 Williams MA, Lipsett PA, Rushton CH, et al. The physician ’s role in discussing organ donation with families. Crit Care Med. 2003;31:1568-1573.
2 Truog RD, Cist AF, Brackett SE, et al. Recommendations for end-of-life care in the intensive care unit: The Ethics Committee of the Society of Critical Care Medicine. Crit Care Med. 2001;29:2332-2348.
3 Pearson IY, Zurynski Y. A survey of personal and professional attitudes of intensivists to organ donation and transplantation. Anaesth Intens Care. 1995;23:68-74.
4 Streat S. Clinical review: moral assumptions and the process of organ donation in the intensive care unit. Crit Care. 2004;8:382-388.
5 Wijdicks EF. The diagnosis of brain death. N Engl J Med. 2001;344:1215-1221.
6 Waters CE, French G, Burt M. Difficulty in brainstem death testing in the presence of high spinal cord injury. Br J Anaesth. 2004;92:760-764.
7 Qureshi AI, Kirmani JF, Xavier AR, et al. Computed tomographic angiography for diagnosis of brain death. Neurology. 2004;62:652-653.
8 Karayalcin K, Umana JP, Harrison JD, et al. Donor thyroid function does not affect outcome in orthotopic liver transplantation. Transplantation. 1994;57:669-672.
9 Goarin JP, Cohen S, Riou B, et al. The effects of triiodothyronine on hemodynamic status and cardiac function in potential heart donors. Anesth Analg. 1996;83:41-47.
10 Bitzani M, Matamis D, Nalbandi V, et al. Resting energy expenditure in brain death. Intens Care Med. 1999;25:970-976.
11 Ropper AH. Unusual spontaneous movements in brain-dead patients. Neurology. 1984;34:1089-1092.
12 Gramm HJ, Zimmermann J, Meinhold H, et al. Hemodynamic responses to noxious stimuli in brain-dead organ donors. Intens Care Med. 1992;18:493-495.
13 Young PJ, Matta BF. Anaesthesia for organ donation in the brainstem dead —why bother ? Anaesthesia. 2000;55:105-106.
14 Rosendale JD, Chabalewski FL, McBride MA, et al. Increased transplanted organs from the use of a standardized donor management protocol. Am J Transplant. 2002;2:761-768.
15 Rosendale JD, Kauffman HM, McBride MA, et al. Aggressive pharmacologic donor management results in more transplanted organs. Transplantation. 2003;75:482-487.
16 Shumway SJ, Hertz MI, Petty MG, et al. Liberalization of donor criteria in lung and heart-lung transplantation. Ann Thorac Surg. 1994;57:92-95.
17 Katz K, Lawler J, Wax J, et al. Vasopressin pressor effects in critically ill children during evaluation for brain death and organ recovery. Resuscitation. 2000;47:33-40.
18 Chen JM, Cullinane S, Spanier TB, et al. Vasopressin deficiency and pressor hypersensitivity in hemodynamically unstable organ donors. Circulation. 1999;100:II244-II246.
19 Chen EP, Bittner HB, Kendall SW, et al. Hormonal and hemodynamic changes in a validated animal model of brain death. Crit Care Med. 1996;24:1352-1359.
20 Pennefather SH, Bullock RE, Dark JH. The effect of fluid therapy on alveolar arterial oxygen gradient in brain-dead organ donors. Transplantation. 1993;56:1418-1422.
21 Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med. 2004;350:2247-2256.
22 Cittanova ML, Leblanc I, Legendre C, et al. Effect of hydroxyethylstarch in brain-dead kidney donors on renal function in kidney-transplant recipients. Lancet. 1996;348:1620-1622.
23 Deman A, Peeters P, Sennesael J. Hydroxyethyl starch does not impair immediate renal function in kidney transplant recipients: a retrospective, multicentre analysis. Nephrol Dial Transplant. 1999;14:1517-1520.
24 Totsuka E, Dodson F, Urakami A, et al. Influence of high donor serum sodium levels on early postoperative graft function in human liver transplantation: effect of correction of donor hypernatremia. Liver Transplant Surg. 1999;5:421-428.
25 Riou B, Kalfon P, Arock M, et al. Cardiovascular consequences of severe hypophosphataemia in brain-dead patients. Br J Anaesth. 1995;74:424-429.
26 Rosendale JD, Kauffman HM, McBride MA, et al. Hormonal resuscitation yields more transplanted hearts, with improved early function. Transplantation. 2003;75:1336-1341.
27 Wood KE, Becker BN, McCartney JG, et al. Care of the potential organ donor. N Engl J Med. 2004;351:2730-2739.
28 Cuthbertson SJ, Margetts MA, Streat SJ. Bereavement follow-up after critical illness. Crit Care Med. 2000;28:1196-1201.
29 Manaouil C, Chatelain D, Montpellier D, et al. New French legislation governing organ removals for therapeutic and scientific purposes. Med Law. 2005;24:585-603.
30 Coppen R, Friele RD, Marquet RL, et al. Opting-out systems: no guarantee for higher donation rates. Transplant Int. 2005;18:1275-1279.
31 Douglass GE, Daly M. Donor families ’ experience of organ donation. Anaesth Intens Care. 1995;23:96-98.