Chapter 12 Bones and joints
Imaging modalities
MUSCULOSKELETAL MAGNETIC RESONANCE IMAGING – GENERAL POINTS
Arthrography – General Points
ARTHROGRAPHY
Indications
Contrast medium
Radiographic views
1 Binkert C.A., Verdun F.R., Zanetti M., et al. CT arthrography of the glenohumeral joint: CT fluoroscopy versus conventional CT and fluoroscopy – comparison of image guidance techniques. Radiology. 2003;229:153-158.
2 Binkert C.A., Zanetti M., Hodler J. Patient’s assessment of discomfort during MR arthrography of the shoulder. Radiology. 2001;221:775-778.
3 Hugo P.C., Newberg A.H., Newman J.S., et al. Complications of arthrography. Sem. Musculoskelet. Radiol.. 1998;2:345-348.
Andreisek G., Duc S.R., Froehlich J.M., et al. MR arthrography of the shoulder, hip, and wrist: evaluation of contrast dynamics and image quality with increasing injection-to-imaging time. Am. J. Roentgenol.. 2007;188:1081-1088.
Tehranzadeh J., Mossop E.P., Golshan-Momeni M. Therapeutic arthrography and bursography. Orthop. Clin. North Am.. 2006;37:393-408.
Arthrography – Site Specific Issues
There are various needle approaches using image guidance and the most commonly used ones are described.
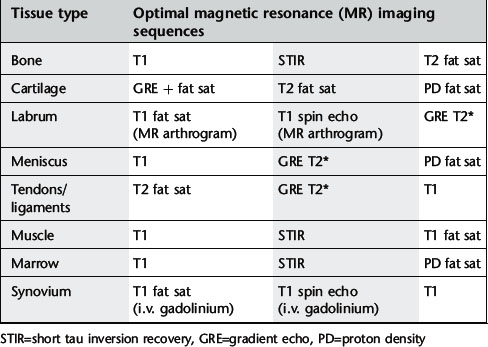
KNEE
Technique
Coumas J.M., Palmer W.E. Knee arthrography. Evolution and current status. Radiol. Clin. North Am.. 1998;36(4):703-728.
De Filippo M., Bertellini A., Pogliacomi F., et al. Multidetector CT arthrography of the knee: diagnostic accuracy and indications. Eur. J. Radiol.. 2008. March 6. Epub
Mutschler C., Vande Berg B.C., Lecouvet F.E., et al. Postoperative meniscus: assessment at dual detector row spiral CT arthrography of the knee. Radiology. 2003;228:635-641.
Hip
Technique

Radiographic views in the paediatric hip arthrogram
In children under the age of 10 years the procedure is usually done under general anaesthesia. A fuller conventional radiographic series is needed to assess the joint dynamics to help in the evaluation of treatment options particularly in developmental dysplasia of the hip:
Aliabadi P., Baker N.D., Jaramillo D. Hip arthrography, aspiration, block, and bursography. Radiol. Clin. North Am.. 1998;36(4):673-690.
Devalia K.L., Wright D., Sathyamurthy P., et al. Role of preoperative arthrography in early Perthes disease as a decision making tool. Is it really necessary? J. Pediatr. Orthop. B. 2007;16:196-200.
Grissom L., Harcke H.T., Thacker M. Imaging in the surgical management of developmental dislocation of the hip. Clin. Orthop. Relat. Res.. 2008;466:791-801.
Llopis E., Cerezal L. Direct MR arthrography of the hip with leg traction: feasibility for assessing articular cartilage. Am. J. Roentgenol.. 2008;190:1124-1128.
Temmerman O.P., Raijmakers P.G., Deville W., et al. The use of plain radiography, subtraction arthrography, nuclear arthrography, and bone scintigraphy in the diagnosis of a loose acetabular component of a total hip prosthesis: a systematic review. J. Arthroplasty. 2007;22:818-827.
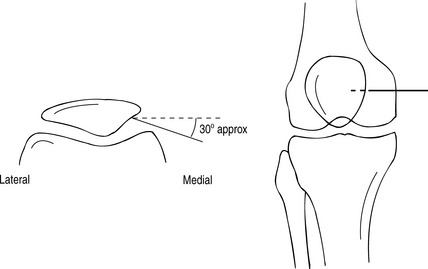
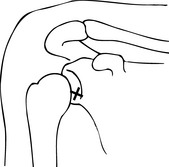
Shoulder
Technique
Chung C.B., Dwek J.R., Feng S., et al. MR arthrography of the glenohumeral joint: a tailored approach. Am. J. Roentgenol.. 2001;177(1):217-219.
Dépelteau H., Bureau N.J., Cardinal E., et al. Arthrography of the shoulder: a simple fluoroscopically guided approach for targeting the rotator cuff interval. Am. J. Roentgenol.. 2004;182(2):329-332.
Farmer K.D., Hughes P.M. MR arthrography of the shoulder: fluoroscopically guided technique using a posterior approach. Am. J. Roentgenol.. 2002;178(2):433-434.
Schneider R., Ghelman B., Kaye J.J. A simplified injection technique for shoulder arthrography. Radiology. 1975;114(3):738-739.
Elbow
Technique
Single contrast

Dubberley J.H., Faber K.J., Patterson S.D., et al. The detection of loose bodies in the elbow: the value of MRI and CT arthrography. J. Bone Joint. Surg. Br.. 2005;87:684-686.
Steinbach L.S., Schwartz M. Elbow arthrography. Radiol. Clin. North Am.. 1998;36(4):635-649.
Waldt S., Bruegel M. Comparison of multislice CT arthrography and MR arthrography for the detection of articular cartilage lesions of the elbow. Eur. Radiol.. 2005;15:784-791.
Wrist
Technique
Radiocarpal joint
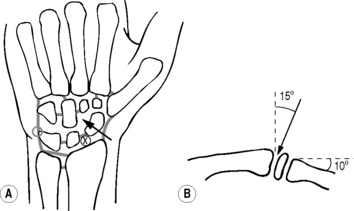
Midcarpal joint
Joshy S., Ghosh S., Lee K., et al. Accuracy of direct MR arthrography in the diagnosis of triangular fibrocartilage complex tears of the wrist. Int. Orthop.. 2008;32:251-253.
Linkous M.D., Gilula L.A. Wrist arthrography today. Radiol. Clin. North Am.. 1998;36(4):651-672.
Moser T., Dosch J.C., Moussaoui A., et al. Wrist ligament tears: evaluation with MRI and combined MDCT and MR arthrography. Am. J. Roentgenol.. 2007;188:1278-1286.
Ruegger C., Schmid M.R., Pfirrmann C.W., et al. Peripheral tear of the triangular fibrocartilage: depiction with MR arthrography of the distal radioulnar joint. Am. J. Roentgenol.. 2007;188:187-192.
Tirman R.M., Weber E.R., Snyder L.L., et al. Midcarpal wrist arthrography for the detection of tears of the scapholunate and lunotriquetral ligaments. Am. J. Roentgenol.. 1985;144:107-108.
Ankle
Technique

Cerezal L., Abascal F., García-Valtuille R., et al. Ankle MR arthrography: how, why and when? Radiol. Clin. North Am.. 2005;43:693-707.
Davies A.M., Cassar-Pullicino V.N. Demonstration of osteochondritis dissecans of the talus by coronal computed tomographic arthrography. Br. J. Radiol.. 1989;62(744):1050-1055.
Schmid M.R., Pfirrmann C.W., Hodler J., et al. Cartilage lesions in the ankle joint: comparison of MR arthrography and CT arthrography. Skeletal Radiol.. 2003;32:259-265.
Tendon Imaging
ULTRASOUND OF THE PAEDIATRIC HIP
Technique
Developmental dysplasia of the hip
With US the unossified elements of the hip – femoral head, greater trochanter, labrum, triradiate cartilage – as well as the bony acetabular roof, can be identified in the first 6 months of life.1 After 9–12 months, the degree of ossification precludes adequate imaging by US and plain film radiography becomes superior. There are two main methods, static and dynamic, and both may be used during one examination.
Hip-joint effusion
Approximately 50% of children with acute hip pain have intra-articular fluid3 and the sensitivity of US for detecting effusion approaches 100%. With the child supine, the hip is scanned anteriorly with the transducer parallel to the femoral neck. Bulging of the anterior portion of the joint capsule can be readily identified.4 The normal distance between the bony femoral neck and the joint capsule is always less than 3 mm, and the difference between the affected and unaffected sides should not be greater than 2 mm.
1 Yousefzadeh D.K., Ramilo J.L. Normal hip in children: correlation of US with anatomic and cryomicrotome sections. Radiology. 1987;165:647-655.
2 Clarke N.M., Harcke H.T., McHugh P., et al. Real time ultrasound in the diagnosis of congenital dislocation and dysplasia of the hip. J. Bone Joint Surg. Br.. 1985;67:406-412.
3 Dörr U., Zieger M., Hauke H. Ultrasonography of the painful hip. Prospective studies in 204 patients. Pediatr. Radiol.. 1988;19:36-40.
4 Miralles M., Gonzalez G., Pulpeiro J.R., et al. Sonography of the painful hip in children: 500 consecutive cases. Am. J. Roentgenol.. 1989;152:579-582.
Radionuclide Bone Scan
Radiopharmaceuticals
99mTc-methylene diphosphonate (MDP) or other 99mTc-labelled diphosphonate, 500 MBq typical, 600 MBq max (3 mSv ED). For single photon emission computed tomography (SPECT) 800 MBq (5 mSv ED).
Technique
Images
Standard
High-resolution images are acquired with a pixel size of 1–2 mm:
Analysis
1 Murray I.P., Dixon J. The role of single photon emission computed tomography in bone scintigraphy. Skeletal Radiol.. 1989;18:493-505.
2 Utsunomiya D., Shiraishi S., Imuta M., et al. Added value of SPECT/CT fusion in assessing suspected bone metastasis: comparison with scintigraphy alone and nonfused scintigraphy and CT. Radiology. 2006;238:264-271.



