Chapter 54 Blood Products and Coagulation
3 What are the main red blood cell surface antigen systems?
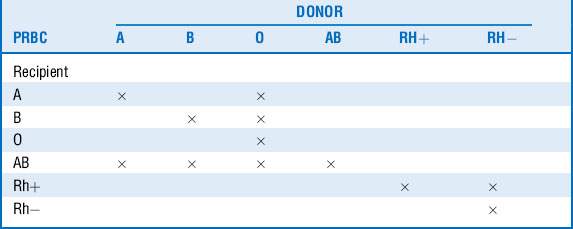
An individual’s red cells may express A, B, both, or no surface antigens, which determine that individual’s blood type. Those who do not express an antigen will eventually develop antibodies against it. People carrying anti-A or anti-B antibodies cannot receive red blood cells with the corresponding surface antigens, or immunologic destruction of the transfused red cells may occur. Consequently, type O individuals are considered universal donors, whereas AB individuals may donate only to other AB recipients. Similar to the ABO system, a separate Rh surface antigen exists that may be either present (Rh+) or absent (Rh−) from the red cell plasma membrane. Individuals who are Rh negative will develop antibodies to the Rh factor when exposed to Rh+ blood. This is not a problem with the initial exposure, but hemolysis may occur with subsequent transfusions (Table 54-1).
5 What are potential transfusion hazards?









10 What are the infectious risks of transfusion?




13 What are the most commonly used techniques of autologous transfusion?
 Preoperative autologous blood donation (PABD). Blood is donated at frequent intervals (as often as every 3 days) starting 4 to 6 weeks before surgery and transfused after surgery as needed. Benefits include freedom from hemolytic, allergic, and febrile reactions, as well as alloimmunization and transfusion-related infections.
Preoperative autologous blood donation (PABD). Blood is donated at frequent intervals (as often as every 3 days) starting 4 to 6 weeks before surgery and transfused after surgery as needed. Benefits include freedom from hemolytic, allergic, and febrile reactions, as well as alloimmunization and transfusion-related infections.


14 What else can be done to minimize blood loss and transfusion requirements?
 Antifibrinolytic agents (ε-aminocaproic acid and tranexamic acid [TXA]) are synthetic lysine analogs that have been used extensively, mainly in cardiac surgery, to minimize blood loss and decrease transfusion requirements. They also appear to minimize blood loss and improve survival in trauma patients, and their use has been increasing in the field. (Aprotinin, an older-generation antifibrinolytic, was withdrawn from the market in 2008 when it was found to be associated with a higher risk for cardiovascular complications and death). A recent multiinstitutional large prospective randomized clinical trial has shown survival advantage in trauma patients treated early with TXA.
Antifibrinolytic agents (ε-aminocaproic acid and tranexamic acid [TXA]) are synthetic lysine analogs that have been used extensively, mainly in cardiac surgery, to minimize blood loss and decrease transfusion requirements. They also appear to minimize blood loss and improve survival in trauma patients, and their use has been increasing in the field. (Aprotinin, an older-generation antifibrinolytic, was withdrawn from the market in 2008 when it was found to be associated with a higher risk for cardiovascular complications and death). A recent multiinstitutional large prospective randomized clinical trial has shown survival advantage in trauma patients treated early with TXA.










17 What is FFP?
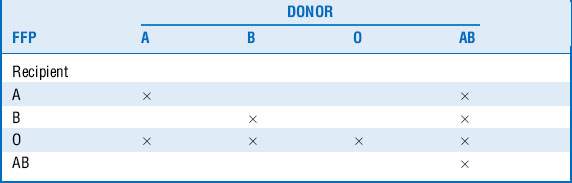
FFP is plasma obtained from single units of whole blood collected by apheresis. It is frozen and maintained at −18° to −30° C to preserve the labile coagulation factors. FFP contains all of the coagulation factors present in blood, along with antithrombin III and proteins C and S, at near-physiologic concentrations. It has a half life of approximately 1 year and has to be thawed before administration. It has to be matched for ABO system compatibility (Table 54-2) but not Rh compatibility.







21 What is measured by prothrombin time (PT)? What is international normalized ratio (INR)?





28 What is damage control resuscitation?
The basic tenets of damage control resuscitation are as follows:
 Avoid crystalloid resuscitation.
Avoid crystalloid resuscitation.
 Aim for permissive hypotension whenever possible.
Aim for permissive hypotension whenever possible.
 Prevent coagulopathy through early use of blood products.
Prevent coagulopathy through early use of blood products.
 Aggressively break the vicious cycle of acidosis, coagulopathy, and hypothermia.
Aggressively break the vicious cycle of acidosis, coagulopathy, and hypothermia.
Key Points Blood Products and Coagulation
1. Controlling the bleeding is more important than replacing the losses.
2. Blood products carry significant risks. Transfuse only when necessary.
3. Know the mechanism of warfarin and heparin anticoagulants and how they can be reversed.
4. Early use of blood component therapy can prevent development of coagulopathy in massively bleeding patients.
5. Excessive crystalloid resuscitation can worsen coagulopathy.
1 Alter H.J., Stramer S.L., Dodd R.Y. Emerging infectious diseases that threaten the blood supply. Semin Hematol. 2007;44:32–41.
2 Brown C.V., Foulkrod K.H., Sadler H.T., et al. Autologous blood transfusion during emergency trauma operations. Arch Surg. 2010;145:690–694.
3 Carless P.A., Henry D.A., Carson J.L., et al. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev. 10, 2010. CD002042, 2010
4 Carson J.L., Noveck H., Berlin J.A., et al. Mortality and morbidity in patients with very low postoperative hemoglobin levels who decline blood transfusion. Transfusion. 2002;42:812–818.
5 CRASH-2 trial collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376:23–32.
6 Duchesne J.C., Hunt J.P., Wahl G., et al. Review of current blood transfusions strategies in a mature level I trauma center: were we wrong for the last 60 years? J Trauma. 2008;65:272–276.
7 Hauser C.J., Boffard K., Dutton R., et al. Results of the CONTROL trial: efficacy and safety of recombinant activated factor VII in the management of refractory traumatic hemorrhage. J Trauma. 2010;69:489–500.
8 Henry D.A., Carless P.A., Moxey A.J., et al. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 3, 2011. CD001886, 2011
9 Holcomb J.B., Wade C.E., Michalek J.E., et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248:447–458.
10 Inaba K., Lustenberger T., Rhee P., et al. The impact of platelet transfusion in massively transfused trauma patients. J Am Coll Surg. 2010;211:573–579.
11 Kennedy L.D., Case L.D., Hurd D.D., et al. A prospective, randomized, double-blind controlled trial of acetaminophen and diphenhydramine pretransfusion medication versus placebo for the prevention of transfusion reactions. Transfusion. 2008;48:2285–2291.
12 Levi M., Levy J.H., Andersen H.F., et al. Safety of recombinant activated factor VII in randomized clinical trials. N Engl J Med. 2010;363:1791–1800.
13 Martí-Carvajal A.J., Solà I., González L.E., et al. Pharmacological interventions for the prevention of allergic and febrile non-haemolytic transfusion reactions. Cochrane Database Syst Rev. 6, 2010. CD007539, 2010
14 Roberts I., Shakur H., Ker K., et al. Antifibrinolytic drugs for acute traumatic injury. Cochrane Database Syst Rev. 1, 2011. CD004896, 2010
15 Schulman S., Kearon C., Kakkar A.K., et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med. 2009;361:2342–2352.
16 Vanderlinde E.S., Heal J.M., Blumberg N. Autologous transfusion. BMJ. 2002;324:772–775.
