Chapter 37 Bioterrorism
2 What are some possible agents that might be used in an attack?
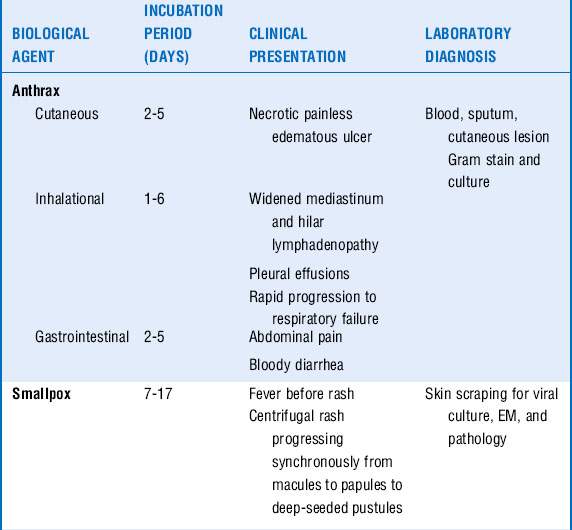
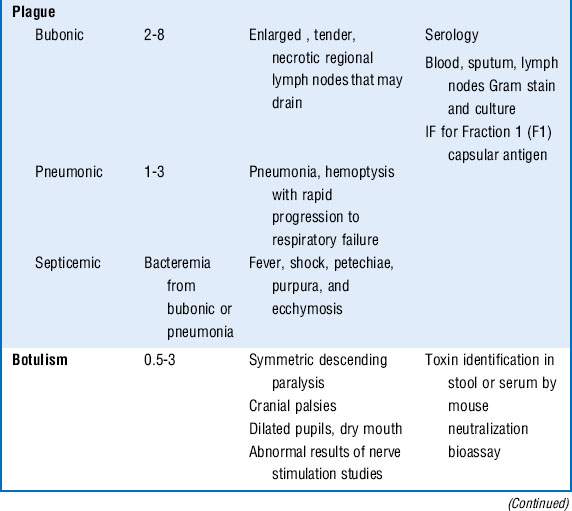
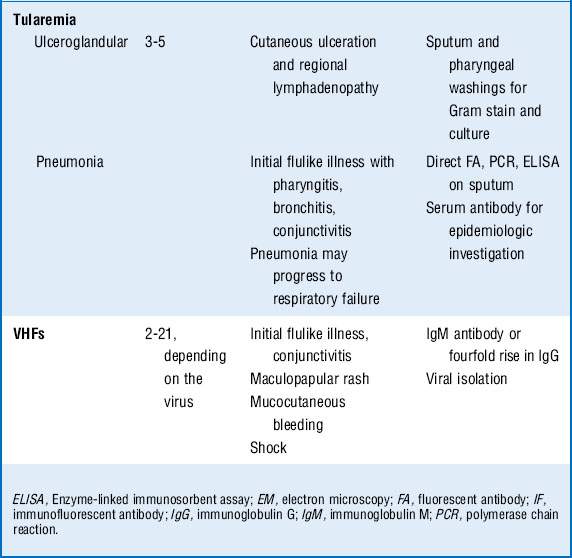
The CDC classifies six pathogens as class A bioterrorism agents: smallpox, plague, botulism, tularemia, viral hemorrhagic fever (VHF), and anthrax. These agents are considered to have the greatest potential for mass casualties, large-scale dissemination, and public panic and social disruption. All of them except VHF have been developed as biological weapons. They are stable in aerosol form and would be most likely delivered in this manner. Most of the civilian population remains susceptible to them, and most cause illnesses not typically seen by providers, causing delayed or missed diagnoses. The major clinical syndromes are summarized in Table 37-1.
3 What are clues to a biological attack?
Recognition of a biological attack may be delayed until patients begin accessing medical care, which may be days to weeks after the event depending on the incubation period of the pathogen (Table 37-1). Features that might suggest a biological attack include the following:






4 What pathogens would present with respiratory failure?
 Anthrax: Pneumonic anthrax is caused by the inhalation of the spore form of Bacillus anthracis. It begins as a nonspecific influenza-like illness with fever, cough, malaise, headache, and vomiting. Rapid progression occurs to hemorrhagic mediastinitis, hilar lymph node enlargement, respiratory failure, hemodynamic collapse, and death. Although chest radiographs classically show only a widened mediastinum without pulmonary infiltrates, several of the victims from the anthrax letter attacks in the fall of 2001 did have pulmonary infiltrates and pleural effusions. Bacteremia and meningitis can occur.
Anthrax: Pneumonic anthrax is caused by the inhalation of the spore form of Bacillus anthracis. It begins as a nonspecific influenza-like illness with fever, cough, malaise, headache, and vomiting. Rapid progression occurs to hemorrhagic mediastinitis, hilar lymph node enlargement, respiratory failure, hemodynamic collapse, and death. Although chest radiographs classically show only a widened mediastinum without pulmonary infiltrates, several of the victims from the anthrax letter attacks in the fall of 2001 did have pulmonary infiltrates and pleural effusions. Bacteremia and meningitis can occur.


5 What pathogens would present with shock?


7 What pathogens may present with predominantly cutaneous manifestations?
 Smallpox, caused by the DNA virus variola major, is acquired via inhalation of infectious droplets aerosolized by affected patients. Typically a prodrome of fever, chills, myalgias, and headache occurs over 2 to 4 days, followed by the eruption of intraoral macules. A maculopapular rash develops on the face, which then progresses in a centrifugal manner to involve the extremities and finally the trunk. The rash progresses to deep-seated vesicles and pustules over 8 to 10 days. Complications include bacterial superinfections, fluid and electrolyte abnormalities, desquamation, panophthalmitis, residual scarring, and death. Secondary bacterial infections involving the skin or lungs may occur and are often complicated by bacteremia and sepsis.
Smallpox, caused by the DNA virus variola major, is acquired via inhalation of infectious droplets aerosolized by affected patients. Typically a prodrome of fever, chills, myalgias, and headache occurs over 2 to 4 days, followed by the eruption of intraoral macules. A maculopapular rash develops on the face, which then progresses in a centrifugal manner to involve the extremities and finally the trunk. The rash progresses to deep-seated vesicles and pustules over 8 to 10 days. Complications include bacterial superinfections, fluid and electrolyte abnormalities, desquamation, panophthalmitis, residual scarring, and death. Secondary bacterial infections involving the skin or lungs may occur and are often complicated by bacteremia and sepsis.


8 What initial steps should be taken if a patient is suspected to be a victim of a bioterrorist attack?
If the biological agent is known, appropriate isolation and infection control measures should be implemented as outlined in Table 37-2.
Table 37-2 Infection Control for Category a Biological Weapons
| Disease | Mode of transmission | Precautions |
|---|---|---|
| Anthrax | ||
| Pulmonary | Inhalation of spores |
9 What infection control measures need to be taken in the ICU?
The biological agents that pose a transmission threat to health care workers in the ICU include smallpox, plague, and VHFs. Anthrax, botulism, and tularemia are not transmissible to health care workers in the ICU setting. See Table 37-2. Infection control precautions include the following:




10 How should the patient be treated (Table 37-3)?
 Anthrax: Cutaneous anthrax can usually be treated with prolonged oral antibiotics for 60 days. Pneumonic anthrax and severe cutaneous disease should initially be treated with intravenous ciprofloxacin or doxycycline coupled with one or two additional agents such as vancomycin, rifampin, or imipenem-cilastatin. Transition to oral ciprofloxacin or doxycycline can be made when the patient is clinically stable. Total treatment should last for 60 days.
Anthrax: Cutaneous anthrax can usually be treated with prolonged oral antibiotics for 60 days. Pneumonic anthrax and severe cutaneous disease should initially be treated with intravenous ciprofloxacin or doxycycline coupled with one or two additional agents such as vancomycin, rifampin, or imipenem-cilastatin. Transition to oral ciprofloxacin or doxycycline can be made when the patient is clinically stable. Total treatment should last for 60 days.

 Plague: Intravenous antibiotics should be administered for 7 days.
Plague: Intravenous antibiotics should be administered for 7 days.
 Tularemia: Intravenous antibiotics should be given for 10 to 14 days.
Tularemia: Intravenous antibiotics should be given for 10 to 14 days.


11 What postexposure prophylaxis (PEP) should be used?
PEP against the category A agents is summarized in Table 37-3.
| Pathogen | Treatment | Postexposure prophylaxis (all administered orally) |
|---|---|---|
| Anthrax | ||
bid, Twice daily; IV, intravenously; PO, orally; tid, three times daily.
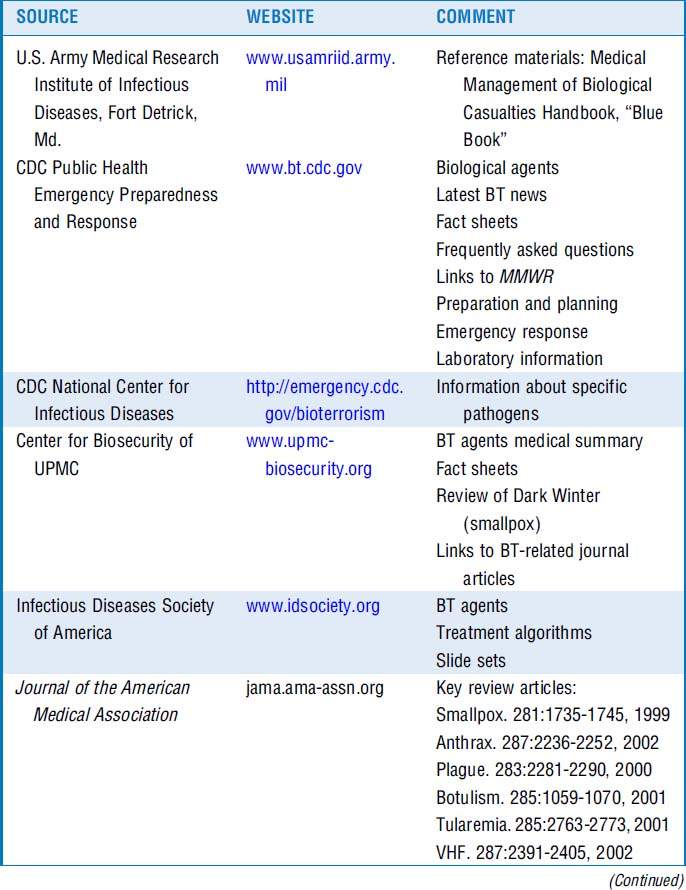
12 What web-based resources can I access?
Resources are listed in Table 37-4.

Key Points Clues to Recognition of a Biological Attack
Clues to Recognition of a Biological Attack
1 Arnon S.S., Schechter R., Ingelsby T.V., et al. Botulinum toxin as a biological weapon. JAMA. 2001;285:1059–1070.
2 Dennis D.T., et al. Tularemia as a biological weapon. In: Henderson D.A., Inglesby T.V., O’Toole T. Bioterrorism: Guidelines for Medical and Public Health Management. Chicago: American Medical Association Press; 2002:611–626.
3 Franz D.R., Jahrling P.B., Friedlander A.M., et al. Clinical recognition and management of patients exposed to biological warfare agents. JAMA. 1997;278:399–411.
4 Henderson D.A., Inglesby T.V., Bartlett J.G., et al. Smallpox as a biological weapon: medical and public health management. JAMA. 1999;281:2127–2137.
5 Inglesby T.V., Dennis D.T., Henderson D.A., et al. Plague as a biological weapon: medical and public health management. JAMA. 2000;283:2281–2290.
6 Inglesby T.V., O’Toole T., Henderson D.A., et al. Anthrax as a biological weapon, 2002: updated recommendations for management. JAMA. 2002;287:2236–2252.
7 Jernigan D.B., Ragunathan P.L., Bell B.P., et al. Investigation of bioterrorism-related anthrax, United States, 2001: epidemiologic findings. Emerg Infect Dis. 2002;8:1019–1028.
8 Management of patients with suspected viral hemorrhagic fever—United States. MMWR Morb Mortal Wkly Rep. 1995;44:475–479.
9 Miller J.M. Agents of bioterrorism. Preparing for bioterrorism at the community level. Infect Dis Clin North Am. 2001;15:1127–1156.
10 Waterer G.W., Robertson H. Bioterrorism for the respiratory physician. Respirology. 2009;14:5–11.
