• Frequently associated with cholelithiasis, choledocholithiasis, choledochal cyst, cirrhosis
CLINICAL ISSUES
• Patients present with repeated episodes of abdominal pain, jaundice, and acute cholangitis
Symptoms can mimic biliary stones due to intermittent obstruction of bile ducts by fragments of tumor
• Most common in older (6th-7th decades) male patients
• High propensity for malignant transformation with up to 83% of patients having adenocarcinoma at diagnosis
• Treatment is surgical resection of tumor (usually partial hepatectomy) or liver transplantation in patients with diffuse involvement of ducts
(Left) ERCP of a patient with elevated liver function tests shows polypoid filling defects within the extrahepatic duct. Mild dysplasia was identified at resection. Biliary papillomatosis (like biliary IPMN) is considered a premalignant lesion and is often frankly invasive at diagnosis. (Courtesy M. Kanematsu, MD.)
(Right) MIP MRCP image in the same patient demonstrates the multiple nodules appearing as low-signal filling defects within the duct. (Courtesy M. Kanematsu, MD.)
(Left) MRCP of a patient with jaundice shows multiple small common and anterior segmental ductal polypoid lesions and mild intrahepatic ductal dilatation. Resection of this premalignant, multifocal disease is often impossible. (Courtesy S. Yeon Kim, MD.)
(Right) Coronal CT reconstruction of the same patient again shows filling defects within the common duct . Bile duct resection confirmed multiple papillary neoplasms associated with invasive carcinoma. (Courtesy S. Yeon Kim, MD.)






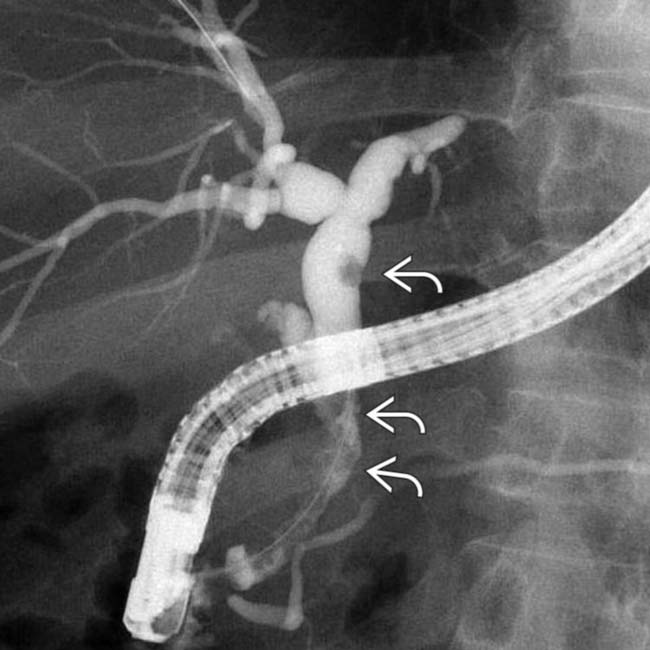
 within the extrahepatic duct. Mild dysplasia was identified at resection. Biliary papillomatosis (like biliary IPMN) is considered a premalignant lesion and is often frankly invasive at diagnosis. (Courtesy M. Kanematsu, MD.)
within the extrahepatic duct. Mild dysplasia was identified at resection. Biliary papillomatosis (like biliary IPMN) is considered a premalignant lesion and is often frankly invasive at diagnosis. (Courtesy M. Kanematsu, MD.)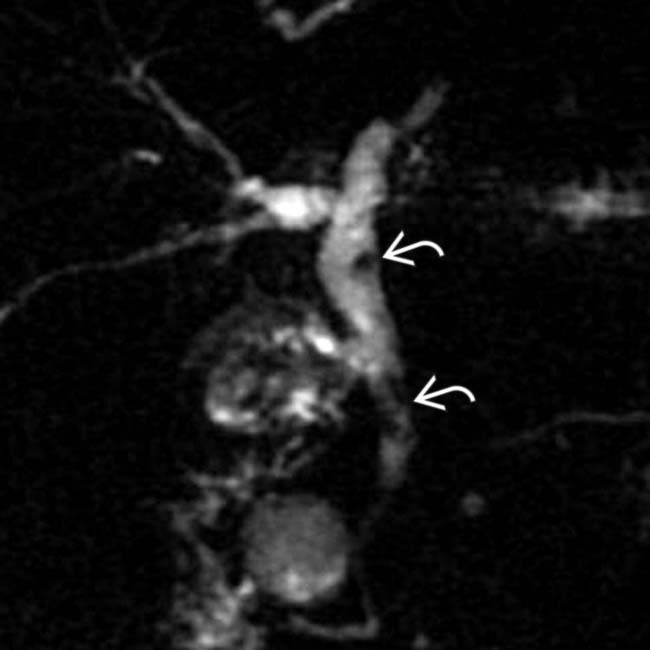
 within the duct. (Courtesy M. Kanematsu, MD.)
within the duct. (Courtesy M. Kanematsu, MD.)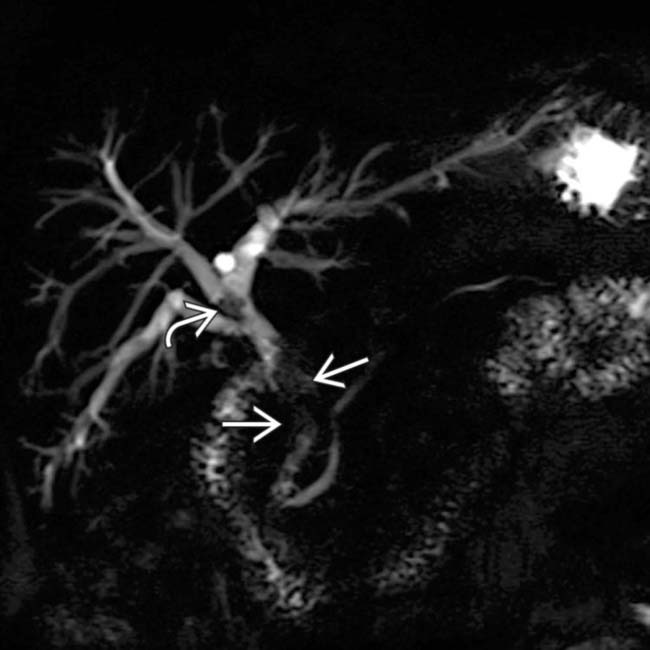
 and anterior segmental
and anterior segmental  ductal polypoid lesions and mild intrahepatic ductal dilatation. Resection of this premalignant, multifocal disease is often impossible.
ductal polypoid lesions and mild intrahepatic ductal dilatation. Resection of this premalignant, multifocal disease is often impossible. 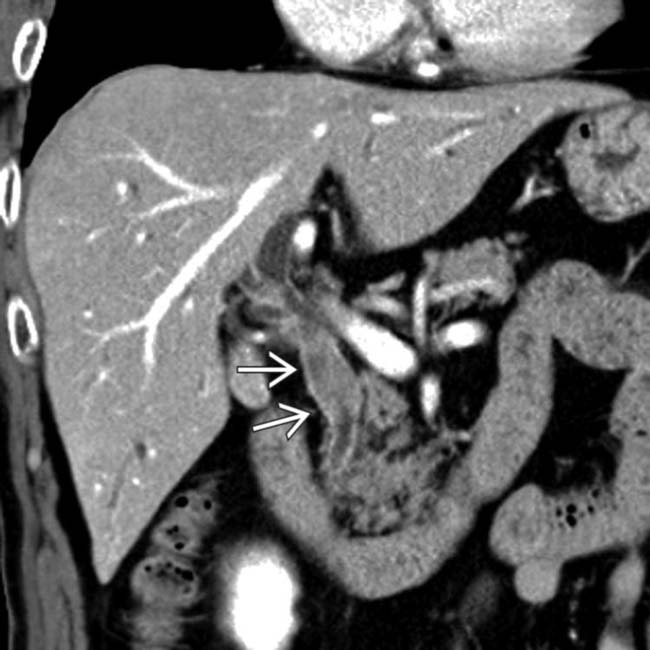
 . Bile duct resection confirmed multiple papillary neoplasms associated with invasive carcinoma.
. Bile duct resection confirmed multiple papillary neoplasms associated with invasive carcinoma. 

