– Melanoma classically described as hyperechoic, without acoustic shadowing
– May be single or multiple
– Flow characteristics variable on color Doppler, but usually evidence of internal flow
• Lymphoma of GB
High-grade lymphomas often present as bulky mass (usually hypodense and homogeneous), while low-grade lymphomas cause only mild wall thickening
Usually other evidence of lymphoma elsewhere, including adenopathy and splenomegaly
• Metastatic disease to biliary tree
Indistinguishable from cholangiocarcinoma, including bile duct wall thickening, discrete soft tissue mass in porta hepatis, and proximal biliary dilatation/obstruction
PATHOLOGY
• Metastases to GB are rare, representing < 5% of all GB malignancies
Melanoma accounts for 50-67% of GB metastases, with lung and renal malignancies also common
Most patients with GB metastases have end-stage disease with widespread metastatic disease
May rarely cause cholecystitis (due to cystic duct obstruction) or jaundice
• GB lymphoma represents only 0.1% of GB cancers
Almost always secondary lymphomatous involvement, with primary GB lymphoma extraordinarily rare
• Metastases to biliary tree are rare, with colon cancer most common (propensity for spread along epithelial surfaces)
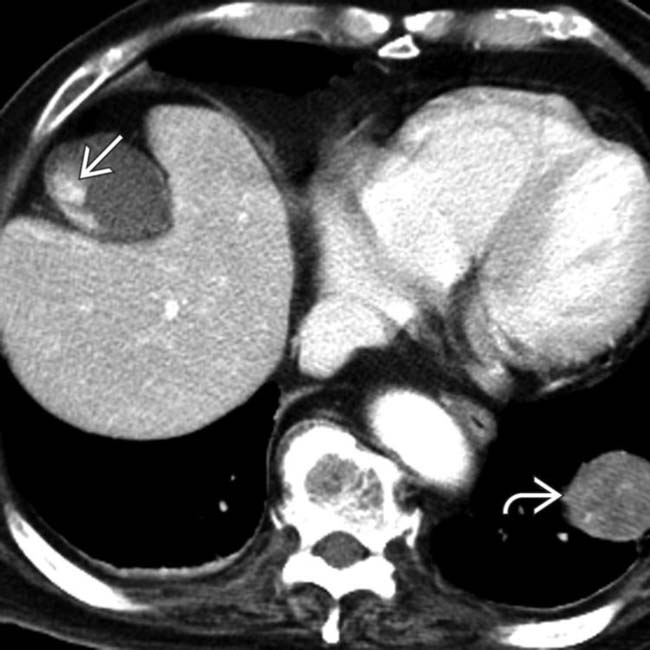
(Left) Axial CECT in a melanoma patient reveals a gallbladder metastasis , as well as a larger rounded left lower lobe pulmonary metastasis . Melanoma is the most common primary malignancy to metastasize to the gallbladder.
(Right) Color Doppler ultrasound demonstrates a hypoechoic rounded nodule in the gallbladder with internal color flow vascularity. While a large polyp or gallbladder cancer could also be considered, this was a melanoma metastasis.
(Left) Axial CECT in a patient with weight loss and jaundice shows a soft tissue mass within the gallbladder along with gallstones . Also noted is massive lymphadenopathy , all due to non-Hodgkin lymphoma.
(Right) Coronal CECT demonstrates a subtle soft tissue nodule arising in the common duct with thickening/hyperenhancement of the more proximal duct. While this could certainly represent a cholangiocarcinoma, this was a metastasis from colon cancer.
Transverse grayscale ultrasound of the porta hepatis in a 22-year-old woman presenting with RUQ pain 8 months after the resection of a lower leg melanoma reveals a large hypoechoic nodal metastasis as well as an additional porta hepatis mass invading the gallbladder wall .
Ultrasound demonstrates a rounded hypoechoic mass in the gallbladder, found to represent a melanoma metastasis.
Axial CECT in a patient with melanoma demonstrates a subtle enhancing nodule which had grown slowly over several exams. This was an isolated melanoma metastasis, without evidence of metastases elsewhere.
Axial CECT in a 54-year-old man with jaundice shows an enhancing mass causing obstruction of the bile ducts at the hepatic hilum. This lesion is indistinguishable by imaging from a Klatskin cholangiocarcinoma but proved to be a metastasis from a renal carcinoma.
Axial CECT in the same case shows the primary renal cell carcinoma that caused the hilar biliary obstruction due to metastasis.
Longitudinal color Doppler ultrasound in a 71-year-old woman with a recently diagnosed melanoma of the back demonstrates a polypoid intraluminal mass involving the posterior wall of the gallbladder and internal flow within the mass , findings consistent with a metastasis from melanoma.
Axial CECT in a 55-year-old man with a history of a scalp melanoma 2 years prior now presenting with weight loss and fatigue, demonstrates one of several enhancing masses in the wall of the gallbladder, proven to be metastases from melanoma.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] CT: Usually polyploid enhancing nodule or mass within GB lumen, but may appear as focal mural thickening
MR: Melanoma classically hyperintense on T1WI and hypointense on T2WI
– Melanoma classically described as hyperechoic, without acoustic shadowing
– May be single or multiple
– Flow characteristics variable on color Doppler, but usually evidence of internal flow
• Lymphoma of GB
High-grade lymphomas often present as bulky mass (usually hypodense and homogeneous), while low-grade lymphomas cause only mild wall thickening
Usually other evidence of lymphoma elsewhere, including adenopathy and splenomegaly
• Metastatic disease to biliary tree
Indistinguishable from cholangiocarcinoma, including bile duct wall thickening, discrete soft tissue mass in porta hepatis, and proximal biliary dilatation/obstruction
PATHOLOGY
• Metastases to GB are rare, representing < 5% of all GB malignancies
Melanoma accounts for 50-67% of GB metastases, with lung and renal malignancies also common
Most patients with GB metastases have end-stage disease with widespread metastatic disease
May rarely cause cholecystitis (due to cystic duct obstruction) or jaundice
•
Buy Membership for Radiology Category to continue reading. Learn more here









 , as well as a larger rounded left lower lobe pulmonary metastasis
, as well as a larger rounded left lower lobe pulmonary metastasis  . Melanoma is the most common primary malignancy to metastasize to the gallbladder.
. Melanoma is the most common primary malignancy to metastasize to the gallbladder.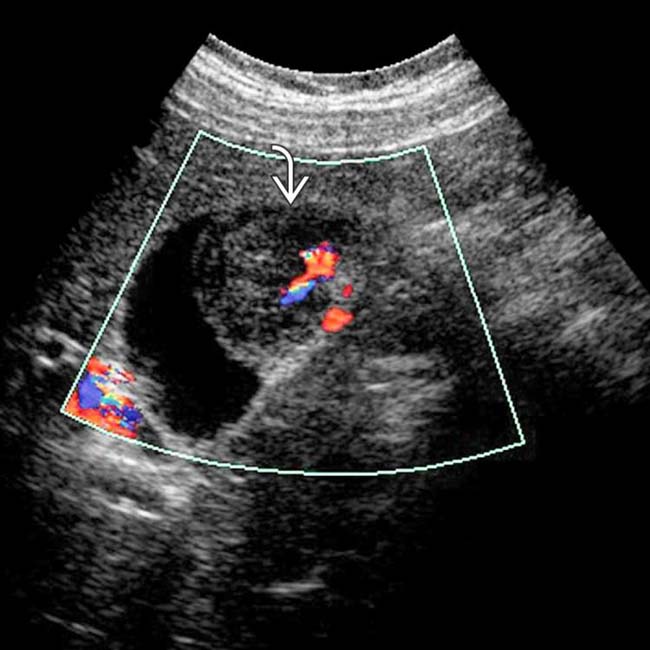
 in the gallbladder with internal color flow vascularity. While a large polyp or gallbladder cancer could also be considered, this was a melanoma metastasis.
in the gallbladder with internal color flow vascularity. While a large polyp or gallbladder cancer could also be considered, this was a melanoma metastasis.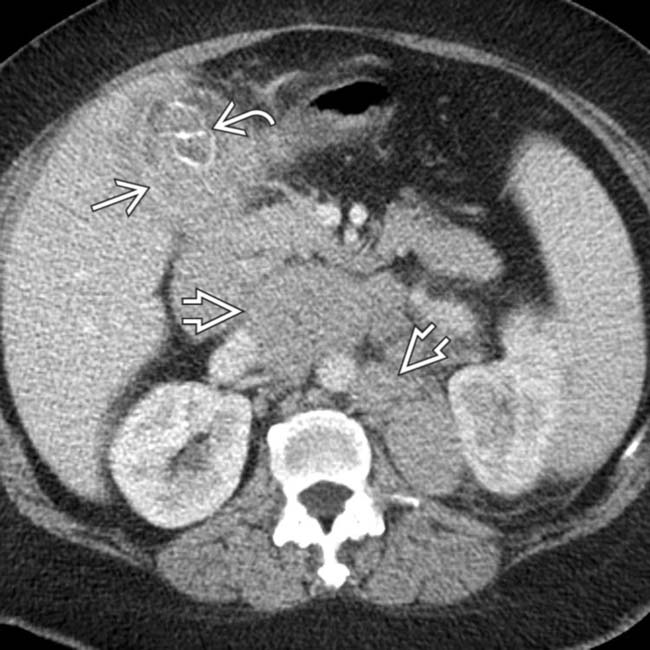
 within the gallbladder along with gallstones
within the gallbladder along with gallstones  . Also noted is massive lymphadenopathy
. Also noted is massive lymphadenopathy  , all due to non-Hodgkin lymphoma.
, all due to non-Hodgkin lymphoma.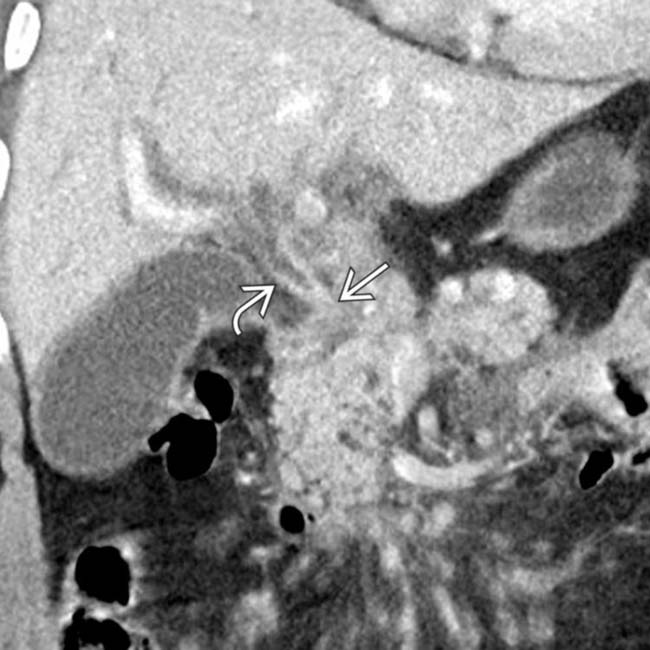
 arising in the common duct with thickening/hyperenhancement
arising in the common duct with thickening/hyperenhancement  of the more proximal duct. While this could certainly represent a cholangiocarcinoma, this was a metastasis from colon cancer.
of the more proximal duct. While this could certainly represent a cholangiocarcinoma, this was a metastasis from colon cancer.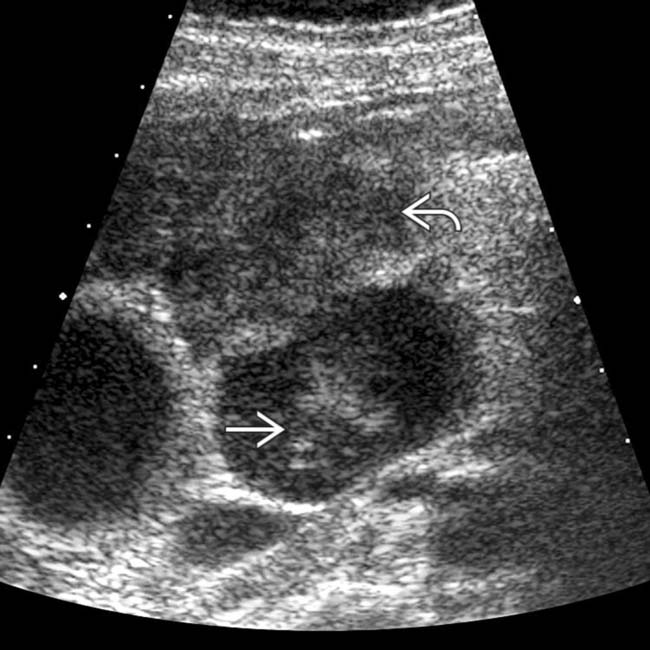
 as well as an additional porta hepatis mass invading the gallbladder wall
as well as an additional porta hepatis mass invading the gallbladder wall  .
.
 in the gallbladder, found to represent a melanoma metastasis.
in the gallbladder, found to represent a melanoma metastasis.
 which had grown slowly over several exams. This was an isolated melanoma metastasis, without evidence of metastases elsewhere.
which had grown slowly over several exams. This was an isolated melanoma metastasis, without evidence of metastases elsewhere.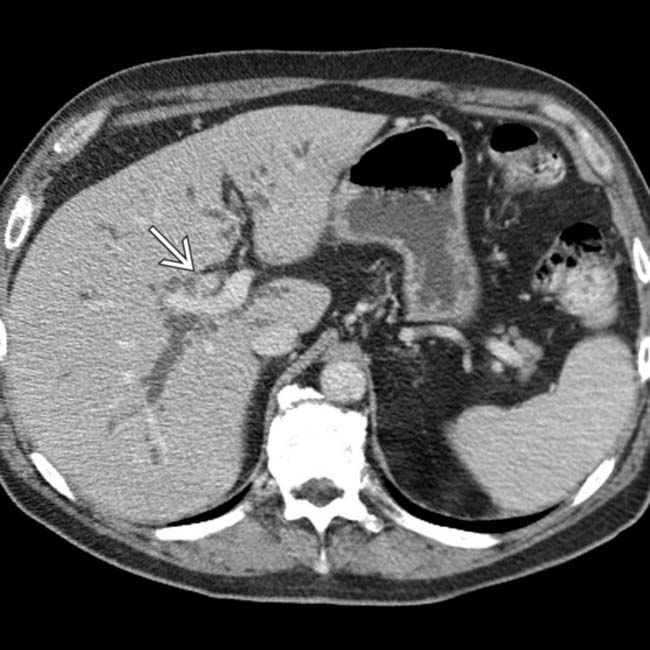
 causing obstruction of the bile ducts at the hepatic hilum. This lesion is indistinguishable by imaging from a Klatskin cholangiocarcinoma but proved to be a metastasis from a renal carcinoma.
causing obstruction of the bile ducts at the hepatic hilum. This lesion is indistinguishable by imaging from a Klatskin cholangiocarcinoma but proved to be a metastasis from a renal carcinoma.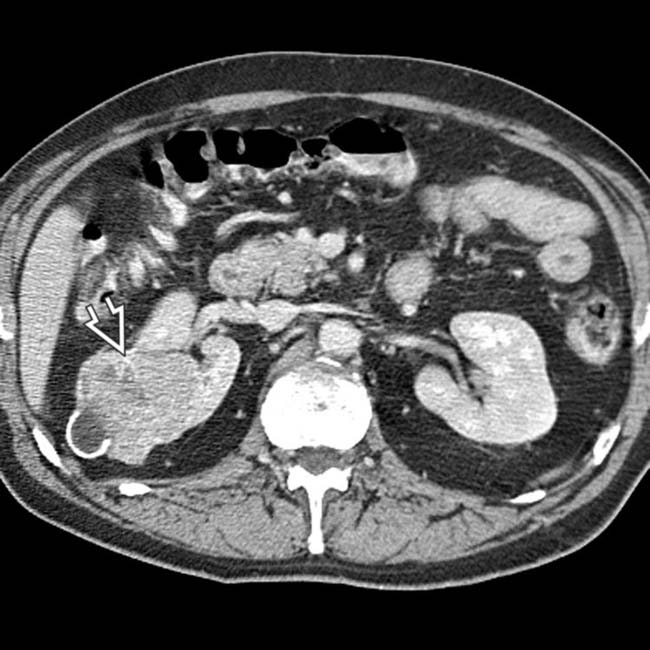
 that caused the hilar biliary obstruction due to metastasis.
that caused the hilar biliary obstruction due to metastasis.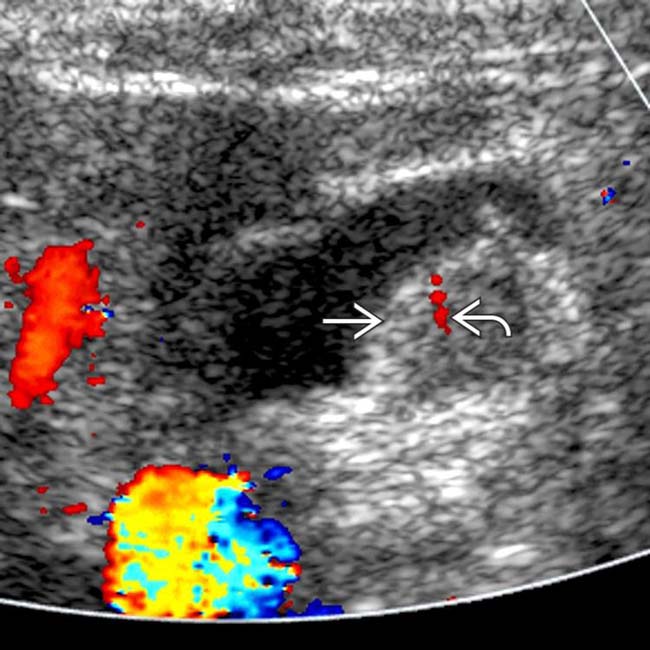
 involving the posterior wall of the gallbladder and internal flow within the mass
involving the posterior wall of the gallbladder and internal flow within the mass  , findings consistent with a metastasis from melanoma.
, findings consistent with a metastasis from melanoma.
 in the wall of the gallbladder, proven to be metastases from melanoma.
in the wall of the gallbladder, proven to be metastases from melanoma.