Chapter 16 Autoimmune Hemolytic Anemia
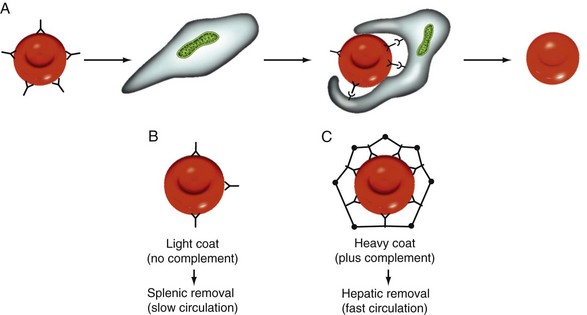
Figure 16-1 MECHANISM OF EXTRAVASCULAR HEMOLYSIS IN AUTOIMMUNE HEMOLYTIC ANEMIA.
(From Cunnigham MJ, Silberstein LE: Autoimmune Hemolytic Anemia. In Hoffman R, Benz EJ Jr, Shattil SJ, et al, eds: Hematology: Basic principles and practice, ed 4, 2005, Philadelphia, Elsevier.)
Table 16-1 Properties and Specificities of Red Blood Cell Autoantibodies

CAIHA, Cold autoimmune hemolytic anemia; Ig, immunoglobulin; WAIHA, warm autoimmune hemolytic anemia.
Four Important Questions for the Diagnosis and Management of Autoimmune Hemolytic Anemia
Question 1: Hemolytic anemia? The basic features of hemolytic anemia are reticulocytosis, low haptoglobin levels, elevated indirect bilirubin, and elevated LDH.
Question 2: Autoimmune hemolytic anemia? A direct DAT is initially performed with a polyspecific antibody to detect IgG or complement C3d bound to RBCs. If the DAT result is positive, the diagnosis of AIHA is established.
Question 3: Warm or Cold Autoimmune Hemolytic Anemia? The DAT is further elaborated with monospecific antibodies to IgG and complement (C3d). If the DAT result is positive with IgG alone or with IgG + C3d, the AIHA is most probably caused by a warm antibody (WAIHA). If the DAT is positive with C3d only, the AIHA is most probably caused by a cold antibody (CAIHA).
Question 4: Primary or secondary AIHA? More than half of AIHAs are secondary to underlying diseases. Secondary AIHA should be suspected in patients with additional findings or who are refractory to initial steroid treatment. In this case, the underlying disease has to be diagnosed (e.g., by serologic tests, CT scan, or bone marrow biopsy).
Table 16-2 Secondary Autoimmune Hemolytic Anemia in Malignancies
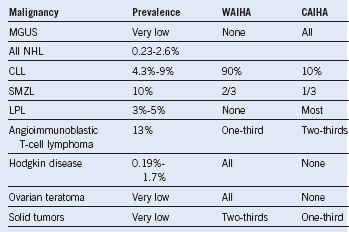
CLL, Chronic lymphocytic leukemia; LPL, lymphoplasmacytic lymphoma; MGUS, monoclonal gammopathy with unknown significance; NHL, non-Hodgkin lymphoma; SMZL, splenic marginal zone lymphoma.
Table 16-3 Autoimmune Hemolytic Anemia After Infections
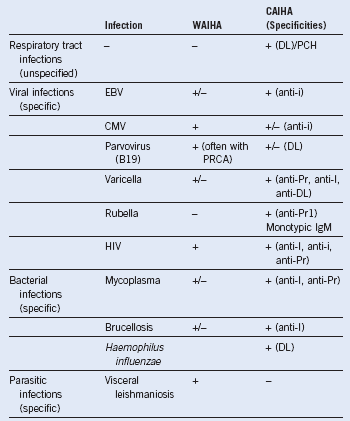
−, not reported; +, predominant type of autoimmune hemolytic anemia; +/−, single or few cases reported; CMV, cytomegalovirus; DL, Donath-Landsteiner antibody; EBV, Epstein-Barr virus; PCH, paroxysmal cold hemoglobinuria; PRCA, pure red blood cell aplasia.
Table 16-4 Drug-Induced Autoimmune Hemolytic Anemia
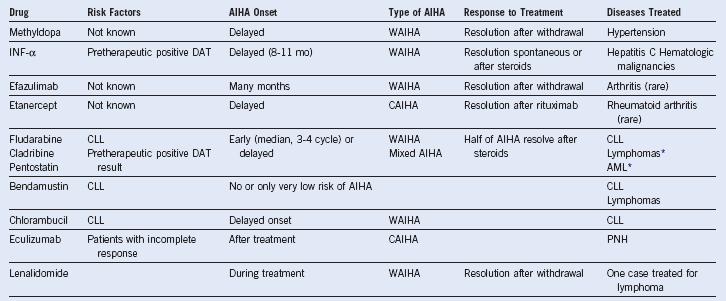
AML, Acute myeloid leukemia; CAIHA, cold autoimmune hemolytic anemia; CLL, chronic lymphocytic leukemia; INF, interferon; PNH, paroxysmal nocturnal hemoglobinuria; WAIHA, warm autoimmune hemolytic anemia.
Transfusion Therapy in Selected Patients With Severe Autoimmune Hemolytic Anemia
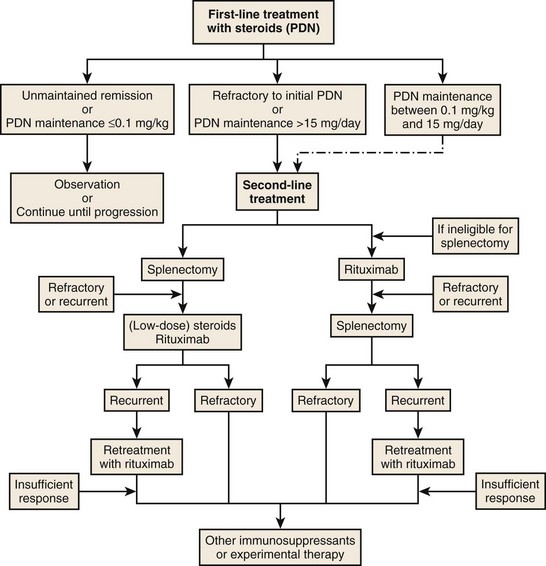
Figure 16-2 PROPOSED ALGORITHM FOR THERAPY OF WARM AUTOIMMUNE HEMOLYTIC ANEMIA.
(Modified from Lechner K, Jäger U: How I treat autoimmune haemolytic anemias in adults. Blood 116:1831, 2010.)
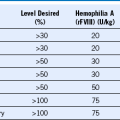
Table 16-5 Treatment Options for Primary and Secondary Warm Autoimmune Hemolytic Anemia and Cold Autoimmune Hemolytic Anemia
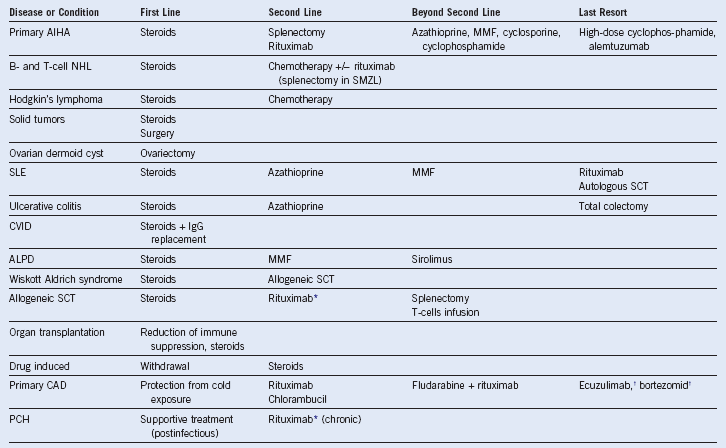
AIHA, Autoimmune hemolytic anemia; ALPD, autoimmune lymphoproliferative disorders; CAD, cold agglutinin disease; CVID, common variable immune deficiency; IgG, immunoglobulin G; MMF, mycophenolate mofetil; NHL, non-Hodgkin lymphoma; PCH, paroxysmal cold hemoglobinuria; SCT, stem cell transplantation; SLE, systemic lupus erythematosus; SMZL, splenic marginal zone lymphoma.
* Early second-line treatment because of known poor response to steroids.
Table 16-6 Second-Line Treatment Options After Steroids
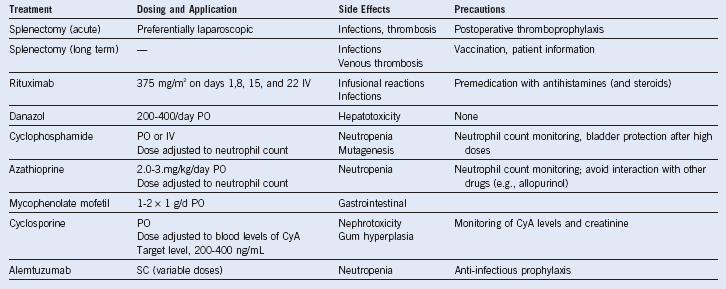
CyA, Cyclosporine A; IV, intravenous; PO, oral; SC, subcutaneous.