Chapter 6 AUTISM
General Discussion
Common behaviors in autistic disorder include stereotypic behaviors such as rocking or nonproductive movements of the hands and fingers as well as self-injurious behaviors and self-stimulation. Seizure disorders and mental retardation are also seen frequently in autistic disorder. Table 6-1 below lists the Diagnostic and Statistical Manual (DSM)-IV Diagnostic Criteria for Autistic Disorder.
Key Historical Features
Family history, especially of limited cognitive abilities or the presence of dysmorphic features
Suggested Work-up
Figure 6-1 provides an algorithm for evaluating patients suspected of having autism. The work-up begins with recognition and screening done at well-child visits. Indications for formal developmental evaluation include the following:
• No babbling, pointing, or other gestures by age 12 months
• No single words by age 16 months
• No two-word spontaneous phrases by age 24 months
• Loss of previously learned language or social skills at any age
• Any parental concern about delayed speech and language development, typically noticed at about age 18 months
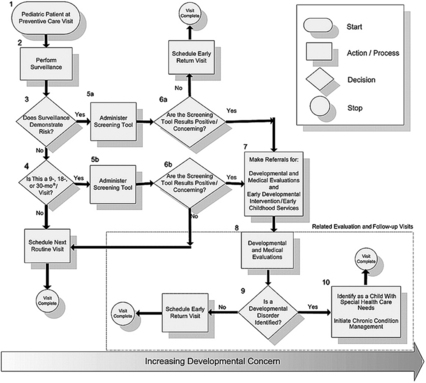
1. Pediatric Patient at Preventive Care Visit. Developmental concerns should be included as one of several health topics addressed at each pediatric preventive care visit throughout the first 5 years of life.
2. Perform Surveillance. Developmental surveillance is a flexible, longitudinal, continuous, and cumulative process whereby knowledgeable health care professionals identify children who may have developmental problems. Developmental surveillance has five components: (a) eliciting and attending to the parents’ concerns about their child’s development, (b) documenting and maintaining a developmental history, (c) making accurate observations of the child, (d) identifying the risk and protective factors, and (e) maintaining an accurate record and documenting the process and findings.
3. Does Surveillance Demonstrate Risk? The concerns of both parents and child health professionals should be included in determining whether surveillance suggests the child may be at risk of developmental delay. If either parents or the child health professional express concern about the child’s development, a developmental screening to specifically address the concern should be conducted.
4. Is This a 9-, 18-, or 30-Month Visit? All children should receive developmental screening using a standardized test. In the absence of established risk factors or parental or provider concerns, a general developmental screen is recommended at the 9-, 18, and 30-month visits. Additionally, autism-specific screening is recommended for all children at the 18-month visit.
5a and 5b. Administer Screening Tool. Developmental screening is the administration of a brief standardized tool that aids in the identification of children at risk of a developmental disorder. Developmental screening that targets the area of concern is indicated whenever a problem is identified during developmental surveillance.
6a and 6b. Are the Screening Tool Results Positive or Cause of Concern? When the results of the periodic screening tool are normal, the child health professional can inform the parents and continue with other aspects of the preventive visit. When a screening tool is administered as a result of concerns about development, an early return visit to provide additional developmental surveillance should be scheduled even if the screening tool results do not indicate a risk of delay.
7-8. Make Referrals for Developmental and Medical Evaluations and Early Developmental Intervention/Early Childhood Services (7). Developmental and Medical Evaluations. (8). If screening results warrant concern, the child should be scheduled for developmental and medical evaluations. Developmental evaluation is aimed at identifying the specific developmental disorder or disorders affecting the child. In addition to the developmental evaluation, a medical diagnostic evaluation to identify any underlying causes should be undertaken. Early developmental intervention/early childhood services can be particularly valuable when a child is first identified to be at high risk of delayed development because these programs often provide evaluation services and can offer other services to the child and family even before an evaluation is complete. Establishing an effective and efficient partnership with early childhood professionals is an important component of successful care coordination for children.
9. Is a Developmental Disorder Identified? If a developmental disorder is identified, the child should be identified as a child with special health care needs, and chronic condition management should be initiated (see no. 10 to follow). If a developmental disorder is not identified through medical and developmental evaluation, the child should be scheduled for an early return visit for further surveillance. More frequent visits, with particular attention paid to areas of concern, will allow the child to be promptly referred for further evaluation if any further evidence of delayed development or a specific disorder emerges.
10. Identification of a Child With Special Health Care Needs. Initial Chronic Condition Management. When a child is discovered to have a significant developmental disorder, that child becomes one with special health care needs, even if that child does not have a specific disease etiology identified. Such a child should be identified by the medical home for appropriate chronic condition management and regular monitoring and entered into the practice’s registry of children and youth with special health care needs.
(From Council on Children with Disabilities, Section on Developmental Behavioral Pediatrics, Bright Futures Steering Committee and Medical Home Initiatives for Children with Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics 2006;118:405–420, with permission.)
A number of resources are available for screening, such as the following:
Additional Work-up
| Genetic testing | If indicated by family history |
| Wood’s lamp examination of skin to identify depigmented macules | If tuberous sclerosis is suspected |
| Lead level | If lead poisoning is suspected |
| Metabolic screening | If an inborn error of metabolism is suspected |
| Electroencephalography | If seizure disorder is suspected |
| Central nervous system (CNS) imaging | If malignancy, hemorrhage, infection, or inflammation is suspected |
| Formal hearing evaluation | If there is any suspicion of hearing deficit because deafness and profound hearing loss can mimic autism |
| Vision screening | If any visual disturbance is suspected |
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV, 4th ed. Washington, DC: American Psychiatric Association; 1994.
2. Council on Children with Disabilities, Section on Developmental Behavioral Pediatrics, Bright Futures Steering Committee and Medical Home Initiatives for Children with Special Needs Project Advisory Committee. Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics 2006; 118:405–420.
3. Juul-Dam N., Townsend J., Courchesne E. Prenatal, perinatal, and neonatal factors in autism, pervasive developmental disorder-not otherwise specified, and the general population. Pediatrics. 2001;107:1–6.
4. Prater C.D., Zylstra R.G. Autism: a medical primer. Am Fam Physician. 2002;66:1667–1674.