CHAPTER 314 Atlantoaxial Rotatory Subluxation, Transverse Ligament Injury
The atlantoaxial joint is one of the most active joints in the body, and increased mobility of this joint causes some interesting problems with stability. Atlantoaxial rotatory subluxation (AARS) refers to a number of pathologic processes in which increased rotational instability of the C1-2 joint causes disarticulation of the facets and translational subluxation. AARS is relatively rare in adults but somewhat more common in children, albeit by a largely different mechanism of action. In pediatrics, the term atlantoaxial fixation refers to subluxation in which the facets become locked, thus making the deformity largely irreducible.1,2 In adults, the condition is almost exclusively due to trauma, whereas in children it may be the result of inflammatory diseases or congenital laxity of the transverse ligament. The lethality of atlantoaxial injuries is often discussed, but the true incidence is unknown. It is possible that the relative paucity of literature regarding atlantoaxial subluxation in adult trauma reflects this lethality. The close proximity of the medulla and vertebral arteries makes potentially fatal injuries seem relatively likely. The presence and duration of neurological symptoms vary greatly. Treatment of AARS is largely dependent on the age of the patient, etiology of the instability, radiographic classification, and the presence or absence of neurological symptoms.
Anatomy and Biomechanics of The Atlantoaxial Joint
The atlantoaxial joint is one of the most mobile joints in the human body and is estimated to move an average of 600 times per hour.3 Unfortunately, with the gain of a greater range and frequency of motion, a joint must sacrifice some inherent stability, and this predisposes the atlantoaxial joint to injury. The normal rotational motion of the cervical spine is approximately 90 degrees to either side, and nearly 60% of this rotation occurs at the atlantoaxial joint.4,5 The facet joints at C1-2 are almost horizontal, which allows excellent axial rotation with the sacrifice of bony translational stability. The joint is largely stabilized by two sets of ligamentous structures, the transverse ligament and the alar ligaments. The transverse ligament is a rather large web-like structure that courses immediately posterior to the dens. When intact, this prevents excessive translation of the atlas on the axis. The paired alar ligaments run from the lateral surface of the tip of the odontoid process to the occipital condyles and serve to limit rotation of the atlas on the axis. The alar ligaments act as secondary translational stabilizers in addition to the transverse ligament. When the transverse ligament is cut in cadaver studies, anterior translation of around 4 mm occurs.6 When the alar ligaments are additionally damaged, further translation of the atlas on the axis also occurs and rotatory stability is lost. The widest portion of the spinal canal in the cervical spine occurs at C1-2, but this part of the canal narrows as the head is turned to the side. The facets can be dislocated at roughly 63 degrees of rotation, and spinal cord compression occurs with this degree of rotation as well.7 It is important to keep in mind that the vertebral arteries run in the transverse foramina and, as the head is turned, the ipsilateral vertebral artery becomes kinked whereas the contralateral artery is stretched.8 Therefore, vertebral artery injury or insufficiency may be associated with AARS.
Diagnosis and Classification
The clinical manifestation of AARS includes what has been termed the “cock-robin” position of the neck. The patient is seen with the head tilted to one side and rotated to the contralateral side with slight flexion of the neck.6,9,10 The patient cannot usually correct the deformity beyond the neutral position, and attempts to reduce the deformity by the examiner cause cervical pain. Occipital pain may occur as a result of compression of the greater occipital nerve or the C2 nerve root. Posterior fossa symptoms (vertigo, nausea, tinnitus, visual disturbance) may result from stretching or kinking of the vertebral arteries.11 Neurological compromise is relatively rare in children unless associated with trauma but is more common in adults.9,10,12 The presence of neurological signs and symptoms in adults is thought to be more common; however, there is a paucity of literature on the subject. Of seven case reports on traumatic adult AARS,13–19 two patients had partial neurological deficits.17,19 Differentiation of atlantoaxial subluxation from benign torticollis is based on the side of sternocleidomastoid spasm. In torticollis, it occurs on the contralateral side of the head rotation because contraction of the muscle leads to the neck deformity. In rotatory subluxation, the muscle contracts in an attempt to reduce the deformity.20,21
Radiographic diagnosis can be difficult but has been made much easier with the advent of newer imaging modalities. Plain radiographs are very difficult to obtain in these patients and can be complex to interpret. An open-mouth, “odontoid” view shows asymmetric lateral masses with respect to the midline.6,10,12,20,22 A lateral mass that has rotated forward appears widened and shifted toward the midline. A lateral radiograph may show one lateral mass of the atlas projecting anterior to the odontoid process and giving a “wink” sign.22,23 In adults fracture may be seen, and the fragments of bone may further confuse the issue. Dynamic films have been suggested as a better tool to determine whether the deformity is fixed,6,12,20,22 but one must be careful in this case to be sure there are no fractures or gross instability.
Computed tomography (CT) is essential in diagnosing these injuries. Cervical spine CT is almost always included in modern trauma evaluation. Axial CT scans can reveal the rotated position of the atlas on the axis, and the classification of AARS (see later) is based on the amount of forward or backward displacement seen on CT. Fractures not easily visualized on plain radiographs also become apparent on CT scans. The occiput-C1 joint should also be examined to be sure that concomitant atlanto-occipital rotatory fixation is not present.24 CT scans can be reformatted in the coronal and sagittal planes and also now in three-dimensional space, which can be very useful in making the diagnosis. The use of contrast material can help determine the position and degree of torsion of the vertebral arteries and will be useful when transarticular screws are considered. Magnetic resonance imaging is the only study that can actually image the transverse ligament.10 It can also reveal the degree of cord compromise, if any. It is not as useful as CT in imaging the bony structure of the cervical spine.
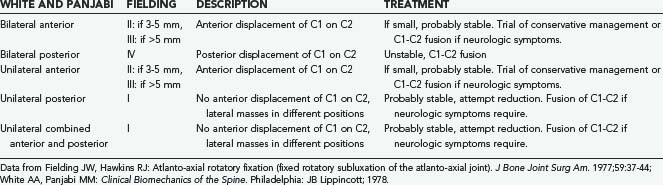
Two classification systems have been proposed for rotatory subluxation, and both are based on the direction and degree of subluxation on imaging. The Fielding system,9 proposed in 1977, divides the entity into four separate classes. In type 1, the odontoid is intact and continues to act as the pivot point for the atlas. In this class, the transverse ligament is often intact with disruption of the alar ligaments bilaterally. Types 2 and 3 encompass injuries with anterior translation of the atlas on the axis, and one lateral mass may act as the pivot point. The transverse ligament is usually disrupted or unusually lax in these cases. In type 4, there is posterior displacement of the atlas and the odontoid is compromised. In 1989, Levine and Edwards proposed the addition of type 5 to the Fielding classification, which consists of bilateral rotatory facet dislocation.25 These injuries occur almost exclusively in trauma; the transverse ligament is generally intact but the facet capsules are disrupted bilaterally. The White and Panjabi system classifies the entity into five classes based on the direction and laterality of the dislocation26 (Table 314-1 and Fig. 314-1).

Grisel’s Syndrome
Nontraumatic atlantoaxial subluxation, or Grisel’s syndrome, is a rare but dangerous complication after infectious processes or head and neck procedures. The underlying mechanism is unknown but is thought to be related to hematogenous spread of infection to the cervical spine with resulting edema and relaxation of the ligamentous structures.27 The most common cause is infection, which accounted for 48% of all cases according to one meta-analysis, followed by postsurgical cases, which accounted for 31%.28 These children often have clinical findings similar to those with painful torticollis. A high index of suspicion should be maintained in any child with a recent infection or procedure, and there should be a low threshold for imaging. A study by Rinaldo and colleagues concluded that permanent neurological sequelae may develop in 15% of patients with nontraumatic atlantoaxial subluxation.29 Children with disorders that already predispose them to ligamentous laxity, such as Down’s and Klippel-Feil syndromes, seem to be at increased risk for the development of Grisel’s syndrome. Broad-spectrum antibiotics can be a preventive measure in these high-risk groups. The majority of patients do quite well with conservative management, including reduction via cervical traction and muscle relaxants, but a small subset with higher grade subluxation may require surgical fusion.
Management
In adults with traumatic subluxation, one must use traction with extreme caution. Bony fractures should be ruled out by CT before the application of traction. Generally, traction is best applied with Gardner-Wells tongs or a halo ring, which give more control than a halter. Frequently, conscious sedation is necessary to provide adequate muscle relaxation. Levine and Edwards advocated a specific technique in which the oropharynx is anesthetized and the C1-2 step-off can be palpated and gently reduced during traction.25 Patients with minor ligamentous injuries are then placed in a halo vest for 3 months to allow fibrous healing and repair of the ligaments.30 Many patients recover quite well with this method of treatment, and motion at C1-2 may be preserved.
If the choice is made to proceed directly to fusion because of gross instability or if nonsurgical methods have failed, several different methods of stabilization have been described. Generally, if the deformity is reducible, posterior fixation plus fusion is all that is required. In the event that the deformity does not reduce, anterior decompression or release may be required, followed by posterior fusion. The anterior decompression may be accomplished via a transoral route or an anterolateral approach. A transoral route may allow exposure of the anterior atlas and axis by incising the posterior pharynx.31 The entire procedure is performed with the patient in cervical traction. Once the soft tissues and longus colli muscles have been stripped from the bone, the atlas will often reduce. If not, the anterior arch of C1 can be resected and the remaining transverse and alar ligaments stripped. This will almost surely allow reduction of the atlas into its normal position. At this point, reduction can be confirmed by lateral radiographs and the patient can be turned, with traction maintained, to perform a posterior fusion.
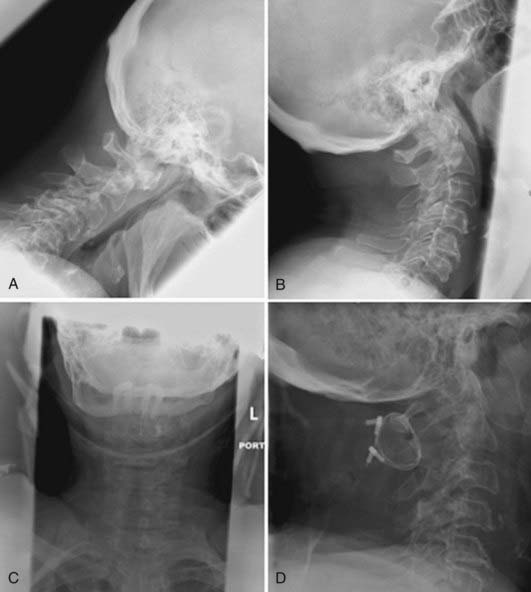
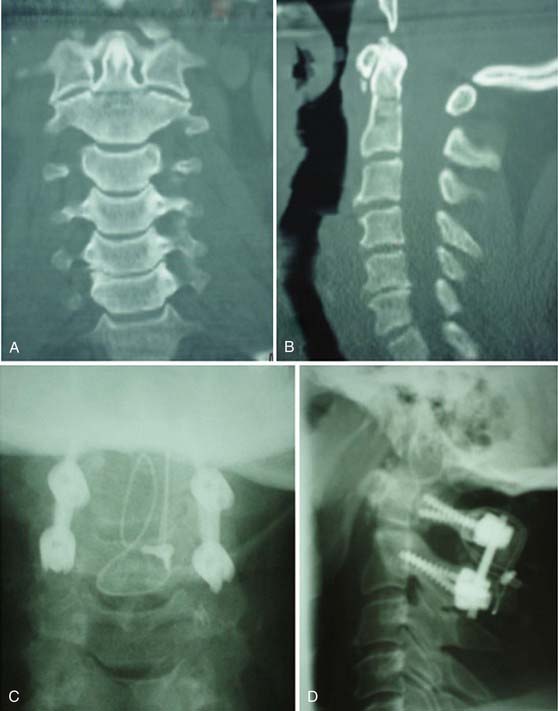
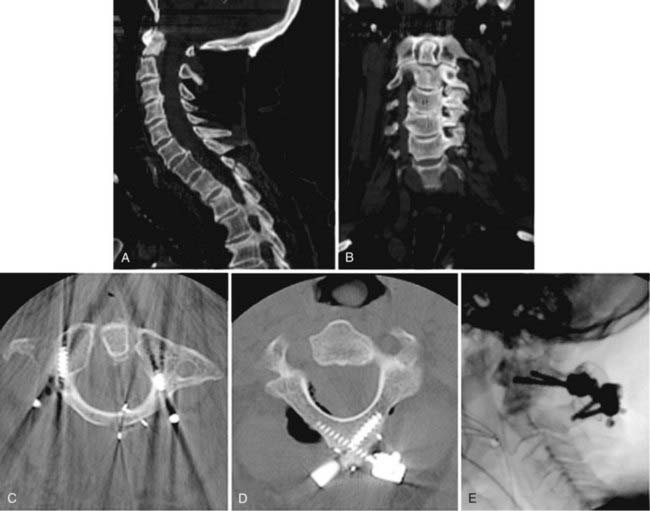
Many methods of posterior C1-2 fusion have been described and have been relatively successful. The Gallie,32 Brooks-Jenkins,33 and Sonntag-Dickman1 approaches have been most widely used. All these methods involve some form of autologous bone graft between C1 and C2, which is compressed by a combination of sublaminar hooks, wires, or cables (Fig. 314-2). These methods all have fairly good fusion rates that may exceed 90% when combined with halo immobilization.34 In the absence of halo immobilization, screw fixation techniques combined with posterior grafting have demonstrated similar fusion rates. The atlantoaxial transarticular screw fixation technique (Fig. 314-3) was first described by Magerl and Seemann35 in 1979 and has proved reliable for stabilizing the atlantoaxial joint along with a posterior graft without the need for a halo. A cadaveric study by Grob and associates showed the Magerl technique of true three-point fixation (two screws, wire or cable fixation of the graft) to be biomechanically superior to the other posterior C1-2 fusion techniques.2 This technique has gained great popularity in atlantoaxial fusion in recent years but may be contraindicated because of anomalous anatomy of the vertebral arteries in as many as 20% of patients.36–39 Harms and Melcher pioneered a technique of C1-2 fusion that incorporates lateral mass screws in C1 and pedicle screws in C2 connected by a posterior rod system and has a lower incidence of vertebral artery injury (Fig. 314-4). This method of fusion has been shown to provide stability similar to transarticular screws40,41 and has also been demonstrated to be clinically effective in a large series.42 Recently, Wright described a translaminar fixation technique for C2, a technique that lowers the risk for vertebral artery injury even further (Fig. 314-5).43 Selection of the specific method of internal stabilization used should be based on the surgeon’s comfort with the various techniques and the specific bony anatomy of each individual patient.

Aryan HE, Newman CB, Nottmeier EW, et al. Stabilization of the atlantoaxial complex via C-1 lateral mass and C-2 pedicle screw fixation in a multicenter clinical experience in 102 patients: modification of the Harms and Goel techniques. J Neurosurg Spine. 2008;8:222-229.
Born CT, Mure AJ, Iannacone WM, et al. Three-dimensional computerized tomographic demonstration of bilateral atlantoaxial rotatory dislocation in an adult: report of a case and review of the literature. J Orthop Trauma. 1994;8:67-72.
Brooks AL, Jenkins EB. Atlanto-axial arthrodesis by the wedge compression method. J Bone Joint Surg Am. 1978;60:279-284.
Dickman CA, Sonntag VK, Papadopoulos SM, et al. The interspinous method of posterior atlantoaxial arthrodesis. J Neurosurg. 1991;74:190-198.
Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation (fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977;59:37-44.
Fuentes S, Bouillot P, Palombi O, et al. Traumatic atlantoaxial rotatory dislocation with odontoid fracture: case report and review. Spine. 2001;26:830-834.
Gallie W. Fractures and dislocations of the cervical spine. Am J Surg. 1939;46:495-499.
Grob D, Crisco JJ3rd, Panjabi MM, et al. Biomechanical evaluation of four different posterior atlantoaxial fixation techniques. Spine. 1992;17:480-490.
Jones RN. Rotatory dislocation of both atlanto-axial joints. J Bone Joint Surg Br. 1984;66:6-7.
Karkos PD, Benton J, Leong SC, et al. Grisel’s syndrome in otolaryngology: a systematic review. Int J Pediatr Otorhinolaryngol. 2007;71:1823-1827.
Levine AM, Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Relat Res. 1989;239:53-68.
Lucas JT, Hungerford GD, Perot PLJr. Treatment of nontraumatic atlantoaxial dislocation and fibrous fusion. Case report. J Neurosurg. 1982;56:139-142.
Magerl F, Seemann P. Stable posterior fusion of the atlas and axis by transarticular screw fixation. In: Kehr P, Weidner A, editors. Cervical Spine, Vol 1. Vienna: Springer-Verlag; 1987:322-327.
Maheshwaran S, Sgouros S, Jeyapalan K, et al. Imaging of childhood torticollis due to atlanto-axial rotatory fixation. Childs Nerv Syst. 1995;11:667-671.
Moore KR, Frank EH. Traumatic atlantoaxial rotatory subluxation and dislocation. Spine. 1995;20:1928-1930.
Robertson PA, Swan HA. Traumatic bilateral rotatory facet dislocation of the atlas on the axis. Spine. 1992;17:1252-1254.
Schmidek HH, Smith DA, Sofferman RA, et al. Transoral unilateral facetectomy in the management of unilateral anterior rotatory atlantoaxial fracture/dislocation: a case report. Neurosurgery. 1986;18:645-652.
White AA, Panjabi MM. Clinical Biomechanics of the Spine. Philadelphia: JB Lippincott; 1978.
Wise JJ, Cheney R, Fischgrund J. Traumatic bilateral rotatory dislocation of the atlanto-axial joints: a case report and review of the literature. J Spinal Disord. 1997;10:451-453.
Wortzman G, Dewar FP. Rotary fixation of the atlantoaxial joint: rotational atlantoaxial subluxation. Radiology. 1968;90:479-487.
Wright NM. Translaminar rigid screw fixation of the axis. Technical note. J Neurosurg Spine. 2005;3:409-414.
1 Dickman CA, Sonntag VK, Papadopoulos SM, et al. The interspinous method of posterior atlantoaxial arthrodesis. J Neurosurg. 1991;74:190-198.
2 Grob D, Crisco JJ3rd, Panjabi MM, et al. Biomechanical evaluation of four different posterior atlantoaxial fixation techniques. Spine. 1992;17:480-490.
3 Bland JH. Rheumatoid subluxation of the cervical spine. J Rheumatol. 1990;17:134-137.
4 Pang D, Li V. Atlantoaxial rotatory fixation: Part 1—Biomechanics of normal rotation at the atlantoaxial joint in children. Neurosurgery. 2004;55:614-625.
5 Phillips WA, Hensinger RN. The management of rotatory atlanto-axial subluxation in children. J Bone Joint Surg Am. 1989;71:664-668.
6 Wortzman G, Dewar FP. Rotary fixation of the atlantoaxial joint: rotational atlantoaxial subluxation. Radiology. 1968;90:479-487.
7 Mazzara JT, Fielding JW. Effect of C1-C2 rotation on canal size. Clin Orthop Relat Res. 1988;237:115-119.
8 White AA, Panjabi MM. Kinematics of the spine. In: White AA, Panjabi MM, editors. Clinical Biomechanics of the Spine. Philadelphia: JB Lippincott; 1978:87-125.
9 Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation (fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977;59:37-44.
10 Maheshwaran S, Sgouros S, Jeyapalan K, et al. Imaging of childhood torticollis due to atlanto-axial rotatory fixation. Childs Nerv Syst. 1995;11:667-671.
11 Shapiro I, Frankel V. Biomechanics of the cervical spine. In: Frankel V, Nordin M, editors. Basic Biomechanics of the Musculoskeletal System. Philadelphia: Lea & Febiger; 1989:209-224.
12 Kowalski HM, Cohen WA, Cooper P, et al. Pitfalls in the CT diagnosis of atlantoaxial rotary subluxation. AJR Am J Roentgenol. 1987;149:595-600.
13 Born CT, Mure AJ, Iannacone WM, et al. Three-dimensional computerized tomographic demonstration of bilateral atlantoaxial rotatory dislocation in an adult: report of a case and review of the literature. J Orthop Trauma. 1994;8:67-72.
14 Fuentes S, Bouillot P, Palombi O, et al. Traumatic atlantoaxial rotatory dislocation with odontoid fracture: case report and review. Spine. 2001;26:830-834.
15 Jones RN. Rotatory dislocation of both atlanto-axial joints. J Bone Joint Surg Br. 1984;66:6-7.
16 Moore KR, Frank EH. Traumatic atlantoaxial rotatory subluxation and dislocation. Spine. 1995;20:1928-1930.
17 Robertson PA, Swan HA. Traumatic bilateral rotatory facet dislocation of the atlas on the axis. Spine. 1992;17:1252-1254.
18 Schmidek HH, Smith DA, Sofferman RA, et al. Transoral unilateral facetectomy in the management of unilateral anterior rotatory atlantoaxial fracture/dislocation: a case report. Neurosurgery. 1986;18:645-652.
19 Wise JJ, Cheney R, Fischgrund J. Traumatic bilateral rotatory dislocation of the atlanto-axial joints: a case report and review of the literature. J Spinal Disord. 1997;10:451-453.
20 Johnson DP, Fergusson CM. Early diagnosis of atlanto-axial rotatory fixation. J Bone Joint Surg Br. 1986;68:698-701.
21 Roche CJ, O’Malley M, Dorgan JC, et al. A pictorial review of atlanto-axial rotatory fixation: key points for the radiologist. Clin Radiol. 2001;56:947-958.
22 Kawabe N, Hirotani H, Tanaka O. Pathomechanism of atlantoaxial rotatory fixation in children. J Pediatr Orthop. 1989;9:569-574.
23 Weinstein S. Atlantoaxial rotatory displacement. In: The Pediatric Spine. New York: Raven Press; 1994:408-420.
24 Fielding JW, Stillwell WT, Chynn KY, et al. Use of computed tomography for the diagnosis of atlanto-axial rotatory fixation. A case report. J Bone Joint Surg Am. 1978;60:1102-1104.
25 Levine AM, Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Relat Res. 1989;239:53-68.
26 White AA, Panjabi MM. Clinical Biomechanics of the Spine. Philadelphia: JB Lippincott; 1978.
27 Richter GT, Bower CM. Cervical complications following routine tonsillectomy and adenoidectomy. Curr Opin Otolaryngol Head Neck Surg. 2006;14:375-380.
28 Karkos PD, Benton J, Leong SC, et al. Grisel’s syndrome in otolaryngology: a systematic review. Int J Pediatr Otorhinolaryngol. 2007;71:1823-1827.
29 Rinaldo A, Mondin V, Suarez C, et al. Grisel’s syndrome in head and neck practice. Oral Oncol. 2005;41:966-970.
30 Lucas JT, Hungerford GD, Perot PLJr. Treatment of nontraumatic atlantoaxial dislocation and fibrous fusion. Case report. J Neurosurg. 1982;56:139-142.
31 Wang C, Yan M, Zhou HT, et al. Open reduction of irreducible atlantoaxial dislocation by transoral anterior atlantoaxial release and posterior internal fixation. Spine. 2006;31:E306-E313.
32 Gallie W. Fractures and dislocations of the cervical spine. Am J Surg. 1939;46:495-499.
33 Brooks AL, Jenkins EB. Atlanto-axial arthrodesis by the wedge compression method. J Bone Joint Surg Am. 1978;60:279-284.
34 Gluf WM, Schmidt MH, Apfelbaum RI. Atlantoaxial transarticular screw fixation: a review of surgical indications, fusion rate, complications, and lessons learned in 191 adult patients. J Neurosurg Spine. 2005;2:155-163.
35 Magerl F, Seemann P. Stable posterior fusion of the atlas and axis by transarticular screw fixation. In: Kehr P, Weidner A, editors. Cervical Spine, Vol 1. Vienna: Springer-Verlag; 1987:322-327.
36 Abou Madawi A, Solanki G, Casey AT, et al. Variation of the groove in the axis vertebra for the vertebral artery. Implications for instrumentation. J Bone Joint Surg Br. 1997;79:820-823.
37 Madawi AA, Casey AT, Solanki GA, et al. Radiological and anatomical evaluation of the atlantoaxial transarticular screw fixation technique. J Neurosurg. 1997;86:961-968.
38 Mandel IM, Kambach BJ, Petersilge CA, et al. Morphologic considerations of C2 isthmus dimensions for the placement of transarticular screws. Spine. 2000;25:1542-1547.
39 Wright NM, Lauryssen C. Vertebral artery injury in C1-2 transarticular screw fixation: results of a survey of the AANS/CNS section on disorders of the spine and peripheral nerves. American Association of Neurological Surgeons/Congress of Neurological Surgeons. J Neurosurg. 1998;88:634-640.
40 Melcher RP, Puttlitz CM, Kleinstueck FS, et al. Biomechanical testing of posterior atlantoaxial fixation techniques. Spine. 2002;27:2435-2440.
41 Paramore CG, Dickman CA, Sonntag VK. The anatomical suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg. 1996;85:221-224.
42 Aryan HE, Newman CB, Nottmeier EW, et al. Stabilization of the atlantoaxial complex via C-1 lateral mass and C-2 pedicle screw fixation in a multicenter clinical experience in 102 patients: modification of the Harms and Goel techniques. J Neurosurg Spine. 2008;8:222-229.
43 Wright NM. Translaminar rigid screw fixation of the axis. Technical note. J Neurosurg Spine. 2005;3:409-414.






