[level-membership-for-radiology-category] Triangular with sharp, linear margin between normal pancreas and area of fatty infiltration
• Lack of mass effect or dilatation of common bile duct or pancreatic duct
• Pancreas maintains normal external contour and normal pancreatic lobulations
• Chemical shift MR (in- and out-of-phase imaging) most specific modality for making a definitive diagnosis in confusing cases
Signal dropout in areas of fatty infiltration on opposed-phase images
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic head adenocarcinoma
• Focal pancreatitis
• Diffuse fatty replacement of pancreas
• Intrapancreatic lipoma
PATHOLOGY
• Dorsal pancreatic bud develops into body, tail, and anterior head of pancreas, while ventral bud develops into posterior head and uncinate process
• Fat accumulates preferentially within anterior head of pancreas derived from dorsal foregut bud
• May reflect more tightly packed pancreatic lobules in ventral bud compared to dorsal bud
CLINICAL ISSUES
• Incidental finding in asymptomatic patients
• No association with endocrine or exocrine abnormalities
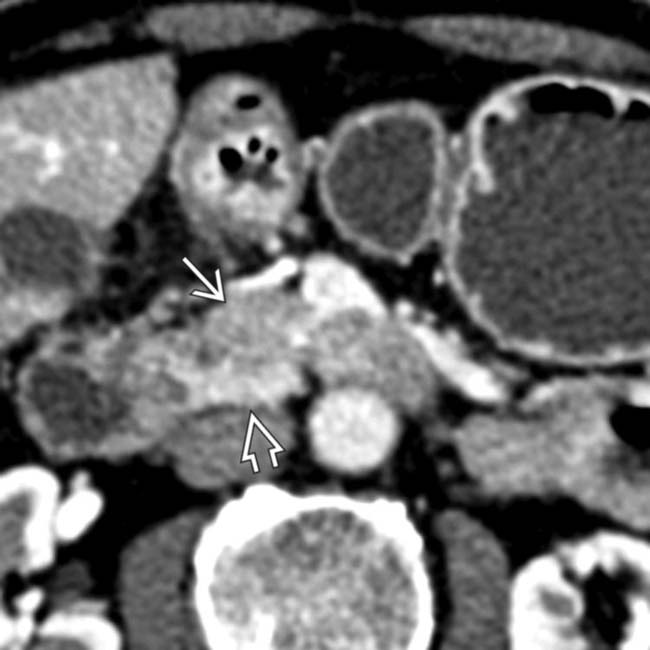
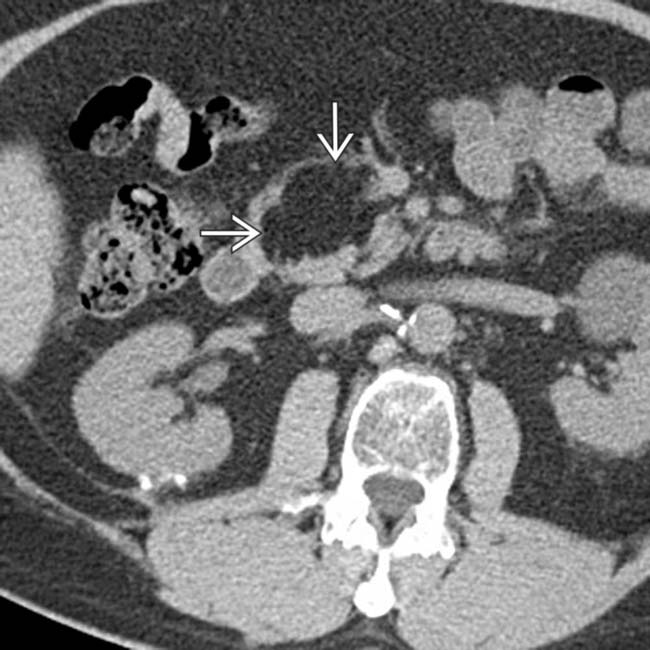
(Left) Axial arterial phase CECT demonstrates a low-attenuation area anteriorly within the head of the pancreas. Note the normally enhancing uncinate process posterior to this area, as well as the sharp linear boundary demarcating the low attenuation area.
(Right) A coronal curved planar reformation along the pancreatic duct demonstrates a normal duct. The characteristic location and the lack of mass effect on the duct are key findings to suggest the diagnosis of focal fatty infiltration.
(Left) Axial in-phase GRE MR image demonstrates uniform signal in the head of the pancreas . (Courtesy H. Harvin, MD.)
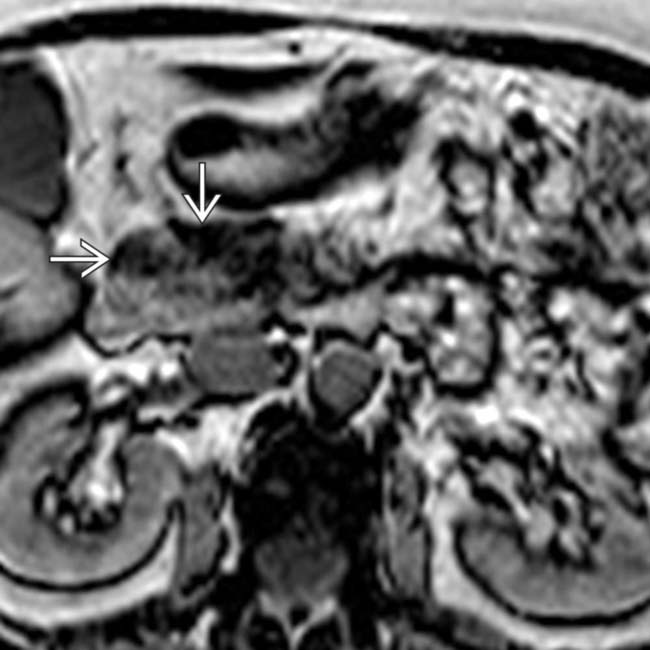
(Right) Axial opposed-phase MR in the same patient shows dropout of signal in the anterior aspect of the head, a classic finding confirming asymmetric fatty lobulation. Note the preserved higher signal and lack of dropout from the normal pancreatic tissue in the uncinate process . (Courtesy H. Harvin, MD.)
TERMINOLOGY
Abbreviations
•
Synonyms
• Focal lipomatosis or focal fatty infiltration of pancreas
Definitions
• Focal accumulation of fat within anterior aspect of head of pancreas, a normal variant that may simulate a hypodense mass on CT
IMAGING
General Features
• Best diagnostic clue
Ill-defined, low-attenuation area (without mass effect or ductal dilatation) in anterior head of pancreas
• Location
Anteriorly within head of pancreas (corresponds to dorsal bud in embryologic development)
Often spares region around intrapancreatic common bile duct (CBD)
• Size
Typically 2-3 cm
• Morphology
Often ill-defined area with geographic distribution
Triangular or plate-like shape
May have straight interface with normal-appearing uncinate process and posterior pancreatic head
CT Findings
• Low-attenuation area within anterior head of pancreas
Triangular with sharp, linear margin between normal pancreas and area of fatty infiltration
• No abnormal enhancement in fatty area
• No mass effect or dilatation of CBD or pancreatic duct (PD)
• Pancreas maintains normal external contour and normal pancreatic lobulations
• Unlike lipoma, not a discrete fatty mass (-20 to -80 HU)
MR Findings
• Chemical shift MR (in- and out-of-phase imaging) is most specific modality for making definitive diagnosis
• Signal dropout in areas of fatty infiltration on opposed-phase images
Ultrasonographic Findings
• Areas of fatty infiltration appear abnormally hyperechoic
• Can create impression of hypoechoic uncinate lesion due to echogenic fatty infiltration in adjacent anterior head
Imaging Recommendations
• Best imaging tool
MR with chemical shift imaging
• Protocol advice
DIFFERENTIAL DIAGNOSIS
Pancreatic Head Adenocarcinoma
• Hypodense lesion with mass effect obstructing PD or CBD
• Contour deformity of pancreas with loss of normal fatty lobulations
Focal Pancreatitis
• Low-attenuation area with peripancreatic inflammation
Diffuse Fatty Replacement of Pancreas
• Associated with cystic fibrosis, lipomatous pseudohypertrophy, and senescent fatty replacement
Intrapancreatic Lipoma
• Rare fat-containing mass with well-defined margins within pancreatic parenchyma
• Usually located in pancreatic head
PATHOLOGY
General Features
• Etiology
Dorsal pancreatic bud develops into body, tail, and anterior head of pancreas, while ventral bud develops into posterior head and uncinate process
Fat accumulates preferentially within anterior head of pancreas derived from dorsal foregut bud
May reflect more tightly packed pancreatic lobules in ventral bud compared to dorsal bud
Staging, Grading, & Classification
• Type I fatty infiltration involves only anterior head of pancreas with sparing of posterior head and uncinate (70%)
• Type II fatty infiltration involves entire head and uncinate process with sparing around common bile duct (30%)
• May be present in up to 3% of all patients
Gross Pathologic & Surgical Features
• Yellowish fat intermixed with normal pancreatic lobules
Microscopic Features
• Adipose cells intermixed with normal pancreatic ductal and islet cells
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
Incidental finding in asymptomatic patients
No association with endocrine or exocrine abnormality
• Other signs/symptoms
Natural History & Prognosis
• No clinical significance
DIAGNOSTIC CHECKLIST
Consider
• Pancreatic carcinoma if contour abnormality or obstruction of PD or CBD
• Pancreatic lipoma if discrete, well-defined area of fat attenuation with no enhancement
Image Interpretation Pearls
• Area of ill-defined hypoattenuation on CT characteristically located within anterior head of pancreas
• Shows signal loss on opposed-phase chemical shift MR
Axial NECT demonstrates a well-defined fat attenuation mass in the pancreatic head, representing a pancreatic lipoma. These lesions are rare, have a predisposition for the pancreatic head, and are much more well-defined and mass-like compared to focal fatty infiltration.
Axial CECT demonstrates a plate-like area of lower attenuation in the anterior aspect of the pancreatic head. Note that this area results in no abnormality of the pancreatic contour, nor is there evidence of pancreatic or biliary ductal obstruction. There is a sharp linear margin between the low- density anterior head and the normal- density posterior head. This is a classic appearance for focal fatty infiltration.
In-phase chemical shift MR from the same patient shows uniform signal throughout the pancreatic head.
Out-phase chemical shift MR from the same patient shows signal drop-out corresponding to the low density seen in the anterior pancreatic head on CT, confirming the diagnosis of benign focal fatty infiltration. Chemical shift MR is the most sensitive modality for this diagnosis.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Triangular with sharp, linear margin between normal pancreas and area of fatty infiltration
• Lack of mass effect or dilatation of common bile duct or pancreatic duct
• Pancreas maintains normal external contour and normal pancreatic lobulations
• Chemical shift MR (in- and out-of-phase imaging) most specific modality for making a definitive diagnosis in confusing cases
Signal dropout in areas of fatty infiltration on opposed-phase images
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic head adenocarcinoma
• Focal pancreatitis
• Diffuse fatty replacement of pancreas
• Intrapancreatic lipoma
PATHOLOGY
• Dorsal pancreatic bud develops into body, tail, and anterior head of pancreas, while ventral bud develops into posterior head and uncinate process
• Fat accumulates preferentially within anterior head of pancreas derived from dorsal foregut bud
• May reflect more tightly packed pancreatic lobules in ventral bud compared to dorsal bud
CLINICAL ISSUES
• Incidental finding in asymptomatic patients
• No association with endocrine or exocrine abnormalities
(Left) Axial arterial phase CECT demonstrates a low-attenuation area anteriorly within the head of the pancreas. Note the normally enhancing uncinate process posterior to this area, as well as the sharp linear boundary demarcating the low attenuation area.
(Right) A coronal curved planar reformation along the pancreatic duct demonstrates a normal duct. The characteristic location and the lack of mass effect on the duct are key findings to suggest the diagnosis of focal fatty infiltration.
(Left) Axial in-phase GRE MR image demonstrates uniform signal in the head of the pancreas . (Courtesy H. Harvin, MD.)
(Right) Axial opposed-phase MR in the same patient shows dropout of signal in the anterior aspect of the head, a classic finding confirming asymmetric fatty lobulation. Note the preserved higher signal and lack of dropout from the normal pancreatic tissue in the uncinate process . (Courtesy H. Harvin, MD.)
TERMINOLOGY
Abbreviations
•
Synonyms
• Focal lipomatosis or focal fatty infiltration of pancreas
Definitions
• Focal accumulation of fat within anterior aspect of head of pancreas, a normal variant that may simulate a hypodense mass on CT
IMAGING
General Features
• Best diagnostic clue
Ill-defined, low-attenuation area (without mass effect or ductal dilatation) in anterior head of pancreas
• Location
Buy Membership for Radiology Category to continue reading. Learn more here

 anteriorly within the head of the pancreas. Note the normally enhancing uncinate process
anteriorly within the head of the pancreas. Note the normally enhancing uncinate process  posterior to this area, as well as the sharp linear boundary demarcating the low attenuation area.
posterior to this area, as well as the sharp linear boundary demarcating the low attenuation area.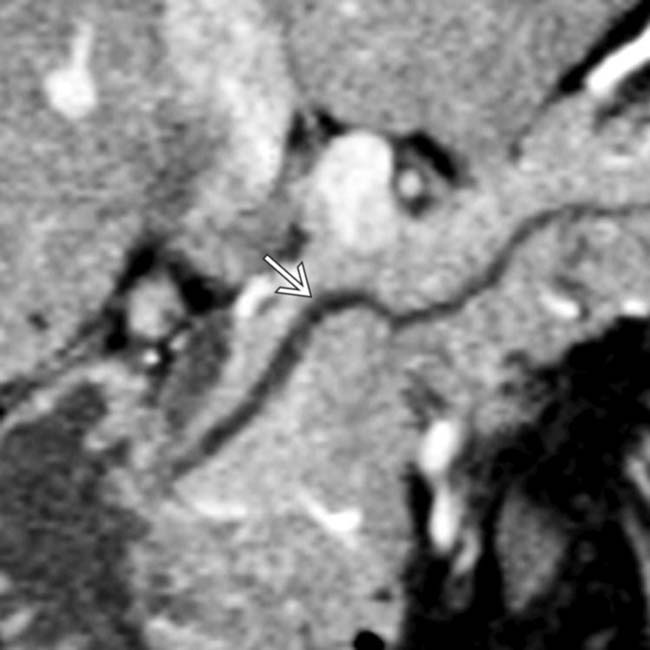
 demonstrates a normal duct. The characteristic location and the lack of mass effect on the duct are key findings to suggest the diagnosis of focal fatty infiltration.
demonstrates a normal duct. The characteristic location and the lack of mass effect on the duct are key findings to suggest the diagnosis of focal fatty infiltration.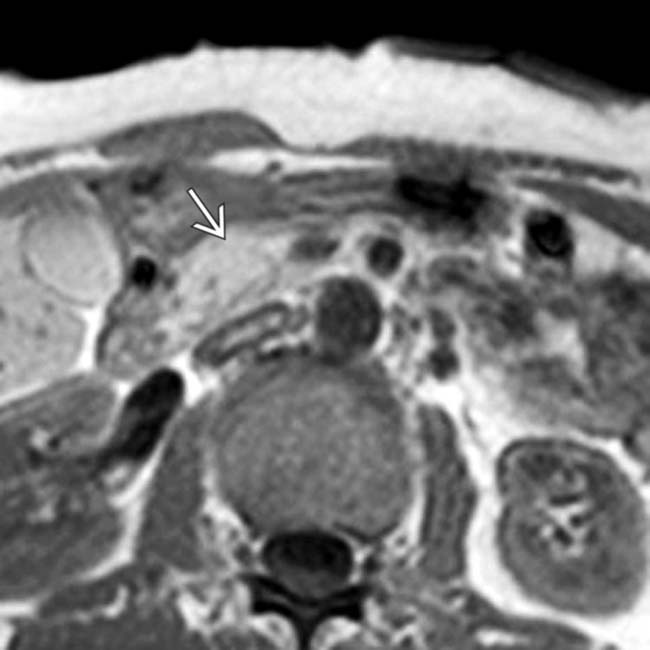
 . (Courtesy H. Harvin, MD.)
. (Courtesy H. Harvin, MD.)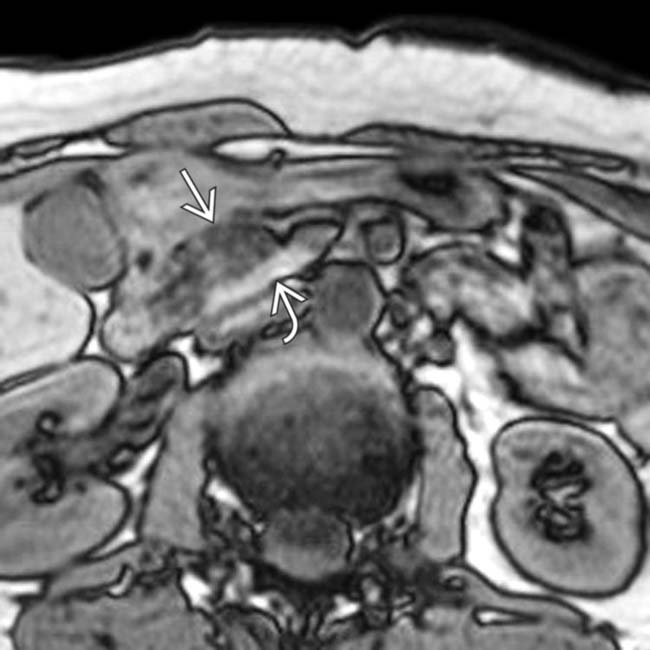
 in the anterior aspect of the head, a classic finding confirming asymmetric fatty lobulation. Note the preserved higher signal and lack of dropout from the normal pancreatic tissue in the uncinate process
in the anterior aspect of the head, a classic finding confirming asymmetric fatty lobulation. Note the preserved higher signal and lack of dropout from the normal pancreatic tissue in the uncinate process  . (Courtesy H. Harvin, MD.)
. (Courtesy H. Harvin, MD.)












 in the pancreatic head, representing a pancreatic lipoma. These lesions are rare, have a predisposition for the pancreatic head, and are much more well-defined and mass-like compared to focal fatty infiltration.
in the pancreatic head, representing a pancreatic lipoma. These lesions are rare, have a predisposition for the pancreatic head, and are much more well-defined and mass-like compared to focal fatty infiltration.
 in the anterior aspect of the pancreatic head. Note that this area results in no abnormality of the pancreatic contour, nor is there evidence of pancreatic or biliary ductal obstruction. There is a sharp linear margin between the low- density anterior head and the normal- density posterior head. This is a classic appearance for focal fatty infiltration.
in the anterior aspect of the pancreatic head. Note that this area results in no abnormality of the pancreatic contour, nor is there evidence of pancreatic or biliary ductal obstruction. There is a sharp linear margin between the low- density anterior head and the normal- density posterior head. This is a classic appearance for focal fatty infiltration.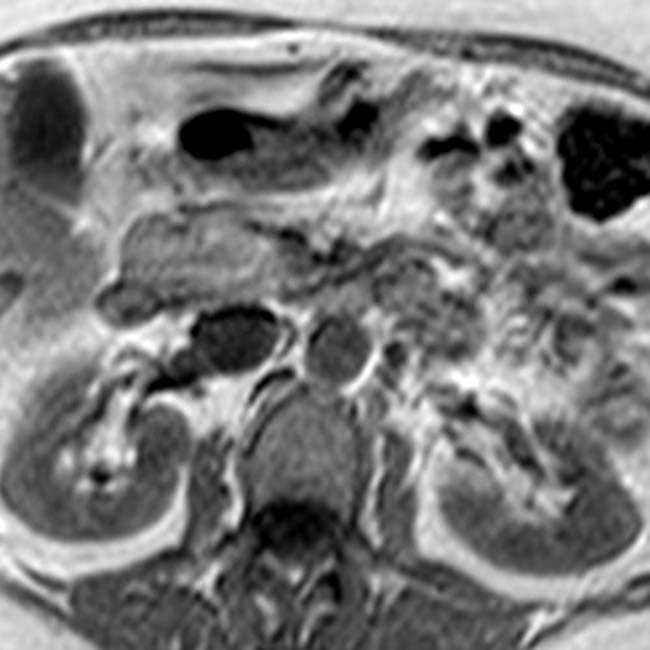
 corresponding to the low density seen in the anterior pancreatic head on CT, confirming the diagnosis of benign focal fatty infiltration. Chemical shift MR is the most sensitive modality for this diagnosis.
corresponding to the low density seen in the anterior pancreatic head on CT, confirming the diagnosis of benign focal fatty infiltration. Chemical shift MR is the most sensitive modality for this diagnosis.
