Disorders associated with a painful arc

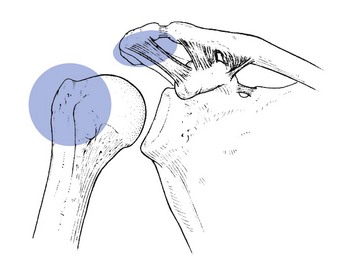
A painful arc is pain felt at about half range in a movement, in the absence of pain before and after the mid-range (see p. 213). Pain may or may not recur at the end of the movement. An arc results from a momentary impingement of a lesion, lying in such a position that it is caught between the lesser or greater humeral tuberosities and the overlying anterior part of the acromion, the coracoacromial ligament or the acromioclavicular joint1–4 (Fig. 1). A painful arc is mainly found on elevation, sometimes on medial rotation of the arm. Irrespective of the precipitating movement, the diagnostic significance remains the same: temporary impingement.
An arc on elevation is usually most pronounced during the active movement, and more on the way up than on the way down. This is due to the muscular activity, which pulls the humeral head closer to the acromion during active elevation.5
Sometimes the patient tries to avoid the painful moment by changing the direction of the elevation when the pain is felt. Indeed, some patients abduct until they feel the pain start at mid-range and then bring the arm in front of the body to avoid further impingement.
Occasionally the patient may experience the pain at mid-range only on the way down, or even on passive medial rotation. This has the same meaning as a painful arc on the way up. If the examiner has the impression that passive elevation or medial rotation is limited, it is important to insist that the movement is gently continued, otherwise the patient may voluntarily stop the movement too early, due to pain. The apparent limitation may be overcome by persistence, and it may be possible for the patient to then get beyond the painful moment. Thus, what might initially be regarded as a limited movement can be proved to be a painful arc with full range, which has completely different diagnostic implications.
Neer introduced the term ‘impingement syndrome’, now widely recognized and further divided into a ‘subacromial’ and a ‘subcoracoid’ impingement syndrome.6–9 Cyriax always considered painful impingement as a sign rather than a syndrome: it does not implicate just one lesion but one of several.10,11 Since the exact diagnosis is in the majority of the cases based on other tests – very often on resisted movements – a painful arc usually has value as a localizing sign, defining exactly in which particular part of the structure the lesion lies.
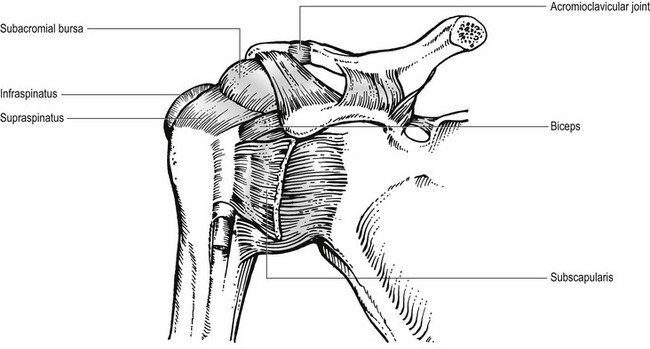
Movement in the subacromial space is between a convex, cuff-covered proximal humerus and a concave surface consisting of the coracoacromial roof and the inferior part of the acromioclavicular joint.12 The gliding surface between these two moving spheres is the bursa. Pathology in one or more of these structures may partly interfere with movement and thus cause the clinical sign, ‘painful arc’ (Fig. 2).
Disorders of the inert structures
Acute subdeltoid bursitis
In acute subdeltoid bursitis an arc is present for the first few hours after the onset. At the end of the spontaneous course, say after 4–5 weeks, when the pain has become much less, the arc appears again.
In practice, the arc is seldom found because the patient presents 2–3 days after the onset, once the pain has become unbearable. At this stage, the pain is so severe that active and passive elevation beyond the horizontal is not possible (see p. 234).
Chronic subdeltoid bursitis
In almost all cases of chronic subdeltoid bursitis a painful arc is present. Here it is not regarded as a localizing sign but as a basic element in the diagnosis. It is most commonly associated with pain at the end of all passive movements, sometimes as the only sign, sometimes combined with pain on resisted abduction and lateral rotation.
When an arc is very pronounced, the diagnosis is most probably chronic subdeltoid bursitis. Occasionally, the arc is very subtle. It may be absent on lateral elevation, but when it is repeated with the arm anteriorly it may show. The same goes for lateral elevation with the arm in medial or lateral rotation. In these cases, elevation should be repeated in several different ways (see p. 246).
Sprain of the acromioclavicular joint
Pain at the end of all passive movements, together with more pain on passive horizontal adduction is typical of a sprain of the acromioclavicular joint. In some cases, a painful arc is also present. It indicates that the lesion lies where it can impinge, which only happens to the inferior ligament. A sprain of the superficial ligament can never cause a painful arc but palpation elicits local tenderness.
Differentiation from a chronic subdeltoid bursitis may be very difficult. A diagnostic infiltration with local anaesthetic may be necessary (see p. 241).
Acromial metastases
This is a rare disorder. Due to the metastases, the acromion becomes so tender that even the slightest pressure from below or above causes severe local pain, which does not spread in the arm. In consequence, local tenderness on palpation and a painful arc are found. Resisted abduction is usually very painful and extremely weak. These signs, together with localized warmth, call for immediate radiography.
 Warning
WarningDisorders of the contractile structures
All the contractile structures mentioned below may give rise to a painful arc in that some part of them can be pinched between humerus and coracoacromial arch.13
Supraspinatus tendinitis
This is the most common cause of painful arc. For this reason, many authors consider that a painful arc usually means that the supraspinatus is involved.14,15 This is not so, since the arc should be regarded only as a localizing sign; resisted abduction identifies the structure at fault. If an arc is also present it shows the lesion to lie at the superficial (bursal) aspect of the tenoperiosteal insertion (see p. 253).
Infraspinatus tendinitis
In this case, pain on resisted lateral rotation is the basic sign. The arc shows the lesion to lie at the superficial aspect of the tenoperiosteal insertion (see p. 263).
Subscapularis tendinitis
Pain on resisted medial rotation draws attention to the subscapularis muscle. As the insertion of the subscapularis is about 3 cm long, only the proximal half of it can impinge on elevation. If the lesion lies in the lower half an arc is not found but passive horizontal adduction is painful (see p. 267).
Tendinitis of the long head of the biceps
This is a rare lesion which causes pain in the shoulder on resisted flexion and supination of the elbow. The combination of these signs with a painful arc means that the lesion must lie where it can impinge. The intra-articular part of the long head of the tendon is the only site.
Disorders mimicking painful arc
Capsular laxity of the shoulder
In some instances of shoulder instability the following is encountered: when the patient lifts the arm up sideways there is a little ‘stop’ at about midway but once beyond this point, the normal movement continues. At the same time, the patient has the impression that something comes out of place and then slips back. In this event, the stop is caused by a partial dislocation of the humeral head, which slips back when the movement continues. Such momentary subluxation is not usually painful. It has nothing to do with an impingement and therefore is not regarded as a painful arc. Recent investigations have shown that slight instability of the shoulder may be one of the precipitating factors in the development of rotator cuff disease. It is therefore highly possible that subluxation of the humerus coexists with a lesion of one of the rotator cuff tendons and thus with a painful arc.16–19
Apprehension tests for shoulder instability must be performed to arrive at the diagnosis. It can also be helpful to palpate the shoulder joint during active elevation (see Chapter 14).
Snapping biceps tendon
Sometimes the long head of the biceps may slip out of the groove on active elevation, giving rise to a momentary sensation of instability. No pain is present but a sort of popping may be felt. Because no impingement occurs, this sensation cannot be regarded as a painful arc. The biceps dislocation test reveals the exact nature of the lesion (see p. 271).
Cervical disc lesion
In a cervical discodural interaction, neck and scapulo-humeral pain is sometimes provoked or increased at about mid-range during active elevation. Passive tests of the shoulder are fully negative, although some resisted movements may be painful. At the cervical spine, a partial articular pattern is found.
The presence of a painful arc in combination with signs and symptoms of a discodural interaction at the neck may confuse the examiner. Two possibilities then emerge: either the painful arc is caused by the neck problem or there is a double lesion – one at the neck and one at the shoulder.
In the former, the arc is usually felt in the scapular area, sometimes radiating down the arm. Scapular localization of the pain is very seldom due to a shoulder problem. The pain at mid-range on elevation is then explained by the muscular tension at the neck becoming greatest around the horizontal. The momentary pain cannot be considered as a true painful arc: the sign results from transmitted stress and is not provoked by any kind of impingement.
However, it is not always easy to be absolutely sure whether there is only one lesion or whether there are more. It is wise in these doubtful cases to start treating the most proximally located disorder (the neck) until all neck signs become normal: full range, no pain. The shoulder should then be re-examined and, if still painful, a shoulder problem must also be present and is then dealt with.
Disorders associated with painful arc are listed in Box 1.
References
1. Solem-Bertoft, E, Thuomas, K, Esterberg, C, The influence of scapular retraction and protraction on the width of the subacromial space. Clin Orthop Rel Res 1993; 296:99–103. 
2. Worland, R, Treatment of rotator cuff impingement. Orthop Rev 1993; 76–79. 
3. Rockwood, C, Lyons, F, Shoulder impingement syndrome: diagnosis, radiographic evaluation and treatment with a modified Neer acromioplasty. J Bone Joint Surg. 1993;75A(3):409–424. 
4. Burns, W, Whipple, T, Anatomic relationships in the shoulder impingement syndrome. Clin Orthop Rel Res 1993; 294:96–102. 
5. Sigholm, G, Styf, J, Herberts, P, Pressure recording in the subacromial bursa. J Orthop Res 1988; 6:123–128. 
6. Neer, C, Anterior acromioplasty for the chronic impingement syndrome of the shoulder. J Bone Joint Surg 1972; 54A:41. 
7. Post, M, Cohen, J, Impingement syndrome, a review of late stage II and early stage III lesions. Clin Orthop Rel Res 1986; 207:126–132. 
8. Patte, D, The subcoracoid impingement. Clin Orthop Rel Res 1990; 254:81–86. 
9. Ha’eri, G, Orth, M, Wiley, A, Shoulder impingement syndrome – results of operative release. Clin Orthop Rel Res 1982; 168:128–132. 
10. Cyriax, JH. Textbook of Orthopaedic Medicine, vol I, Diagnosis of Soft Tissue Lesions, 8th ed. London: Baillière Tindall; 1982.
11. Fu, F, Harner, C, Klein, A, Shoulder impingement syndrome. A critical review. Clin Orthop Rel Res 1991; 269:162–173. 
12. Harryman, DT, Sidles, JA, Clark, JM, et al, Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Joint Surg 1990; 27A:1334–1342. 
13. Abrams, J, Special shoulder problems in the throwing athlete: pathology, diagnosis, and nonoperative management. Clin Sports Med. 1991;10(4):839–861. 
14. Hawkins, R, Abrams, J, Impingement syndrome in the absence of rotator cuff tear (stages I and II). Orthop Clin North Am. 1987;18(3):373–382. 
15. Neer, C, Impingement lesions. Clin Orthop Rel Res 1983; 173:70–77. 
16. Jobe, F, Giangarra, C, Kvitne, R, Anterior capsulolabral reconstruction of the shoulder in athletes in overhand sports. Am J Sports Med 1991; 19:428–434. 
17. Flatow, EL, Soslowsky, LJ, Ticker, JB, et al, Excursion of the rotator cuff under the acromion. Patterns of subacromial contact. Am J Sports Med 1994; 22:779–788. 
18. Lazarus, MD, Harryman, DT, Yung, SW, et al, Anterosuperior humeral displacement: limitation by the coracoacromial arch. AAOS Annual Meeting, Orlando, 1995.. 
19. Poppen, LA, Walter, KS, Normal and abnormal motion of the shoulder. J Bone Joint Surg 1976; 58A:195. 

