Chapter 9 Arterial system
Methods of imaging the arterial system
Collins R., Cranny G., Burch J., et al. A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease. Health Technol. Assess.. 2007;11(20):iii-iv. xi–xiii, 1–184
Kaufman J.A., Lee M.J., editors. Vascular and Interventional Radiology: The Requisites. Philadelphia: Elsevier-Mosby, 2004.
Introduction to Catheter Techniques
The basic technique of arterial catheterization is also applicable to veins.
Patient preparation
Equipment for the Seldinger technique
Needles
Guidewires
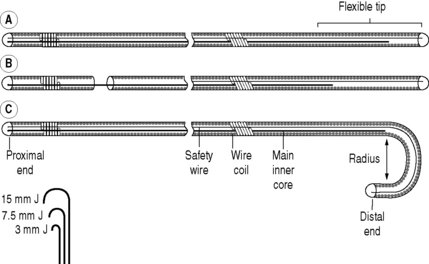
Basic guidewires consist of two central cores of straight wire around which is a tightly wound coiled wire spring (Fig. 9.1). The ends are sealed with solder. One of the central core wires is secured at both ends – a safety feature in case of fracturing. The other is anchored in solder at one end, but terminates 5 cm from the other end, leaving a soft flexible tip. Some guidewires have a movable central core so the tip can be flexible or stiff. Others have a J-shaped tip which is useful for negotiating vessels with irregular walls. The size of the J-curve is denoted by its radius in mm. Guidewires are polyethylene coated but may be coated with a thin film of Teflon to reduce friction. Teflon, however, also increases the thrombogenicity, which can be countered by using heparin-bonded Teflon. The most common sizes are 0.035 and 0.038 inch diameter. A more recent development is hydrophilic guidewires. These frequently have a metal mandrel as their core. They are very slippery with excellent torque and are useful in negotiating narrow tortuous vessels. They require constant lubrication with saline.
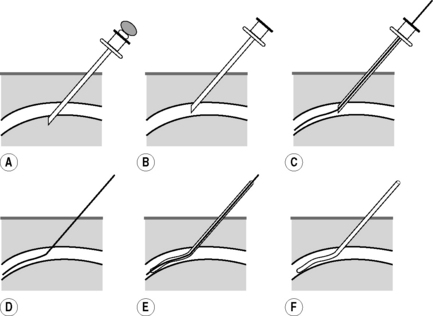
FEMORAL ARTERY PUNCTURE
This is the most frequently used puncture site providing access to the left ventricle, aorta and its branches and has the lowest complication rate of the peripheral sites.
Technique (Fig. 9.2)
High Brachial Artery Puncture
AXILLARY ARTERY PUNCTURE
GENERAL COMPLICATIONS OF CATHETER TECHNIQUES
Due to the technique
Diagnostic angiography is an invasive procedure and complications are expected. The majority of these are minor, e.g. groin haematoma. Recommended upper limits for complication rates have been produced by the Society of Cardiovascular and Interventional Radiology (SCVIR):1 these rates are included in the following discussion.
Local
Distant
Ascending Aortography
Indications
Contrast medium
Low osmolar contrast material (LOCM) 370, 0.75 ml kg−1 (max. 40 ml). Inject at 18–20 ml s−1.

ARTERIOGRAPHY OF THE LOWER LIMB
Methods
Both lower limbs
BALLOON ANGIOPLASTY
Also known as percutaneous transluminal angioplasty or balloon dilation.
Indications
Equipment
Technique
Principles
Renal arteries
Iliac arteries
Femoral arteries (common, and origins of superficial femoral and profunda arteries)
Superficial femoral and popliteal arteries
Catheter-directed arterial thrombolysis
It is an important tool in the management of thrombosed haemodialysis access.
Aftercare
Complications
Due to technique
1 Ouriel K., Shortell C.K., DeWeese J.A., et al. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J. Vasc. Surg.. 1994;19:1021-1030.
2 Dawson K., Armon A., Braithwaite B.D., et al. Stroke during intra-arterial thrombolysis: a survey of experience in the UK (abstr). Br. J. Surg.. 1996;83:5-8.
Vascular Embolization
Indications
Equipment
Technique
Principles
Complications
VASCULAR ULTRASOUND
The main components of arterial vascular US studies are:
Computed Tomographic Angiography
Although CTA involves administration of iodinated contrast (see Chapter 2) and significant radiation dose, there are many advantages: imaging is very rapid – usually less than 30 s to acquire the main dataset even for extended scans including lower limbs, scanners are readily available, unstable patients can be monitored with standard equipment, and valuable information is obtained about the blood vessel wall and surrounding structures.
PERIPHERAL (LOWER LIMB) COMPUTED TOMOGRAPHIC ANGIOGRAPHY
Description of other specific CTA methods are found in appropriate chapters.
Patient preparation
General precautions for use of ionizing radiation (Chapter 1) and iodinated contrast (Chapter 2). The nature and purpose of the examination is explained to the patient.
Technique
For optimum images a MDCT scanner with at least a 16 slice detector is used:
Magnetic Resonance Angiography
Guidelines on MR safety and selection of patients must be followed (see Chapter 1).
MR angiography (MRA) is now in widespread clinical use and is a highly sensitive and specific tool for assessment of the arterial system. For most examinations contrast-enhanced MRA with i.v. gadolinium (see Chapter 2) is now the preferred method. Gadolinium i.v. shortens the T1 relaxation time of blood so blood appears bright when imaged with a very short TR (repetition time) and other structures on the image appear dark. Timing of the contrast injection is critical. Imaging without contrast is used infrequently, but may be either a ‘bright blood’ cine technique, to demonstrate both anatomical and functional data, or ‘black blood’ imaging, which gives useful morphological information.
Earls J.P., Edelman R.R. Magnetic resonance angiography: body applications. In: Edelman R.R., Hesselink J.R., Zlatkin M.B., et al, editors. Clinical Magnetic Resonance Imaging. Philadelphia: Saunders-Elsevier, 2006.
Ho V.B., Corse W.R. MR angiography of the abdominal aorta and peripheral vessels. Radiol. Clin. North Am.. 2003;41(1):115-144.



