Chapter 30 Aortic Dissection
3 Describe the DeBakey and Stanford classifications of aortic dissection
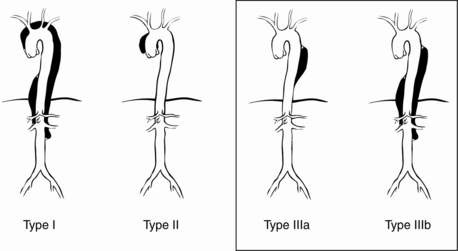
The DeBakey classification describes three types of dissection (Fig. 30-1):
 Type I: extends from aortic root to beyond the ascending aorta
Type I: extends from aortic root to beyond the ascending aorta
 Type II: involves only the ascending aorta
Type II: involves only the ascending aorta
 Type III: begins distal to the takeoff of the left subclavian artery and has two subtypes
Type III: begins distal to the takeoff of the left subclavian artery and has two subtypes


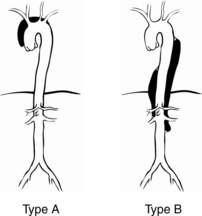
The Stanford classification has two types of dissection (Fig. 30-2):


5 What are the risk factors and associated conditions for dissection?









6 Describe the common clinical signs and symptoms of aortic dissection
 Pain: The most common presenting symptom is chest pain, occurring in up to 90% of patients with acute dissection. Classically, for type A dissections, sudden onset of severe anterior chest pain with extension to the back occurs that is described as ripping or tearing in nature. However, in the IRAD, pain was more often described as sharp rather than ripping or tearing. The pain is usually of maximal intensity from its inception and is frequently unremitting. It may migrate along the path of the dissection. The pain of aortic dissection may mimic that of myocardial ischemia. Patients with type B dissections are more likely to be seen with back pain (64%) alone.
Pain: The most common presenting symptom is chest pain, occurring in up to 90% of patients with acute dissection. Classically, for type A dissections, sudden onset of severe anterior chest pain with extension to the back occurs that is described as ripping or tearing in nature. However, in the IRAD, pain was more often described as sharp rather than ripping or tearing. The pain is usually of maximal intensity from its inception and is frequently unremitting. It may migrate along the path of the dissection. The pain of aortic dissection may mimic that of myocardial ischemia. Patients with type B dissections are more likely to be seen with back pain (64%) alone.

7 Describe the common clinical findings associated with aortic dissection
 Neurologic symptoms. The reported frequency of neurologic symptoms in pooled data of type A and B dissections approaches 17%; in type A alone, 29% of patients were seen initially with neurologic symptoms, 53% of which represented ischemic stroke. Neurologic complications may result from hypotension, malperfusion, distal thromboembolism, or nerve compression. Acute paraplegia as a result of spinal cord malperfusion has been described as a primary manifestation in 1% to 3% of patients. Up to 50% of neurologic symptoms may be transient.
Neurologic symptoms. The reported frequency of neurologic symptoms in pooled data of type A and B dissections approaches 17%; in type A alone, 29% of patients were seen initially with neurologic symptoms, 53% of which represented ischemic stroke. Neurologic complications may result from hypotension, malperfusion, distal thromboembolism, or nerve compression. Acute paraplegia as a result of spinal cord malperfusion has been described as a primary manifestation in 1% to 3% of patients. Up to 50% of neurologic symptoms may be transient.

 Acute aortic regurgitation may be present in 41% to 76% of patients with proximal dissection and may be caused by widening of the aortic annulus resulting in incomplete valve closure or actual disruption of the aortic valve leaflets from the dissection flap. Clinical manifestations of dissection-related aortic regurgitation span from mere diastolic murmurs without clinical significance to overt congestive heart failure and cardiogenic shock.
Acute aortic regurgitation may be present in 41% to 76% of patients with proximal dissection and may be caused by widening of the aortic annulus resulting in incomplete valve closure or actual disruption of the aortic valve leaflets from the dissection flap. Clinical manifestations of dissection-related aortic regurgitation span from mere diastolic murmurs without clinical significance to overt congestive heart failure and cardiogenic shock.
















12 What are the strategies for medical management of dissection and commonly used medications?



Acknowledgment
Key Points Diagnosis and Treatment of Acute Aortic Dissection
1. Aortic dissection is classically associated with sudden chest or back pain, a pulse deficit, and mediastinal widening on chest radiograph.
2. The imaging modality (CT, MRI, or TEE) that is most readily available should be the one selected to confirm the diagnosis of acute aortic dissection.
3. An acute type A aortic dissection is a surgical emergency. Although type B dissections are usually managed medically, one third of these patients eventually require surgery because of worsening of the dissection, rupture, malperfusion, or intractable pain. In either case, prompt surgical consultation is recommended.
4. When managing acute aortic dissection, adequate β-blockade must be established before the initiation of nitroprusside to prevent propagation of the dissection from a reflex increase in cardiac output.
5. The use of endovascular stent-grafts will likely play a large role in the management of dissections.
1 Akin I., Kische S., Rehders T.C., et al. Thoracic endovascular stent-graft therapy in aortic dissection. Curr Opin Cardiol. 2010;25:552–559.
2 Clouse W.D., Hallett J.W.Jr. Schaff HV, et al: Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clin Proc. 2004;79:176–180.
3 Eggebrecht H., Nienaber C., Neuhauser M., et al. Endovascular stent-graft placement in aortic dissection: a meta-analysis. Eur Heart J. 2006;27:489–498.
4 Ehrlich M.P., Dumfarth J., Schoder R., et al. Midterm results after endovascular treatment of acute, complicated type B aortic dissection. Ann Thorac Surg. 2010;90:1444–1448.
5 Estrera A.L., Miller C.C.III. Safi HJ, et al: Outcomes of medical management of acute type B aortic dissection. Circulation. 2006;114(Suppl 1):I384–I389.
6 Hagan P.G., Nienaber C.A., Isselbacher E.M., et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283:897–903.
7 Hiratzka L.F., Bakris G.L., Beckman J.A., et al. 2010 CCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. Circulation. 2010;121:e266–e369.
8 Khoynezhad A., Plestis K.A. Managing emergency hypertension in aortic dissection and aortic aneurysm surgery. J Card Surg. 2006;21(Suppl 1):S3–S7.
9 Leurs L.J., Bell R., Degrieck Y., et al. Endovascular treatment of thoracic aortic diseases: combined experience from the EUROSTAR and United Kingdom Thoracic Endograft registries. J Vasc Surg. 2004;40:670–680.
10 Nienaber C., Rousseau H., Eggebrecht H. Randomized comparison of strategies for type-B aortic dissection. The Investigation of Stent Grafts in Aortic Dissection (INSTEAD) trial. Circulation. 2009;120:2519–2528.
11 Olsson C., Thelin S., Stahle E., et al. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114:2611–2618.
12 Parsa C.J., Schroder J.N., Daneshmand M.A., et al. Midterm results for endovascular repair of complicated acute and chronic type B aortic dissection. Ann Thorac Surg. 2010;89:97–102.
13 Trimarchi S., Nienaber C.A., Rampoldi V., et al. Role and results of surgery in acute type B aortic dissection: insights from the International Registry of Acute Aortic Dissection (IRAD). Circulation. 2006;14(Suppl 1):I357–I364.
14 Yagdi T., Atay Y., Engin C., et al. Impact of organ malperfusion on mortality and morbidity in acute type A aortic dissections. J Card Surg. 2006;21:363–369.
15 Zoli S., Etz C.D., Roder F., et al. Long-term survival after open repair of chronic distal aortic dissection. Ann Thorac Surg. 2010;89:1458–1466.
