Chapter 538 Anomalies of the Penis and Urethra
Hypospadias
Clinical Manifestations
Hypospadias is classified according to the position of the urethral meatus after taking into account whether chordee is present (Fig. 538-1). The deformity is described as glanular (on the glans penis), coronal, subcoronal, midpenile, penoscrotal, scrotal, or perineal. Approximately 60% of cases are distal, 25% are subcoronal or midpenile, and 15% are proximal. In the most severe cases, the scrotum is bifid and sometimes there is moderate penoscrotal transposition. As many as 15% of affected boys have a megameatal variant, in which the foreskin is developed normally (megameatus intact prepuce [MIP] variant), and there is either glanular or subcoronal hypospadias with a “fish mouth” meatus. These cases might not be diagnosed until after a circumcision is performed.

Approximately 10% of boys with hypospadias have an undescended testis; inguinal hernias also are common. In the newborn, the differential diagnosis of proximal hypospadias associated with an undescended testis should include forms of a disorder of sexual differentiation, particularly female virilization (congenital adrenal hyperplasia), mixed gonadal dysgenesis, partial androgen insensitivity, and true hermaphroditism. A karyotype should be obtained in patients with midpenile or proximal hypospadias and cryptorchidism (Chapter 577). In boys with penoscrotal hypospadias, a voiding cystourethrogram should be considered because 5-10% of these children have a dilated prostatic utricle, which is a remnant of the müllerian system (Chapter 548). The incidence of upper urinary tract abnormalities is low unless there are abnormalities of other organ systems.
Chordee without Hypospadias
In some boys there is mild or moderate ventral penile curvature (chordee) and incomplete development of the foreskin (dorsal hood), but the urethral meatus is at the tip of the glans (Fig. 538-2). In most of these boys, the urethra is normal but there is insufficient ventral penile skin or prominent, inelastic ventral bands of dartos fascia that prevent a straight erection. In some cases, the urethra is hypoplastic, and a formal urethroplasty is necessary for repair. The only sign of this anomaly in the neonate may be the hooded foreskin, and delayed repair under general anesthesia at 6 mo of age is recommended.
Phimosis and Paraphimosis
Phimosis refers to the inability to retract the prepuce. At birth, phimosis is physiologic. Over time, the adhesions between the prepuce and glans lyse and the distal phimotic ring loosens. In 90% of uncircumcised boys the prepuce becomes fully retractable by 3 yr of age. Accumulation of epithelial debris under the infant’s prepuce is physiologic and does not mandate circumcision. In older boys, phimosis may be physiologic, may be pathologic from inflammation and scarring at the tip of the foreskin (Fig. 538-3), or occurs after circumcision. The prepuce might have been retracted forcefully on 1 or 2 occasions in the past, which can result in a cicatricial scar that prevents subsequent retraction of the foreskin. In boys with persistent physiologic or pathologic phimosis, application of corticosteroid cream to the foreskin 3 times daily for 1 mo loosens the phimotic ring in 2/3 of cases. If there is ballooning of the foreskin during voiding or phimosis beyond 10 yr of age and topical corticosteroid therapy is ineffective, circumcision is recommended.

Paraphimosis occurs when the foreskin is retracted past the coronal sulcus and the prepuce cannot be pulled back over the glans (Fig. 538-4). Painful venous stasis in the retracted foreskin results, with edema leading to severe pain and inability to reduce the foreskin (pull it back over the glans). Treatment includes lubricating the foreskin and glans and then simultaneously compressing the glans and placing distal traction on the foreskin to try to push the phimotic ring past the coronal sulcus. In rare cases, emergency circumcision under general anesthesia is necessary.

Circumcision
UTIs are 10-15 times more common in uncircumcised infant boys than in circumcised infants, with the urinary pathogens arising from bacteria that colonize the space between the prepuce and glans. The risk of febrile UTI (Chapter 532) is highest between birth and 6 mo, but there is an increased risk of UTI until 5 yr of age. Many recommend circumcision in infants who are predisposed to UTI, such as those with congenital hydronephrosis and vesicoureteral reflux. Circumcision reduces the risk of sexually transmitted infections in adults (Chapter 114), in particular AIDS (Chapter 268). There have been only a handful of reports of men who were circumcised at birth and subsequently acquired penile carcinoma, but in Scandinavian countries, where few men are circumcised and hygiene is good, the incidence of penile cancer is low.
Complications after neonatal circumcision include bleeding, wound infection, meatal stenosis, secondary phimosis, removal of insufficient foreskin, and fibrous penile adhesions (skin bridge; Fig. 538-5); 0.2-3.0% of patients undergo a subsequent operative procedure. Boys with a large hydrocele or hernia are at particular risk for secondary phimosis because the scrotal swelling tends to displace the penile shaft skin over the glans. Potentially serious complications include sepsis, amputation of the distal part of the glans, removal of an excessive amount of foreskin, and urethrocutaneous fistula. Circumcision should not be performed in neonates with hypospadias, chordee without hypospadias, or a dorsal hood deformity (relative contraindication) or in those with a small penis (Fig. 538-6). In boys with a wandering raphe, in which the median raphe deviates to one side, there may be underlying penile torsion or hypospadias, and evaluation by a pediatric urologist is suggested before performing a circumcision.


Penile Torsion
Penile torsion is a rotational defect of the penile shaft. It usually occurs in a counterclockwise direction, that is, to the left side (see Fig. 538-6). In most cases, penile development is normal, and the condition is unrecognized until circumcision is performed or the foreskin is retractable. In many cases the midline raphe of the penile shaft is deviated. Penile torsion also occurs in some boys with hypospadias. The defect has primarily cosmetic significance and correction is unnecessary if the rotation is <60 degrees from the midline.
Inconspicuous Penis
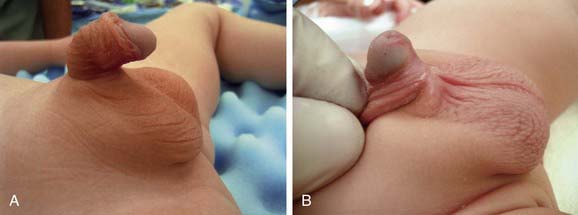
The term inconspicuous penis refers to a penis that appears to be small. A webbed penis is a condition in which the scrotal skin extends onto the ventral penile shaft. This deformity represents an abnormality of the attachment between the penis and scrotum. Although the deformity might appear mild, if a routine circumcision is performed, the penis can retract into the scrotum, resulting in secondary phimosis (trapped penis). The concealed (hidden or buried) penis is a normally developed penis that is camouflaged by the suprapubic fat pad (Fig. 538-7). This anomaly may be congenital, iatrogenic after circumcision, or a result of obesity. Surgical correction is indicated for cosmetic reasons or if there is a functional abnormality with a splayed stream.
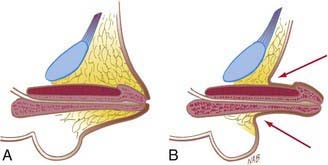
Figure 538-7 Concealed penis (A), which may be visualized by retracting skin lateral to penile shaft (B).
(From Wein AJ, Kavoussi LR, Novick AC, et al, editors: Campbell-Walsh urology, ed 9, Philadelphia, 2007, Saunders.)
A trapped penis is an acquired form of inconspicuous penis and refers to a phallus that becomes embedded in the suprapubic fat pad after circumcision (Fig. 538-8). This deformity can occur after neonatal circumcision in an infant who has significant scrotal swelling from a large hydrocele or inguinal hernia or after routine circumcision in an infant with a webbed penis. This complication can predispose to UTIs and can cause urinary retention. Initial treatment of a trapped penis should include topical corticosteroid cream, which often loosens the phimotic ring. In some cases secondary repair is necessary at 6-9 mo.

Micropenis
Micropenis is defined as a normally formed penis that is at least 2.5 standard deviations below the mean in size (Fig. 538-9). Typically, the ratio of the length of the penile shaft to its circumference is normal. The pertinent measurement is the stretched penile length, which is measured by stretching the penis and measuring the distance from the penile base under the pubic symphysis to the tip of the glans. The mean length of the term newborn penis is 3.5 ± 0.7 cm and the diameter is 1.1 ± 0.2 cm. The diagnosis of micropenis is made if the stretched length is <1.9 cm.

Figure 538-9 Micropenis secondary to hypopituitarism in an 8-year-old boy.
(From Wein AJ, Kavoussi LR, Novick AC, et al, editors: Campbell-Walsh urology, ed 9, Philadelphia, 2007, Saunders.)
Micropenis results from a hormonal abnormality that occurs after 14 wk of gestation. Common causes include hypogonadotropic hypogonadism, hypergonadotropic hypogonadism (primary testicular failure), and idiopathic micropenis. If growth hormone deficiency also is present, neonatal hypoglycemia can occur. The most common cause of micropenis is failure of the hypothalamus to produce an adequate amount of gonadotropin-releasing hormone, as typically occurs in Kallmann syndrome (Chapter 577), Prader-Willi syndrome (Chapter 102), and Lawrence-Moon-Biedl syndrome. In some cases, there is growth hormone deficiency. Primary testicular failure can result from gonadal dysgenesis or rudimentary testes syndrome and also occurs in Robinow syndrome (characterized by hypoplastic genitalia, shortening of the forearms, frontal bossing, hypertelorism, wide palpebral fissures, short broad nose, long philtrum, small chin, brachydactyly, and a normal karyotype).
Priapism
The most common cause of priapism in children is sickle cell disease, which is characterized by predominance of sickle hemoglobin (Hb SS; Chapter 456.1). As many as 27.5% of children with sickle cell disease develop priapism. The priapism is generally related to a low-flow state, secondary to sickling of red blood cells within the sinusoids of the corpora cavernosa during normal erection, resulting in venous stasis. This situation results in decreased local oxygen tension and pH, which potentiates further stasis and sickling. Priapism typically occurs during sleep, when mild hypoventilatory acidosis depresses oxygen tension and pH in the corpora. There is typically significant corporal engorgement with sparing of the glans penis. If the spongiosum is involved, voiding may be impaired. Evaluation includes complete blood count and serum chemistry. If sickle cell status is unknown, hemoglobin electrophoresis should be performed. In some cases, corporal aspiration is performed to distinguish between a high-flow and low-flow state. Other causes of low-flow priapism include sildenafil ingestion and leukemia.
Meatal Stenosis
Meatal stenosis is a condition that almost always is acquired and occurs after neonatal circumcision. It probably results from severe inflammation of the denuded glans. If the meatus is pinpoint, boys void with a forceful, fine stream that goes a great distance. These boys can experience dysuria, frequency, hematuria, or a combination of these conditions, typically at age 3-8 yr. UTI is uncommon. Other boys have dorsal deflection of the urinary stream. Although the meatus may be small, hydronephrosis or voiding difficulty is extremely rare unless there is associated balanitis xerotica obliterans (see Fig. 538-3; chronic dermatitis of unknown etiology, generally involving the glans and prepuce, occasionally extending into the urethra). Treatment is meatoplasty, in which the urethral meatus is opened surgically; this procedure can be performed either under anesthesia as an outpatient or in the office using local anesthesia (EMLA cream) with or without sedation. Routine cystoscopy is unnecessary.
Other Male Urethral Anomalies
Parameatal urethral cyst manifests as an asymptomatic small cyst on one side of the urethral meatus. Treatment is excision under anesthesia. Congenital urethral fistula is a rare deformity in which a fistula is present from the penile urethra. It usually is an isolated abnormality. Treatment is fistula closure. Megalourethra is a large urethra that usually is associated with abnormal development of the corpus spongiosum. This condition is most commonly associated with prune-belly syndrome (Chapter 534). Urethral duplication is a rare condition in which the two urethral channels lie in the same sagittal plane. There are many variations with complete and incomplete urethral duplication. These boys often have a double stream. Most commonly the dorsal urethra is small and the ventral urethra is normal caliber. Treatment involves excision of the small urethra. Urethral hypoplasia is a rare condition in which the urethra is extremely small but patent. In some cases, a temporary cutaneous vesicostomy is necessary for satisfactory urinary drainage. Either gradual enlargement of the urethra or major urethroplasty is necessary. Urethral atresia refers to maldevelopment of the urethra and nearly always is fatal unless the urachus remains patent throughout gestation.
Urethral Prolapse (Female)
Urethral prolapse is encountered predominantly in black girls 1-9 yr of age. The most common signs are bloody spotting on the underwear or diaper, although dysuria or perineal discomfort also can occur (Fig. 538-10). An inexperienced examiner can mistake the finding for sexual abuse. The usual therapy consists of application of estrogen cream 2-3 times daily for 3-4 wk and sitz baths. Surgical excision and reapproximation of the mucosal edges is curative.

Other Female Urethral Lesions
Paraurethral cyst results from retained secretions in the Skene glands secondary to ductal obstruction (Fig. 538-11). These lesions are present at birth, and most regress in size during the first 4-8 wk, although occasionally incision and drainage is necessary. A prolapsed ectopic ureterocele appears as a cystic mass protruding from the urethra and is a presenting symptom in 10% of girls with a ureterocele, which is a cystic swelling of the terminal ureter (Fig. 538-12). Ultrasonography should be performed to visualize the upper urinary tracts to confirm the diagnosis. Usually, either the ureterocele is incised or an upper urinary tract reconstructive procedure is necessary.


Allen L. Disorders of sexual development. Obstet Gynecol Clin North Am. 2009;36:25-45.
Bauer R, Kogan BA. Modern technique for penile torsion repair. J Urol. 2009;182:286-290.
Dickerman JD. Circumcision in the time of HIV: when is there enough evidence to revise the American Academy of Pediatrics’ policy on circumcision? Pediatrics. 2007;119:1006-1007.
Elder JS. Abnormalities of the genitalia in boys and their surgical management. In: Wein AJ, Kavoussi LR, Novick AC, et al, editors. Campbell-Walsh urology. ed 9. Philadelphia: Saunders; 2007:3745-3760.
Hoag CC, Gotto GT, Morrison KB, et al. Long-term functional outcome and satisfaction of patients with hypospadias repaired in childhood. Can Urol Assoc J. 2008;2:23-31.
Jones BC, O’Brien M, Chase J, et al. Early hypospadias surgery may lead to a better long-term psychosexual outcome. J Urol. 2009;182:1744-1749.
Lund L, Engebjerg MC, Pedersen L, et al. Prevalence of hypospadias in Danish boys: a longitudinal study, 1977–2005. Eur Urol. 2009;55:1022-1026.
Malone P, Steinbrecher H. Medical aspects of male circumcision. BMJ. 2007;335:1206-1209.
Montague DK, Jarow J, Broderick GJ, et al. American Urological Association Guideline on the management of priapism. J Urol. 2003;170:1318-1324.
Moriya K, Kakizaki H, Tanaka H, et al. Long-term patient reported outcome of urinary symptoms after hypospadias surgery: norm related study in adolescents. J Urol. 2007;178:1659-1662.
Pohl HG, Joyce GF, Wise M, et al. Cryptorchidism and hypospadias. J Urol. 2007;177:1646-1651.
Prais D, Shoov-Furman R, Amir J. Is ritual circumcision a risk factor for neonatal urinary tract infections? Arch Dis Child. 2009;94:191-194.
Schonbucher VB, Landolt MA, Gobet R, et al. Psychosexual development of children and adolescents with hypospadias. J Sex Med. 2008;5:1365-1373.
Sharma S, Gupta DK. Gender assignment and hormonal treatment for disorders of sexual differentiation. Pediatr Surg Int. 2008;24:1131-1135.
Tobian AA, Serwadda D, Quinn TC, et al. Male circumcision for the prevention of HSV-2 and HPV infections and syphilis. N Engl J Med. 2009;360:1298-1309.