[level-membership-for-radiology-category] Incomplete annular pancreas: Pancreatic tissue may extend anterolateral or posterolateral to duodenum or anterior and posterior to duodenum (“crocodile-jaw” configuration)
• MR: Normal pancreatic tissue (with identical signal to normal pancreas) encircling duodenum
MRCP: Main pancreatic duct encircling duodenum (and abnormally extending to right side of duodenum)
Secretin dilates duct and facilitates diagnosis
• Fluoroscopic barium study (upper GI): Extrinsic smooth compression and narrowing of 2nd part of duodenum
• ERCP: Duct draining pancreatic head encircles the duodenum and joins normal main pancreatic duct
TOP DIFFERENTIAL DIAGNOSES
• Duodenal carcinoma
• Pancreatic ductal carcinoma
• Postbulbar peptic ulcer
• Multiple other causes of duodenal stenosis
PATHOLOGY
• Etiology: Incomplete rotation of ventral anlage leads to pancreatic tissue encircling 2nd part of duodenum
Other congenital anomalies in up to 75% of pediatric cases (Down syndrome, duodenal atresia, etc.)
CLINICAL ISSUES
• 50% of cases present in infancy due to gastric outlet obstruction
• Most adults asymptomatic, but rare symptoms include gastric obstruction, upper GI bleeding, and jaundice
Rare symptoms include partial gastric outlet obstruction, upper GI bleeding, abdominal pain, and obstructive jaundice
• Associated in adults with gastric/duodenal ulcers and pancreatitis; questionable link with pancreatic cancer
(Left) Graphic shows concentric luminal narrowing of the 2nd portion of the duodenum by encircling annular pancreatic tissue. The pancreatic head duct also encircles the descending duodenum. Note the proximal duodenal dilatation .
(Right) ERCP shows a small pancreatic head duct originating on the right anterior surface of the duodenum, encircling it, and emptying into the main pancreatic duct near the ampulla .
(Left) Axial CECT demonstrates pancreatic tissue completely encircling the duodenum . Notice the different enhancement of the pancreatic tissue and the duodenal wall.
(Right) Sagittal CECT in the same patient demonstrates that the duodenum is narrowed by pancreatic tissue both anteriorly and posteriorly. While adults with annular pancreas are usually asymptomatic, this patient was experiencing intermittent obstruction and early satiety.
Axial CECT shows pancreatic tissue completely encircling the 2nd part of the duodenum .
Upper GI series shows circumferential narrowing of the lumen of the 2nd portion of the duodenum by the annular pancreas.
Axial CECT shows pancreatic tissue completely encircling the 2nd part of the duodenum , characteristic of an annular pancreas.
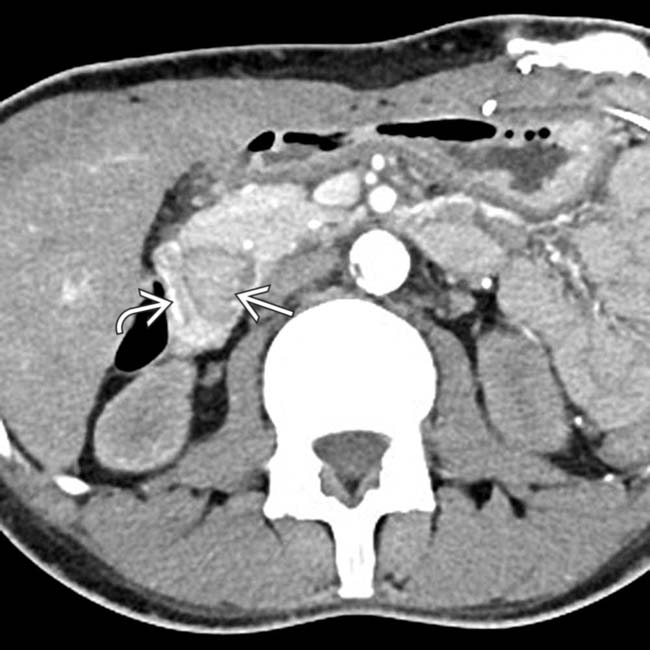
Axial CECT demonstrates pancreatic head tissue encircling the duodenum . Note the infiltrated mesentery due to pancreatitis related to the annular pancreas.
ERCP shows a portion of the annular pancreatic duct that has a beaded appearance due to chronic pancreatitis.
Axial CECT demonstrates pancreas tissue encircling the duodenum , a characteristic CT appearance of an annular pancreas.
Axial CECT demonstrates a thin sliver of pancreatic tissue wrapping around the duodenum , characteristic of an annular pancreas. Annular pancreas is asymptomatic in most adult patients.
Axial CECT shows the 2nd portion of the duodenum completely encircled by pancreatic tissue , a classic appearance for an annular pancreas. The duodenal lumen is not significantly narrowed.
Axial gadolinium-enhanced MR demonstrates a thin rim of pancreatic tissue lateral to the second duodenum . There is no significant narrowing of the duodenum and the patient was asymptomatic. Note that the thin rim of pancreatic tissue lateral to the duodenum enhances the same as the rest of the pancreatic head tissue.
Axial CECT shows the duodenum completely encircled by otherwise normal-appearing pancreatic tissue. The duodenal lumen is mildly narrowed, but this patient was asymptomatic.
Axial CECT demonstrates pancreatic tissue encircling the duodenum, in keeping with an annular pancreas.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Incomplete annular pancreas: Pancreatic tissue may extend anterolateral or posterolateral to duodenum or anterior and posterior to duodenum (“crocodile-jaw” configuration)
• MR: Normal pancreatic tissue (with identical signal to normal pancreas) encircling duodenum
MRCP: Main pancreatic duct encircling duodenum (and abnormally extending to right side of duodenum)
Secretin dilates duct and facilitates diagnosis
• Fluoroscopic barium study (upper GI): Extrinsic smooth compression and narrowing of 2nd part of duodenum
• ERCP: Duct draining pancreatic head encircles the duodenum and joins normal main pancreatic duct
TOP DIFFERENTIAL DIAGNOSES
• Duodenal carcinoma
• Pancreatic ductal carcinoma
• Postbulbar peptic ulcer
• Multiple other causes of duodenal stenosis
PATHOLOGY
• Etiology: Incomplete rotation of ventral anlage leads to pancreatic tissue encircling 2nd part of duodenum
Other congenital anomalies in up to 75% of pediatric cases (Down syndrome, duodenal atresia, etc.)
CLINICAL ISSUES
• 50% of cases present in infancy due to gastric outlet obstruction
• Most adults asymptomatic, but rare symptoms include gastric obstruction, upper GI bleeding, and jaundice
Rare symptoms include partial gastric outlet obstruction, upper GI bleeding, abdominal pain, and obstructive jaundice
• Associated in adults with gastric/duodenal ulcers and pancreatitis; questionable link with pancreatic cancer
Buy Membership for Radiology Category to continue reading. Learn more here




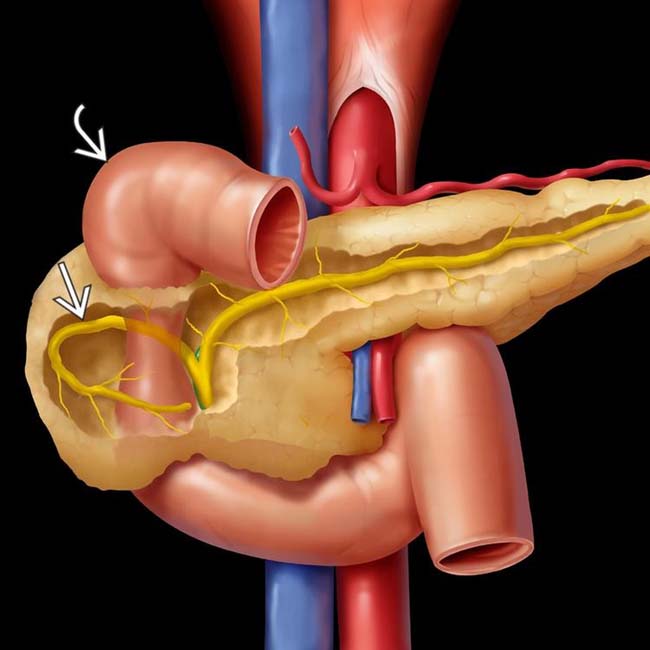
 also encircles the descending duodenum. Note the proximal duodenal dilatation
also encircles the descending duodenum. Note the proximal duodenal dilatation  .
.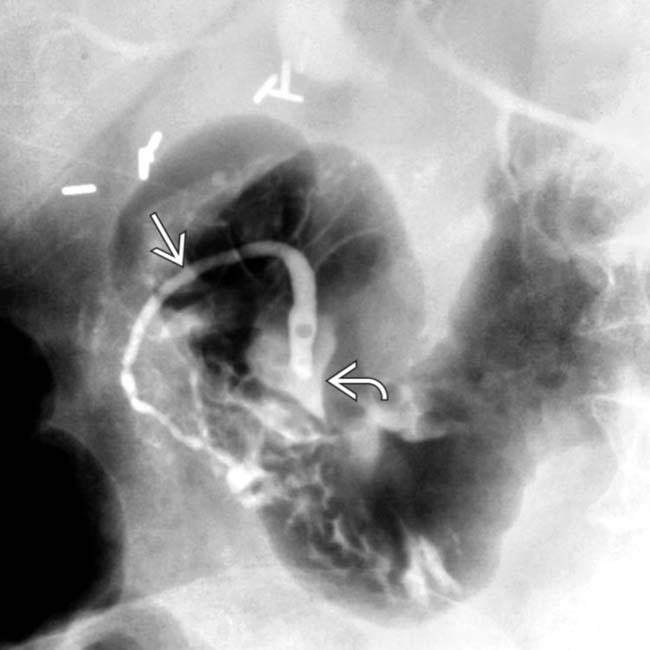
 originating on the right anterior surface of the duodenum, encircling it, and emptying into the main pancreatic duct near the ampulla
originating on the right anterior surface of the duodenum, encircling it, and emptying into the main pancreatic duct near the ampulla  .
.
 completely encircling the duodenum
completely encircling the duodenum  . Notice the different enhancement of the pancreatic tissue and the duodenal wall.
. Notice the different enhancement of the pancreatic tissue and the duodenal wall.
 is narrowed by pancreatic tissue
is narrowed by pancreatic tissue  both anteriorly and posteriorly. While adults with annular pancreas are usually asymptomatic, this patient was experiencing intermittent obstruction and early satiety.
both anteriorly and posteriorly. While adults with annular pancreas are usually asymptomatic, this patient was experiencing intermittent obstruction and early satiety.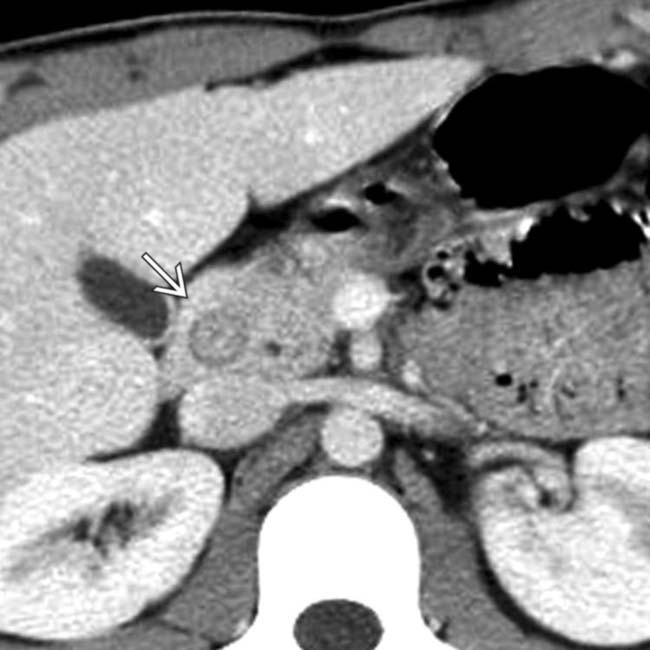
 .
.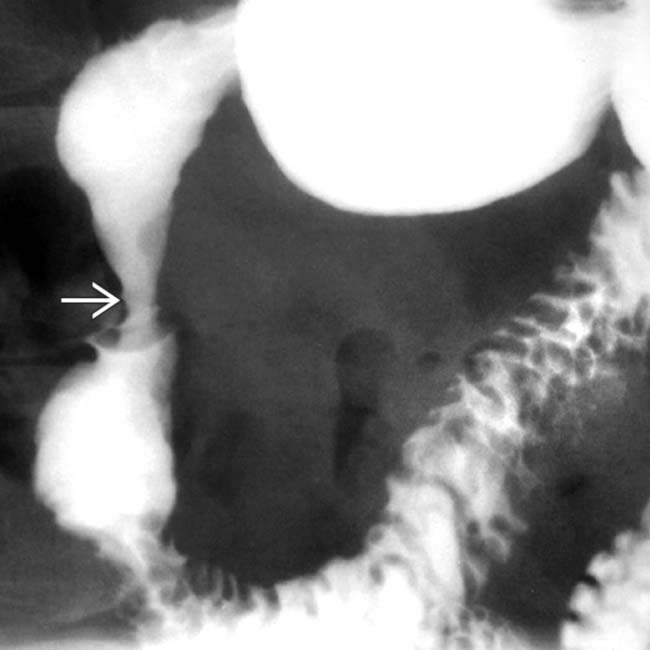
 of the lumen of the 2nd portion of the duodenum by the annular pancreas.
of the lumen of the 2nd portion of the duodenum by the annular pancreas.
 completely encircling the 2nd part of the duodenum
completely encircling the 2nd part of the duodenum  , characteristic of an annular pancreas.
, characteristic of an annular pancreas.
 encircling the duodenum
encircling the duodenum  . Note the infiltrated mesentery due to pancreatitis related to the annular pancreas.
. Note the infiltrated mesentery due to pancreatitis related to the annular pancreas.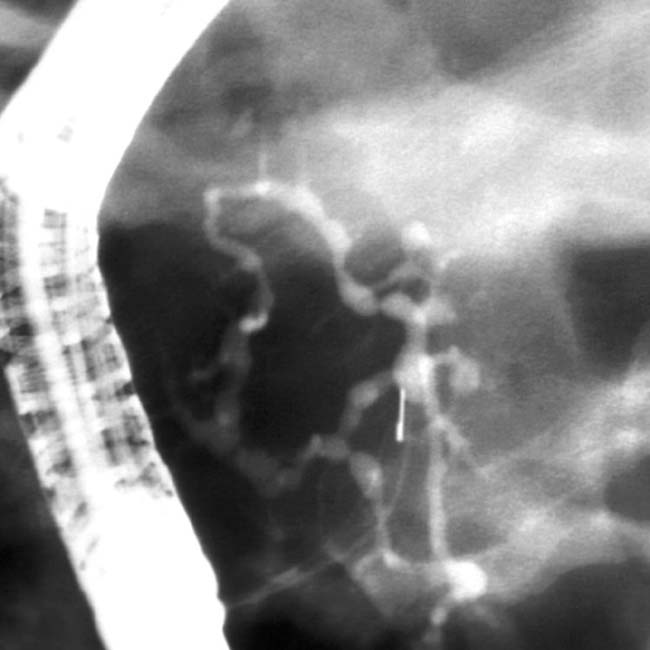
 encircling the duodenum
encircling the duodenum  , a characteristic CT appearance of an annular pancreas.
, a characteristic CT appearance of an annular pancreas.
 wrapping around the duodenum
wrapping around the duodenum  , characteristic of an annular pancreas. Annular pancreas is asymptomatic in most adult patients.
, characteristic of an annular pancreas. Annular pancreas is asymptomatic in most adult patients.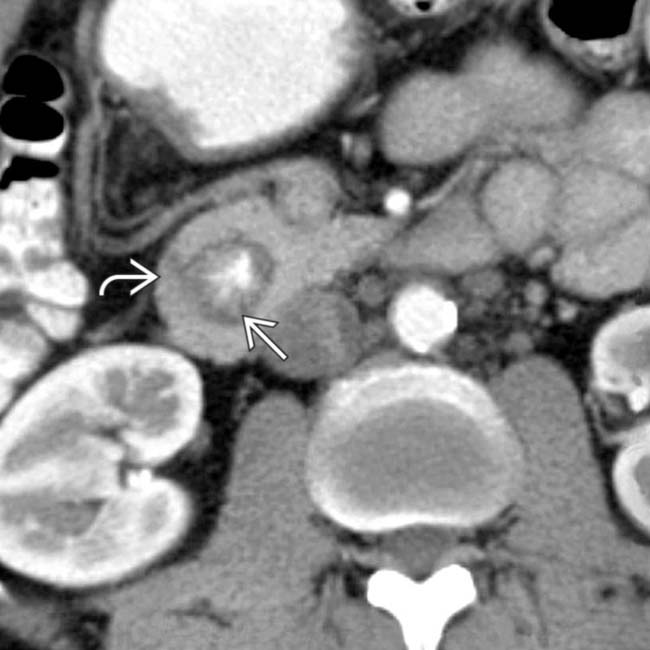
 completely encircled by pancreatic tissue
completely encircled by pancreatic tissue  , a classic appearance for an annular pancreas. The duodenal lumen is not significantly narrowed.
, a classic appearance for an annular pancreas. The duodenal lumen is not significantly narrowed.
 lateral to the second duodenum
lateral to the second duodenum  . There is no significant narrowing of the duodenum and the patient was asymptomatic. Note that the thin rim of pancreatic tissue lateral to the duodenum enhances the same as the rest of the pancreatic head tissue.
. There is no significant narrowing of the duodenum and the patient was asymptomatic. Note that the thin rim of pancreatic tissue lateral to the duodenum enhances the same as the rest of the pancreatic head tissue.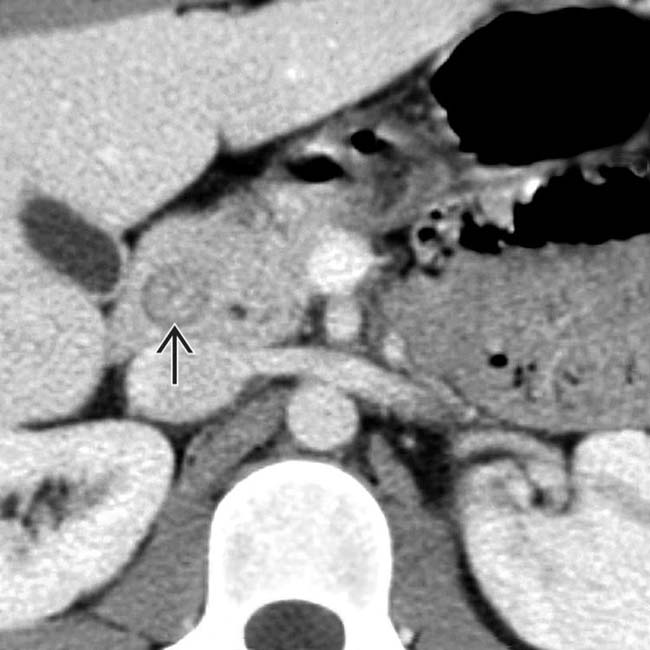
 completely encircled by otherwise normal-appearing pancreatic tissue. The duodenal lumen is mildly narrowed, but this patient was asymptomatic.
completely encircled by otherwise normal-appearing pancreatic tissue. The duodenal lumen is mildly narrowed, but this patient was asymptomatic.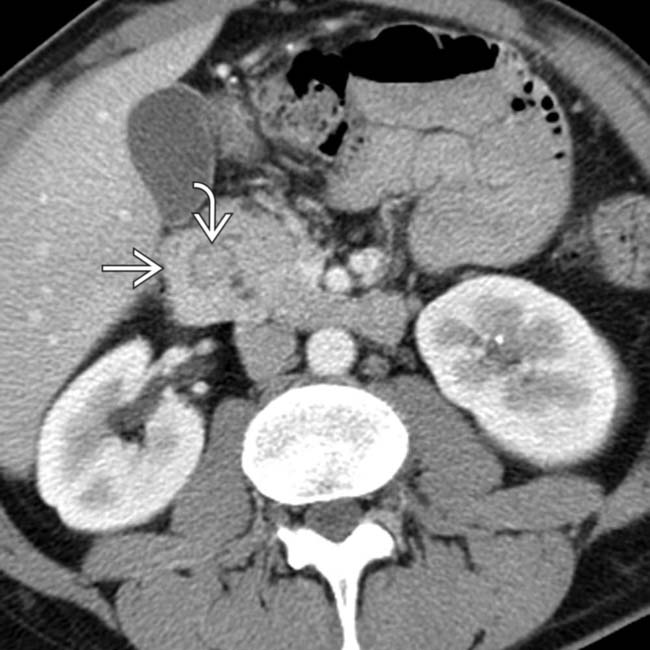
 encircling the duodenum, in keeping with an annular pancreas.
encircling the duodenum, in keeping with an annular pancreas.