Applied anatomy of the shoulder girdle

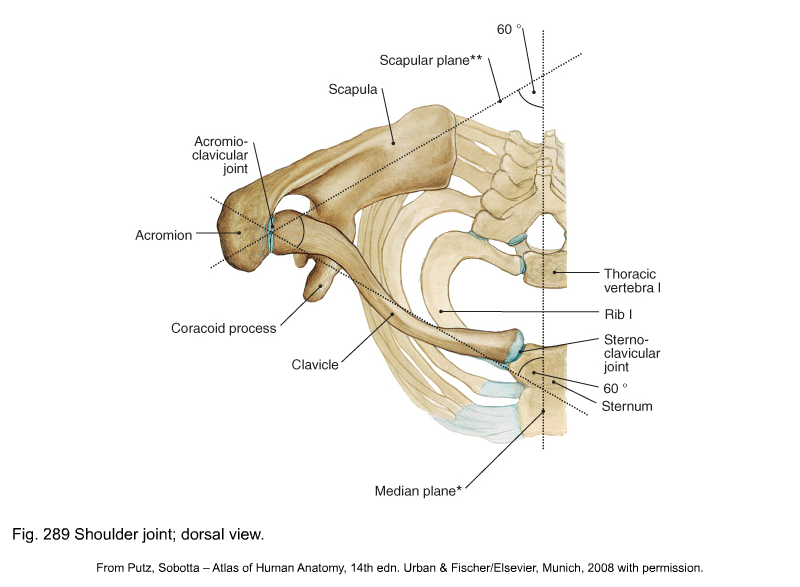
The shoulder girdle forms the connection between the spine, the thorax and the upper limb. It contains three primary articulations, all directly related to the scapula: the acromioclavicular joint, the sternoclavicular joint and the scapulothoracic gliding surface (see Putz, Fig. 289). The shoulder girdle acts as a unit: it cannot be functionally separated from the secondary articulations, i.e. the lower cervical spine, the cervicothoracic junction and the upper thoracic spine, to which it is connected via the costovertebral joints.
Osteoligamentous structures
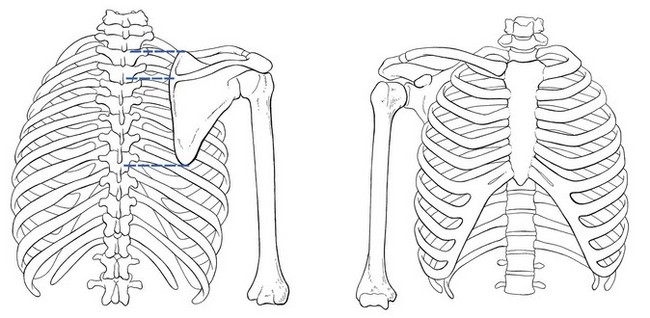
The clavicle articulates at the medial aspect with the sternum – the sternoclavicular joint – and at the lateral aspect with the acromion to form the acromioclavicular joint. In this way it connects the scapula to the trunk (Fig. 1).
Acromioclavicular joint
The rather flat articular surface at the lateral end of the clavicle articulates with the flat articular surface at the medial border of the acromion. The joint has a capsule which is reinforced by ligaments: cranially the superior acromioclavicular ligament and caudally the inferior one. The joint often contains an intra-articular disc, which is sometimes incomplete (meniscoid) and is subject to early degeneration. The joint line runs obliquely, from craniolateral to caudomedial (Fig. 2).
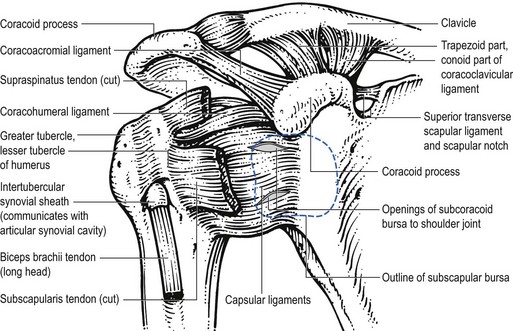
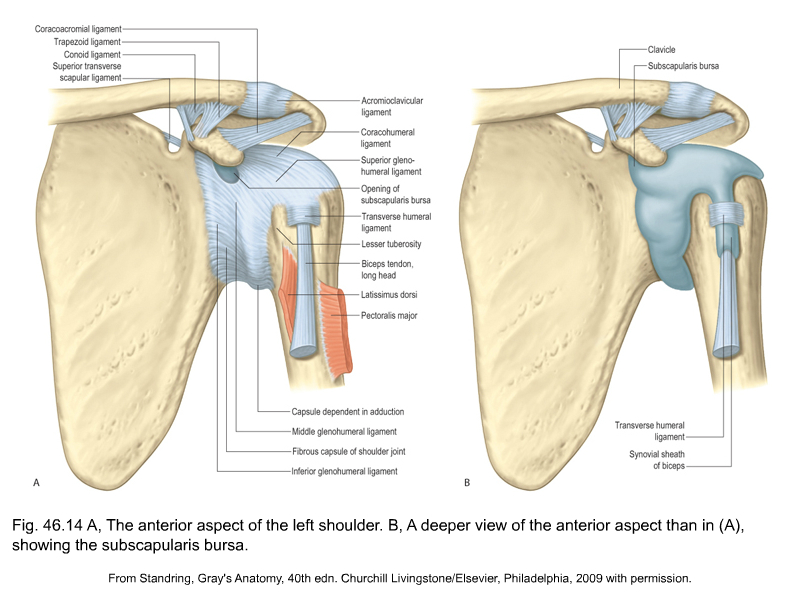
Extra-articular ligaments are important for the stability of the joint and to keep the movements of the lateral end of the clavicle within a certain range. Together they form the roof of the shoulder joint (see Standring, Fig. 46.14). They are the coracoacromial ligament – between the lateral border of the coracoid process and the acromion – and the coracoclavicular ligament. The latter consists of:
• The trapezoid ligament which runs from the medial border of the coracoid process to the trapezoid line at the inferior part of the lateral end of the clavicle.
• The conoid ligament which is spanned between the base of the coracoid process and the conoid tubercle just medial to the trapezoid line.
Movements in the acromioclavicular joint are directly related to those in the sternoclavicular joint and those of the scapula. This joint is also discussed inthe online chapter Applied anatomy of the shoulder.
Sternoclavicular joint
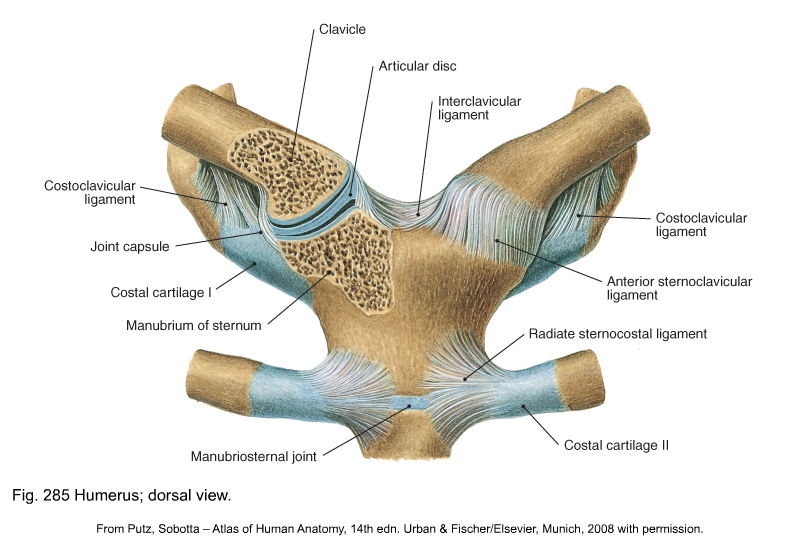
The sternoclavicular joint is more complex. It is formed by the articular surface at the medial aspect of the clavicle and the articular surface at the superolateral corner of the sternal manubrium. The two joint surfaces are discongruent and this is resolved by the presence of an intra-articular disc, which divides the joint into two cavities. The rather loose joint capsule is reinforced by anterior and posterior sternoclavicular ligaments. There are two extracapsular ligaments: the interclavicular ligament, which interconnects both clavicles and covers the jugular notch, and the costoclavicular ligament, between the sternal end of the first rib and the medial part of the clavicle (see Putz, Fig. 285).
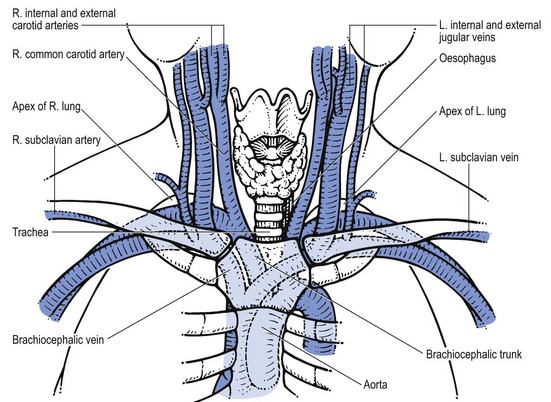
Close behind the joint lie some vital structures: some important blood vessels (aorta, brachiocephalic trunk, brachiocephalic vein, subclavian artery, subclavian vein, jugular vein and carotid artery), the trachea, the oesophagus, the lung and pleura (Fig. 3).
Movements in the sternoclavicular joint are possible around three axes:
• Clavicular elevation and depression occur around an anteroposterior axis
• Clavicular protraction – the lateral end of the clavicle moves forwards, and retraction – the lateral end of the clavicle moves backwards, around a vertical axis
• Backwards and forwards rotation of the clavicle around its longitudinal axis.
Glenohumeral and scapular movements also mobilize the clavicle and thus influence the sternoclavicular joint. Diminution of the mobility of the clavicle will have direct consequences for the joints with which it articulates – sternoclavicular and acromioclavicular – and indirectly for the glenohumeral joint.
Scapulothoracic gliding mechanism
The scapulothoracic gliding mechanism is a ‘virtual articulation’ indicating that the scapula is mobile in relation to the thorax.
The gliding surfaces are formed by the anterior aspect of the scapula and the posterior aspect of the thorax. In between the scapula and the thorax lie the subscapular and the serratus anterior muscles (see below). Together with their fasciae they take part in the gliding mechanisms that occur during movement.
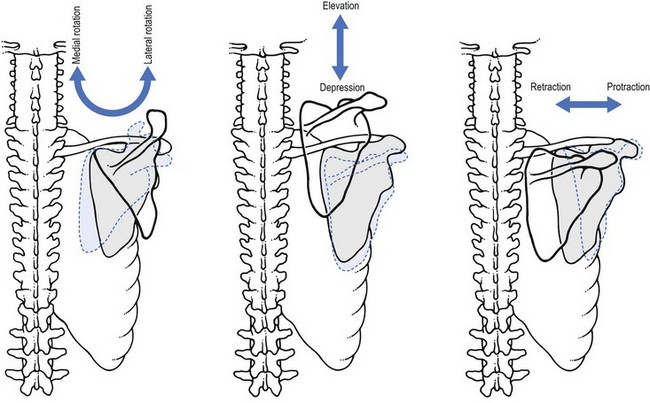
The scapula moves in three directions:
• Up and down (elevation and depression, respectively) when the lateral end of the clavicle does the same. The medial border of the scapula remains more or less parallel to the spine.
• Lateral and medial rotation – the inferior angle moves laterally and medially. These movements are mainly induced by movements of the arm towards abduction/elevation and extension.
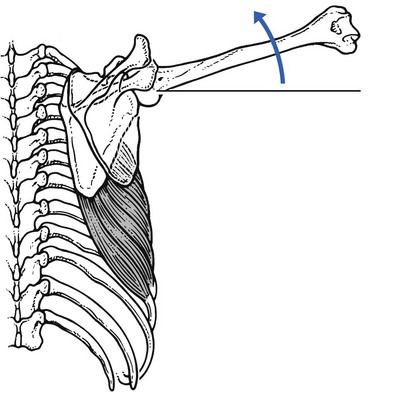
• It glides laterally and medially – protraction and retraction or approximation – when the lateral end of the clavicle does the same. The scapula glides away from the spine but its medial border remains parallel to the spine (Fig. 4).
Costovertebral joints
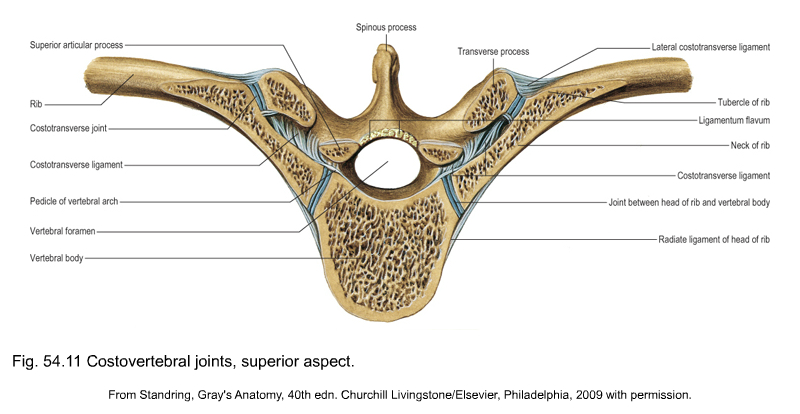
The ribs articulate with the thoracic spine at two levels (see Standring, Fig. 54.11):
• At the vertebral body – the costovertebral joint: the head of the rib articulates with the lateral aspect of one or two vertebral bodies. The joint capsule is reinforced by the radiate ligament of the joint at the head of the rib. Intra-articularly the head of the rib is connected to the intervertebral disc by the intra-articular ligament of the joint at the head of the rib.
• At the transverse process – the costotransverse joint: the tubercle of the rib articulates with the articular facet on the transverse process of the vertebra. The joint capsule is again reinforced by several ligaments: costotransverse ligament – between the neck of the rib and the transverse process; lateral costotransverse ligament – between the angle of the rib and the tip of the transverse process; and the superior costotransverse ligament – between the crest of the neck of the rib and the inferior border of the transverse process of the vertebra above (Fig. 5).
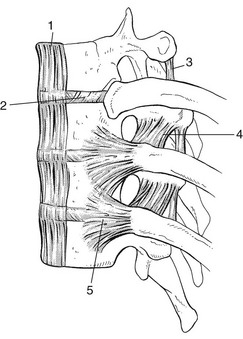
Fig 5 The costovertebral joints. (1) anterior longitudinal ligament; (2) disc; (3) costotransverse ligament; (4) superior costotransverse ligament; (5) radiate ligament.
Muscles and their innervation
Those muscles that create movement at the acromioclavicular joint, the sternoclavicular joint or in the scapulothoracic gliding mechanism, or those muscles that connect the scapula to the trunk, can be considered as ‘shoulder girdle musculature’. Many of these muscles also have influence on the secondary articulations: the cervical spine, the shoulder or the thoracic spine and are discussed in the online chapters Applied anatomy of the cervical spine, Applied anatomy of the shoulder, and Applied anatomy of the thorax and abdomen respectively. In this chapter only those muscles that are not discussed elsewhere are described.
Anterior aspect of the shoulder girdle
The muscles at the anterior aspect of the shoulder girdle are outlined in Table 1 and Figure 6.
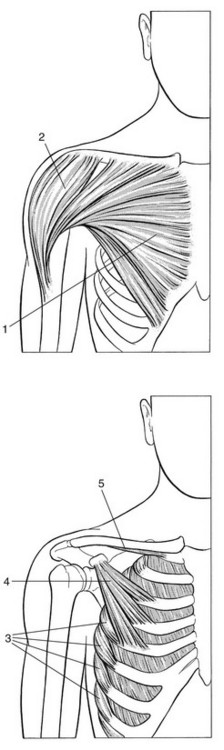
Fig 6 Anterior muscles of the shoulder girdle. (1) pectoralis major; (2) deltoid; (3) serratus anterior; (4) pectoralis minor; (5) subclavius.
Table 1
Anterior muscles of the shoulder girdle
| Muscle | Nerve | Spinal nerve root |
| Sternocleidomastoid | Spinal accessory and cervical plexus | C1–C2 |
| Subclavius | Nerve to subclavius | C5–C6 |
| Pectoralis minor | Pectoral nerves | C6–C8 |
| Pectoralis major | Pectoral nerves | C5–T1 |
| Deltoid | Axillary nerve | C4–C6 |
| Pectoral part | Pectoral rami | C4–C5 |
| Biceps brachii | Musculocutaneous nerve | C5–C6 |
| Coracobrachialis | Musculocutaneous nerve | C6–C7 |
Sternocleidomastoid muscle
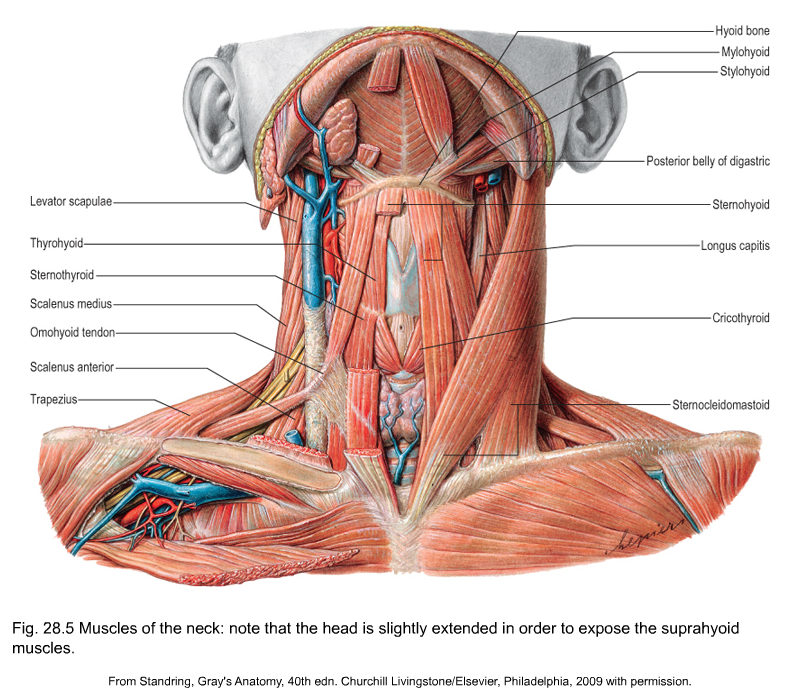
The sternocleidomastoid muscle originates with two heads, one from the manubrium of the sternum and one from the medial end of the clavicle (see Standring, Fig. 28.5). It inserts at the mastoid process and the superior nuchal line. Contraction of the muscle puts stress onto the sternoclavicular joint.
Subclavius muscle
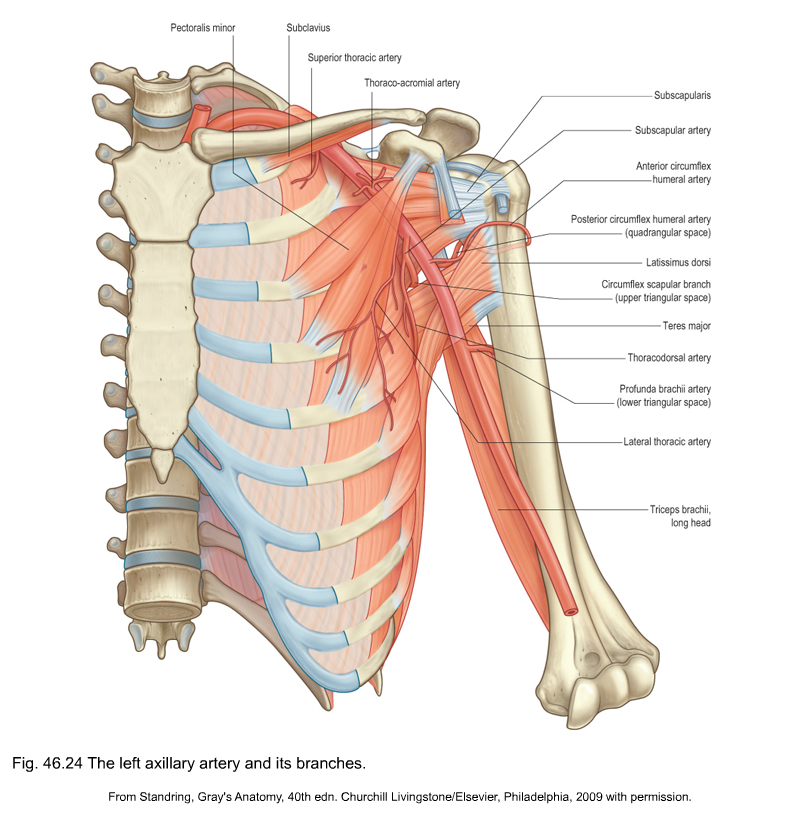
The subclavius takes origin at the junction between the bone and the cartilage at the sternal end of the first rib (see Standring, Fig. 46.24). It inserts at the inferior and lateral aspect of the clavicle. It pulls the clavicle against the sternum and has a stabilizing effect on the sternoclavicular joint.
Pectoralis minor muscle
The pectoralis minor muscle takes origin anteriorly at the third to fifth ribs and inserts at the inferior and medial border of the coracoid process (see Standring, Fig. 46.24). Its contraction results in a depression and protraction of the scapula.
Posterior aspect of the shoulder girdle
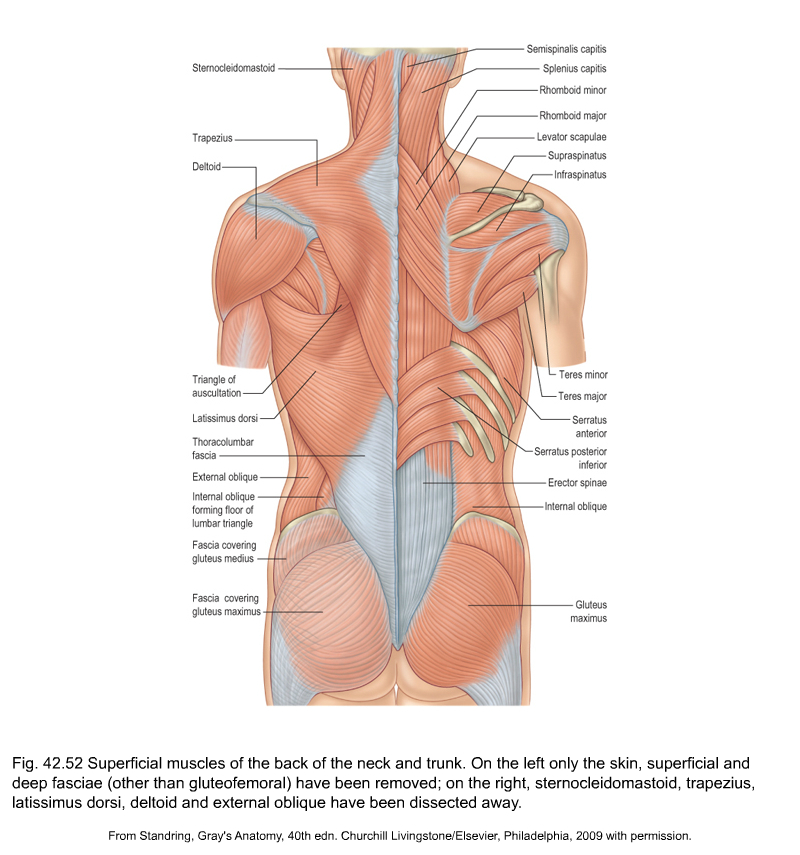
The muscles at the posterior aspect of the shoulder girdle are outlined in Table 2 and Figure 7 and see Standring, Fig 42.52.
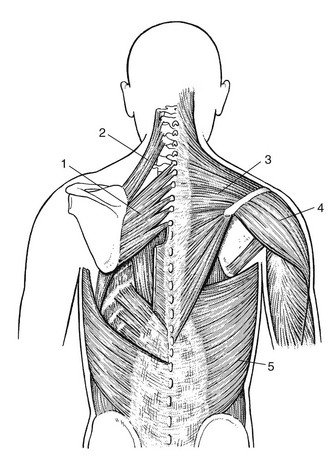
Fig 7 Posterior muscles of the shoulder girdle. (1) Rhomboids; (2) levator scapulae; (3) trapezius; (4) deltoid; (5) latissimus dorsi.
Table 2
Posterior muscles of the shoulder girdle
| Muscle | Nerve | Spinal nerve root |
| Trapezius | Spinal accessory nerve | C2–C4 |
| Levator scapulae | Dorsal scapular nerve | C4–C5 |
| Rhomboids | Dorsal scapular nerve | C4–C5 |
| Serratus anterior | Long thoracic nerve | C5–C7 |
| Latissimus dorsi | Thoracodorsal nerve | C6–C8 |
| Teres major | Thoracodorsal nerve | C6–C7 |
| Subscapularis | Subscapular nerve | C5–C8 |
| Infraspinatus | Suprascapular nerve | C4–C6 |
| Teres minor | Axillary nerve | C5–C6 |
| Supraspinatus | Suprascapular nerve | C4–C6 |
| Deltoid | Axillary nerve | C4–C6 |
| Triceps brachii | Radial nerve | C6–C8 |
Levator scapulae muscle
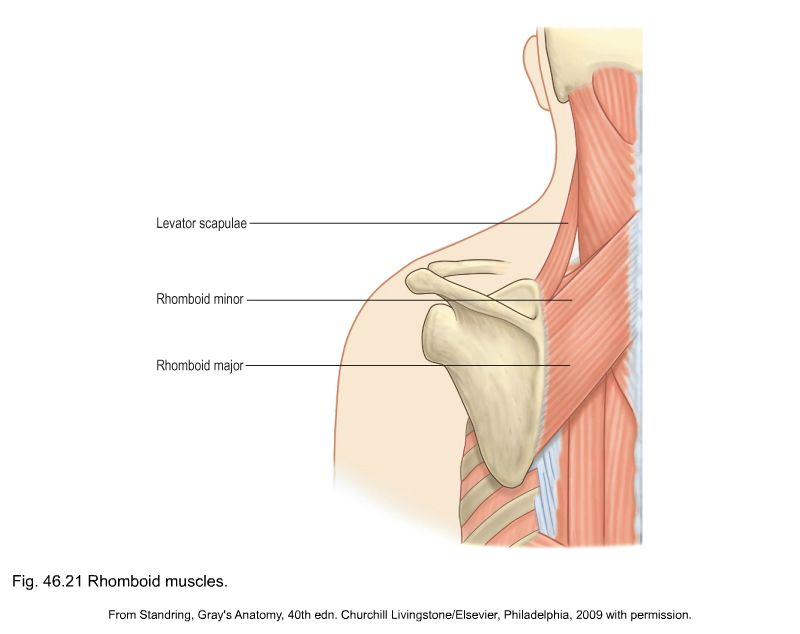
The levator scapulae takes origin at the posterior tubercles of the transverse processes of the first to fourth cervical vertebrae and inserts at the superior angle and superior part of the medial border of the scapula (see Standring, Fig. 46.21). It elevates and medially rotates the scapula.
Serratus anterior muscle
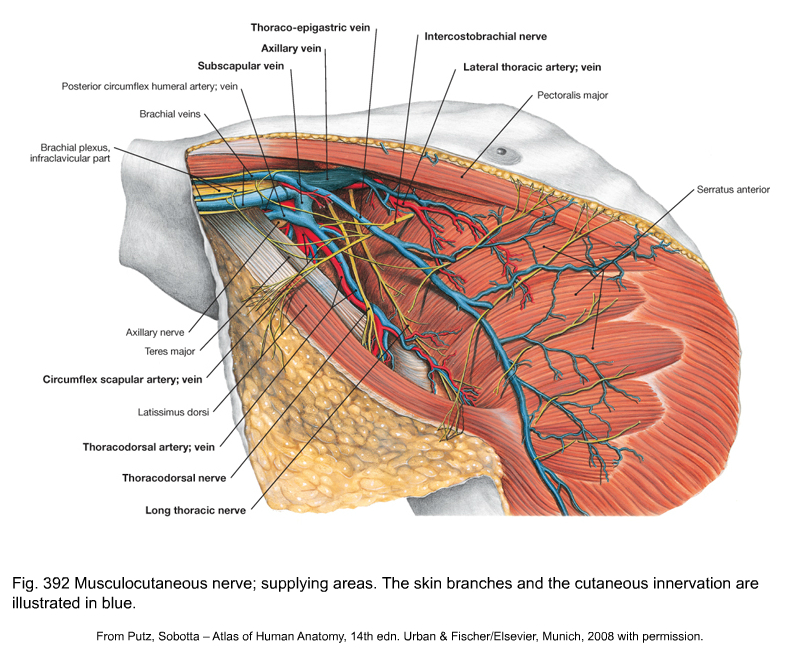
The serratus anterior has origin with nine or ten heads at the lateral aspect of the first to eighth or ninth ribs and inserts along the entire medial border of the scapula, from the superior to the inferior angle (see Putz, Fig. 392). Three different parts are recognized: superior, medial and inferior. It fixates the scapula against the thorax and moves the scapula towards protraction and lateral rotation. The muscle is innervated by the nervus thoracicus longus.
Mobility of the shoulder girdle
Mobility in the shoulder girdle depends on the mobility of the primary joints – acromioclavicular, sternoclavicular and scapulothoracic gliding mechanism. It can only be maximal when the secondary articulations also function normally.
The movements that occur when the shoulder is moved and that can be assessed in shoulder girdle examination are:
• Elevation: the shoulder moves upwards in the frontal plane. The range is approximately 30–45°.
• Depression: the shoulder moves downwards in the frontal plane. The range is about 5°.
• Protraction: the shoulder moves forwards in a transverse plane with a range of up to 30°.
• Retraction: the shoulder moves backwards in a transverse plane. The range is about 30°. This movement is also referred to as ‘scapular approximation’.
Anterior and posterior rotation of the clavicle cannot be examined separately. It is the result of arm movements towards flexion or elevation and extension (Fig. 8).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}