Applied anatomy of the sacroiliac joint

The joint
The sacroiliac joint possesses all the characteristics of a true joint: a joint cavity containing synovial fluid,1 adjacent bones having ligamentous connections, cartilaginous surfaces which permit movements and an outer fibrous joint capsule with an inner synovial lining.2–5
The joint most commonly links the posterosuperior part of the medial aspect of the iliac bones with the first, second and the upper part of the third segment of the sacrum (Fig. 1). A transverse section shows that the joint is situated rather anteriorly (Fig. 2). The clinical consequence of this is that it is not possible to elicit tenderness by digital pressure at the joint.
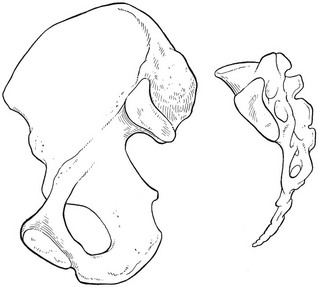
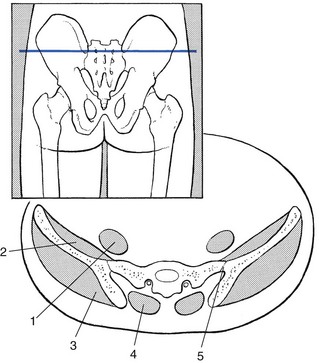
Fig 2 Transverse section at the level of the sacroiliac joint: 1, psoas; 2, iliacus; 3, gluteus; 4, erector spinae; 5, sacroiliac joint.
The sacrum can be regarded as a wedge that fits vertically between the two iliac bones. The sacrum also fits between these bones in the transversal plane.6
The dorsal width of the sacrum exceeds the ventral width only in the middle portion of the joint (see Fig. 4c). At the lower and upper parts, the wedge shape is quite reversed (see Fig. 2). Several investigators, however, have demonstrated a high degree of variability in the plane of sacroiliac joints, in both the vertical and transverse directions.1,7,8
The articular surfaces are ear- or C-shaped and exhibit irregular ridges and depressions that fit into each other.9,10 The anatomical configuration, together with strong ligaments, make the joint very stable. These features are more pronounced in men than in women, suggesting the likelihood of increased mobility in the latter. Some authors also associate this increased mobility with the position of the centre of gravity, which in women lies dorsal to the hip joint and not in line with the axis of support (Fig. 3). This exerts a strong rotational force in the sacroiliac joint.11,12
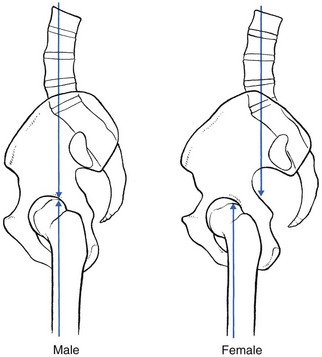
Fig 3 Differences between the position of the centre of gravity in the male and female. The position of the centre of gravity lies in line with the axis of the support (male), or lies dorsally (female).
Cartilage covers the joint surfaces. It is thicker and smoother at the sacral than at the iliac surface.5
Joint capsule and ligaments
A tight articular capsule is attached close to the margins of the articular surfaces of the ilium and sacrum.
Powerful ligaments support the joint and sharply limit movements (Fig. 4). These ligaments can be divided into the massive interosseous sacroiliac ligament, the posterior and anterior ligaments, and three accessory ligaments – the sacrotuberous, sacrospinous and iliolumbar ligaments.
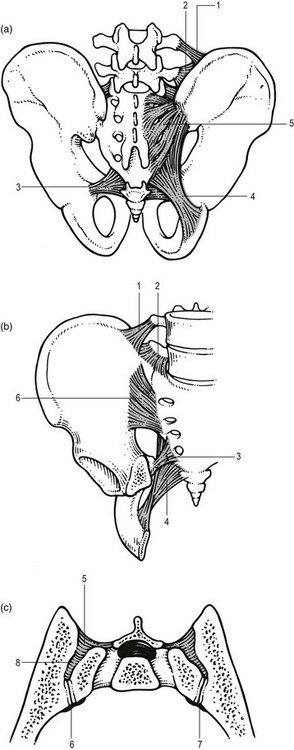
Fig 4 (a) Posterior and (b) anterior aspect. 1, 2, superior and inferior bands of iliolumbar ligaments; 3, sacrospinous ligament; 4, sacrotuberous ligament; 5, posterior sacroiliac ligaments; 6, anterior sacroiliac ligaments. (c) Transection through the sacroiliac joint: 7, sacroiliac joint; 8, interosseous ligament.
The interosseous ligament fills the irregular space between sacrum and ilium at the level of S1 and S2, immediately behind and above the joint. The shortest and strongest part of this ligament is in the frontal, horizontal axis of movement of the sacrum and it is therefore also known as the axial ligament.
The strong posterior sacroiliac ligament consists of several fascicles of different lengths which overlie the interosseus ligament and pass in an oblique direction from the lateral crests of the sacrum to the posterior superior iliac spine and the posterior end of the inner lip of the iliac crest. Those fibres from the third and fourth sacral segments are longer and constitute the long posterior sacroiliac ligaments.13
The thin anterior sacroiliac ligament consists of two bands which reinforce the anterior and inferior parts of the fibrous capsule and also pass across the joint obliquely from sacrum to ilium.
The sacrotuberous ligament is attached to the posterior iliac spines, the lower part of the sacrum and the upper part of the coccyx. Its fibres run obliquely downwards and laterally to insert at the medial margin of the ischial tuberosity. The gluteus maximus, the thoracolumbar fascia, the multifidus muscle and, in some individuals (especially females), long head of biceps femoris are partly attached to this ligament.
The thin triangular sacrospinous ligament attaches to the lateral margins of sacrum and coccyx in front of the attachments of the sacrotuberous ligament. The fibres run in a lateral, caudal and anterior direction to insert at the spine of the ilium.
The iliolumbar ligament takes origin at the lower part of the transverse processes of the fourth and particularly the fifth lumbar vertebrae. Its fibres radiate to the anterior part of the upper surface of the sacrum as well as to the crest of the ilium.
Muscles
The sacroiliac joint is surrounded by some of the largest and most powerful muscles of the body, i.e. the erector spinae, psoas, quadratus lumborum, piriformis, abdominal obliques, gluteal and hamstrings. However, there are no muscles designed to act on the sacroiliac joint to produce active, physiological movements. All muscles that cross the joint are designed to act on the hip or the lumbar spine.1,2,14–16 None of the small movements of the sacroiliac joint is produced by active movements of the sacrum. The movements are indirectly imposed by gravity and muscles acting on trunk and lower limbs.
Whether these muscles could contribute to active stability of the joint (force closure) is still open to debate. Some authors suggest that the latissimus dorsi and the contralateral gluteus maximus are coupled via the thoracolumbar fascia. The forces of these two synergists cross the sacroiliac joints perpendicularly and it is hypothesised that this could stabilize the joint indirectly.17–20
Innervation
No authoritative anatomical studies exist today but most authors report a posterior innervation from the lateral branches of the posterior rami L4–S3 and an anterior innervation from the L2–L3 segments.21
The fact that capsule and ligaments contain nociceptors suggests that the sacroiliac joint is a possible source of low back pain and also plays a role in somatic referred pain.22
The wide range of segmental innervation probably accounts for the variable referred pain patterns seen in sacroiliac joint lesions,1,23 although pain is localized most commonly at the buttock and the posterior thigh.
Biomechanical aspects
In essence the sacroiliac joint is a stress-relieving joint that serves as a buffer between the lumbosacral and hip joint.10 The sacroiliac joint transmits forces from the vertebral column sideways into the pelvis and then to the lower limbs. Conversely, forces from the lower limbs can be transmitted through pelvis and sacrum to the vertebral column. Despite its size, the sacroiliac joint cannot be considered the same as any other major joint of the body: its ranges of movement (nutation–counternutation, more complex movements and pelvic torsion) are very small and are not controlled by active muscular contractions.
The precise nature of motion in the normal joint is still unclear and joints such as the sacroiliac joint with extensive ridges and depressions can be expected to have a very limited amount of mobility. In Kapandji’s words: ‘There is more a tendency to movement than actual movement since the extremely powerful ligaments preclude any movement from the start’.6
Both in vivo and in vitro kinematic studies have demonstrated various types of minor motion in the sacroiliac joints, such as gliding, rotation, tilting, nodding and translation.24–26 Mobility is always increased temporarily at the end of pregnancy and for up to 3 months afterwards.15,27,28 It decreases in men at between 40 and 50 years, and after the age of 50 in women.29
Nutation–counternutation
Most authors1,15,30–33 accept that there is a small rotatory movement about a frontal, horizontal axis at the level of S1–S2, constituted by the shortest and strongest part of the interosseous (‘axial’) ligament.
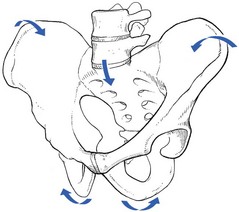
During anterior rotation, called nutation, the promontory of the sacrum moves inferiorly and anteriorly while the apex of the sacrum and the coccyx move posteriorly (Fig. 5a). As a result of the converging planes of the sacral joint surfaces, the iliac bones are approximated, whereas the ischial tuberosities move apart (Fig. 6). This movement also results in slight distraction of the symphysis pubis. Nutation is limited by the tension of the anterior sacroiliac ligament, the interosseus ligament, the short upper part of the posterior sacroiliac ligament and the sacrospinous and sacrotuberous ligaments.
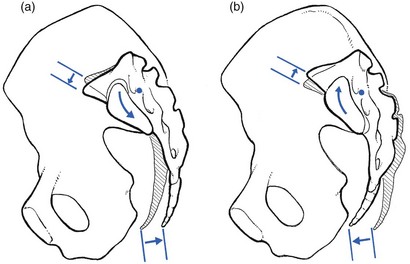
During counternutation (posterior rotation), the promontory of the sacrum moves superiorly and posteriorly while the apex and the coccyx move anteriorly (Fig. 5b). As a result, the iliac bones move apart, whereas the ischial tuberosities are approximated. Counternutation is limited by the tension of the posterior sacroiliac ligaments, especially the long part of these ligaments.6
Weisl30 showed that the length of the anterior–posterior diameter of the superior aperture of the pelvis changed by 5–6 mm during combined nutation–counternutation. This mobility pattern has been confirmed in women.34
More complex movements
Radiological stereophotogrammetrical analysis35 has identified very small movements in the sacroiliac joints. In changing position from supine to standing or sitting and between standing and hyperextension of the leg, the movements proved even to be three-dimensional, although again most constant around the frontal, horizontal axis. The mean values obtained were: 2.5°, translation 0.7 mm.
In a recent study of sacroiliac kinematics for reciprocal straddle positions in relatively young subjects, it was established that the pelvis showed a tendency to move in three directions – flexion–extension, side flexion and rotation.36 Another study, using rigidly fixed external devices in 21 volunteers, examined the range of motion of the sacroiliac joint during maximal flexion and extension of the trunk and during standing on one leg. The conclusion was that there was a small range of movement (less than 1°) but with an irregular direction – during flexion of the trunk, the sacrum was just as likely to flex as to extend around a transverse axis. Consequently, in a sample of individuals and for one particular test, the true range of motion of the sacroiliac joint is 0°.37
Torsion of the pelvis
Cramer discusses more complex movements.38 During walking (Fig. 7), when a person lifts one leg and puts the entire body weight on the other leg, the load of the trunk moves the sacrum forward and caudally but also causes forward rotation. The ilium on the weight-bearing side is pushed cranially and rotates dorsally and externally. On the non-weight-bearing side, the movement of the sacrum is dorsal and cranial, with posterior rotation; on this side the ilium slides caudally and rotates forward in relation to the sacrum. Overall, the movements of the iliac are torsional. This mobility of the sacroiliac joints incontrovertibly relieves part of the strain on the lumbar spine and is therefore clearly beneficial.
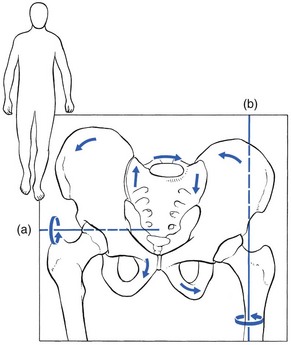
Fig 7 Complex movements of the iliac bones and sacrum during walking (from Cramer A38, with permission). (a) Rotation of the iliac bone at the non-weight-bearing side, around a frontal, horizontal axis. (b) Rotation of the iliac bone at the weight-bearing side around a vertical axis.
It has been conjectured that jumping from a height or stepping onto a high stool increases these complex movements and perhaps even subluxates the joint. Vleeming et al39,40 have stated that:
Abnormal loading conditions could theoretically force the sacroiliac joint in a new position where ridges and depressions are no longer complementary. Such an abnormal joint position could be regarded as a blocked joint. Being part of the complex kinematic chain between legs and spine, even a small displacement of the sacrum or ilium could be responsible for abnormal displacement or stress of the lumbar vertebrae.
In the literature, however, they have found (as yet) no definite proof of this phenomenon. In the radiological stereophotogrammetrical analysis mentioned earlier, Sturesson et al35 also found that the mobility of symptomatic joints had a mean value equal to that of asymptomatic joints.
Mobility normally decreases with age, which is regularly shown on the radiograph in elderly patients with osteophytes at the lower margin of the joints or even bony ankylosis. In middle age the joint has already reduced in width and becomes obliterated by fibrous and fibrocartilagenous adhesions.4 In ankylosing spondylitis complete fusion is found even in young adults.
References
1. Solonen, KA, The sacroiliac joint in the light of anatomical, roentgenological and clinical studies. Acta Orthop Scand. 1957;27(suppl):1–127. 
2. Albee, FH. A study of the anatomy and the clinical importance of the sacro-iliac joint. JAMA. 1909; 53(16):1273–1276.
3. Gardner, E, Gray, DJ, O’Rahilly, R. Anatomy: A Regional Study of Human Structure, 4th ed. Philadelphia: Saunders; 1975.
4. Brooke, R, The sacro-iliac joint. J Anat 1924; 58:299–305. 
5. Sashin, DA. A critical analysis of the anatomy and pathological changes of the sacroiliac joints. J Bone Joint Surg. 1930; 12:891–910.
6. Kapandji, IA. The Physiology of the Joints, vol 3. Trunk and Vertebral Column, 2nd ed. New York: Churchill Livingstone; 1974.
7. Fischer, LP, Gonon, GP, Carret, JP, Dimmet, J. Biomecanique articulaire. Ass Corp Med. 1976; 2:33–36.
8. Bakland, O, Hansen, JH, The axial sacroiliac joint. Anat Clin 1984; 6:29–36. 
9. Vleeming, A, Stoeckaert, R, Volkers, ACW, Snijders, CJ, Relation between form and function in the sacro-iliac joint. Part I: Clinical anatomical aspects. Spine 1990; 15:130–132. 
10. Bowen, V, Cassidy, JD, Macroscopic anatomy of the sacro-iliac joint from embryonic life until the eighth decade. Spine 1981; 6:620–628. 
11. Tischauer, ER, Miller, M, Nathan, IM, Lordosimetry. A new technique for the measurement of postural response to materials handling. Am J Indust Hyg Ass 1973; 1:1–12. 
12. Bellamy, N, Park, W, Rooney, PJ, What do we know about the sacro-iliac joint? Semin Arthritis Rheum 1983; 12:282–313. 
13. Williams PL, ed. Gray’s Anatomy, 38th ed, Edinburgh: Churchill Livingstone, 1995.
14. Miller, JA, Schultz, AB, Andersson, GB, Load displacement behaviour of sacro-iliac joints. J Orthop Res 1987; 5:92–101. 
15. Colachis, SC, Warden, RE, Becthal, CO, et al, Movement of the sacro-iliac joint in the adult male. Arch Phys Med Rehabil 1963; 44:490–498. 
16. Bogduk, N. Clinical Anatomy of the Lumbar Spine and Sacrum. Edinburgh: Churchill Livingstone; 1997.
17. Snijders, CJ. Transfer of lumbosacral load to the iliac bones and legs. Part 2: Loading of the sacroiliac joints when lifting in stooped posture. J Clin Biomech. 1993; 8:295–301.
18. Snijders, CJ, Slagter, AHE, Van Strik, R, et al, Why leg crossing? The influence of common postures on abdominal muscle activity. Spine 1995; 20:1989–1993. 
19. Vleeming, A, Snijders, CJ, Stoeckaert, R, The posterior layer of the thoraco-lumbar fascia: its function in load transfer from spine to legs. Spine 1995; 20:753–758. 
20. Hodges, PW, Is there a role for transversus abdominis in lumbo-pelvic stability? Manual Therapy. 1999;4(2):74–86. 
21. Bernard, TN, Cassidy, JD. The sacroiliac joint syndrome. Pathophysiology, diagnosis and management. In: Frymoyer JW, ed. The Adult Spine: Principles and Practice. New York: Raven Press; 1991:2107–2130.
22. Oostendorp RAB, Elvers JWH, van Gool JJ, Clarijs JP. The sacro-iliac joint: its role in posture and dysfunction. Segmental signs of sacro-iliac joint dysfunction. First International Symposium on the Sacro-iliac Joint, Maastricht, 1991. ECO, PO Box 25327, Rotterdam, NL.
23. Bernard, TN, Cassidy, JD. The sacro-iliac joint syndrome: pathophysiology, diagnosis and management. In: Frymoyer JW, et al, eds. The Adult Spine: Principles and Practice. New York: Raven Press, 1991.
24. Beal, MC, The sacro-iliac problem: review of anatomy, mechanics and diagnosis. J Am Obstet Organ. 1982;81(10):667–679. 
25. Kim, LYS. Pelvic torsion, a common cause of low back pain. Orthop Rev. 1984; 13(4):206–211.
26. Lavignoll, B, An approach to the functional anatomy of the sacro-iliac joints in vivo. Anatomica Clinica 1983; 5:169–176. 
27. Clarke, WE. Legros: The Tissues of the Body: An Introduction to the Study of Anatomy. Oxford: Clarendon Press; 1952.
28. Lynch, FW. The pelvic articulation during pregnancy, labor and the puerperium. An X-ray study. Surg Gynecol Obstet. 1920; 30:575–580.
29. MacDonald, GR, Hunt, TE, Sacro-iliac joints: observation on the gross and histological changes in the various age groups. Canad Med Assoc J 1952; 66:157–163. 
30. Weisl, H, The movements of the sacro-iliac joint. Acta Anat 1955; 23:80–91. 
31. Duncan, JM. The behaviour of the pelvic articulations in the mechanism of parturition. Dublin Q J Med Sci. 1854; 18:60–69.
32. Egund, N, Olsson, TH, Schmid, H, Selvik, G, Movement in the sacroiliac joints demonstrated with roentgen stereophotogrammetry. Acta Radiol (Diagn) 1978; 19:833. 
33. Vleeming, A, Stoeckart, R, Snijders, CJ, et al. Mobility in the sacro-iliac joints in the elderly. A kinematic and roentgenologic study. Clin Biomech. 1992; 7:170–176.
34. Brunner, C, Kissling, R, Jacob, HAC, The effects of morphology and histopathologic findings on the mobility of the sacro-iliac joint. Spine. 1991;16(9):221–224. 
35. Sturesson, B, Selvik, G, Uden, A, Movements of the sacro-iliac joints. A roentgen stereophotogrammetric analysis. Spine 1969; 14:162–165. 
36. Smidt, GL, McQuade, K, Wei, SH, et al, Sacro-iliac kinematics for reciprocal straddle positions. Spine. 1995;20(9):1047–1054. 
37. Jacob, HAC, Kissling, RO, The mobility of the SI joints in healthy volunteers between 20 and 50 years of age. Clin Biomech 1995; 10:352–361. 
38. Cramer, A. Iliosakralmechanik. Asklepsios. 1965; 6:261–262.
39. Vleeming A, van Wingerden JP, Snijders CJ, Stoeckart R, Stijnen T. Load application to the sacrotuberous ligament; influences on sacro-iliac joint mechanics. First International Symposium on the Sacro-iliac Joint, Maastricht, 1991. ECO, PO Box 25327, Rotterdam NL.
40. Vleeming, A, Volkers, ACW, Snijders, CJ, Stoeckart, R, Relation between form and function in the sacro-iliac joint. Part 2: biomechanical aspects. Spine. 1990;15(2):133–135. 

