Chapter 23 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts
A Four-Tunnel Technique
Introduction
Anterior cruciate ligament (ACL) reconstruction is now commonly performed, and the procedure has become progressively more reliable as our understanding of the ligament’s anatomy and biomechanics has improved. Correct tunnel placement, sturdy grafts, and rigid fixation techniques all contribute to a good postoperative outcome, but the contemporary literature reveals that success rates following single-bundle ACL reconstruction vary between 69% and 95%.1–3 Moreover, the persistence of a pivot “glide” (International Knee Documentation Committee Grade B) in 15% of cases4 has raised doubts as to whether subsequent arthrosis can be prevented. Single-bundle ACL reconstruction techniques do not completely reproduce the native anatomy and function. Grafts behave similarly to the anteromedial (AM) bundle of the ACL, resulting in anterior tibial translation not being fully controlled toward extension,5 where the posterolateral (PL) bundle has been shown to have a more important action. Several studies using different measurement techniques have also shown that single-bundle grafts are even less efficacious in providing rotatory stability.6–8
A number of authors have proposed reconstructing both AM and PL bundles to address these issues. Zaricznyj9 first published early clinical results of this type of procedure in 1987, but Japanese researchers were instrumental in subsequently developing “double-bundle reconstruction.” Combined with a strong European interest in the technique, several papers have since been published.10–27 These have described numerous technical variations using either one or two tibial or femoral tunnels, either autograft or allograft, and using different graft tensioning methods.
This chapter describes a double-bundle ACL reconstruction technique that uses two independent tibial and two independent femoral tunnels. This was first described by Franceschi et al16 in 2002 and subsequently refined.17,20
Surgical Procedure
Graft Harvesting
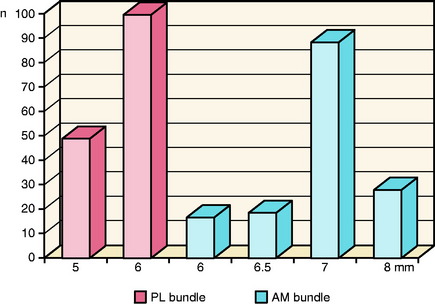
The gracilis and semitendinosus tendons are harvested using a tendon stripper as per a routine single-bundle hamstring reconstruction. The maximal length of tendon is harvested and the residual muscle removed. The gracilis graft (future PL bundle) is passed through a 15-mm continuous loop Endobutton-CL (Smith & Nephew, Mansfield, MA). A 20- to 30-mm Endobutton-CL is used for the semitendinosus graft (future AM bundle) due to the longer femoral AM tunnel. Each graft is then placed on a tensioning board and whipstitched with an absorbable #1 suture over 40 mm of its length. The two bundles are then calibrated. Grafts and the corresponding tunnel diameters are sized in 0.5-mm increments. The diameters of the double-stranded grafts are on average 6 mm for the PL bundle and 7 mm for the AM bundle (Fig. 23-1). If the diameter of the PL bundle graft measures less than 5 mm, we recommend attempting to triple the graft to increase its diameter. This is usually possible because the required length of the PL graft is shorter than the AM. If, however, the length is insufficient, then we recommend converting to a single-bundle technique.
Arthroscopic Reconstruction
The position of the arthroscopy portals is critical to allow the correct positioning of the bone tunnels. We recommend that the AM and anterolateral portals are made just adjacent to the corresponding borders of the patella tendon. Both should be placed as high as possible, just beneath the inferior border of the patella. The high anterolateral portal allows the tibial attachment of the ACL to be well visualized in the flexed knee. We do not find it necessary to use an accessory medial portal as proposed by Yagi et al.22 Following the arthroscopic evaluation and treatment of meniscal and articular lesions, the intercondylar notch is prepared. Scar tissue and ligament remnants are cleared from the 9 to 12 o’clock positions (the 12 to 3 o’clock positions in left knees), allowing the limits of the femoral ACL footprint to be well visualized.
Preparation of the Femoral Tunnels
The choice to drill the femoral tunnels via the AM portal and not via a transtibial approach is based on anatomical considerations. Several authors have shown that it is difficult to place a femoral tunnel in the anatomical attachment of the ACL via the transtibial approach.28–30 The advantages of using the AM portal have been outlined by Cha et al30 and Aglietti et al,21 who found that not only can the femoral tunnel be placed more anatomically, but that the femoral and tibial tunnels can be made independent of each other and that tunnel placement is also independent of graft type.
Although it is possible to drill the femoral AM tunnel via the tibial tunnel,24 it is not possible to reach the anatomical attachment of the PL bundle on the femur via this approach. In order to achieve anatomical placement of both tunnels on the femur, the alternative would be to use an “outside-in” approach.21,23 This necessitates the use of a second incision, made laterally, in order to position the drill guide. This approach is more invasive (incising both the lateral intermuscular septum and the capsule, which may be associated with some morbidity), and for this reason using the AM portal seems more appropriate.
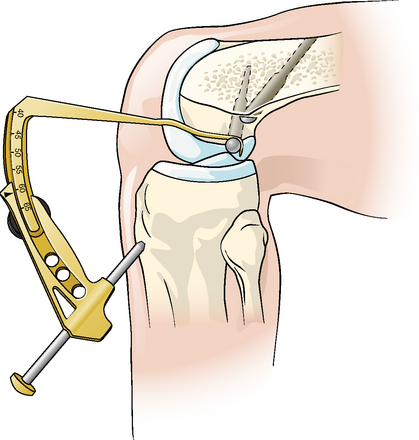
After drilling the AM tunnel, a femoral PL bundle drill guide (Fig. 23-2) is used. The appropriate size guide is introduced into the AM tunnel and then rotated so that the PL bundle tunnel is positioned lower, more shallow, and more laterally (using notch navigation terminology) in the intercondylar notch at the 2:30 position (the 9:30 position in right knees). The drill guide allows the PL tunnel to be pierced with a 4.5-mm drill (again piercing the lateral cortex) so that the two femoral tunnels diverge at 15 degrees. With the knee flexed, the AM tunnel is more vertical, measuring 45 to 50 mm in length compared with the more oblique PL tunnel, which varies between 30 and 35 mm long. The PL tunnel should breach the cortex proximal to the tibial insertion of the lateral collateral ligament such that the cortical bone is sufficient to support the Endobutton. As with the AM bundle, the PL bundle is then dilated to the appropriate diameter. The drill guide is designed so that an approximate 2-mm bony bridge is left between the tunnels as they emerge into the intercondylar notch. This corresponds to the anatomical positions of the two tunnels in the femoral ACL attachment.

Preparation of the Tibial Tunnels
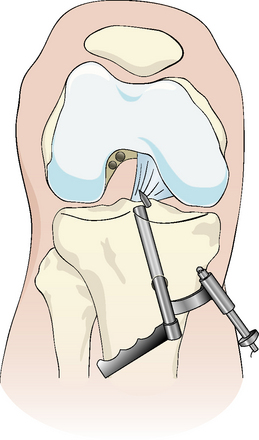
The method for drilling the two tibial tunnels is based on the use of individual AM and PL bundle drill guides. The AM guide has an arm that can be hooked over the back of the retroeminence ridge (RER), which lies just anterior to the tibial attachment of the posterior cruciate ligament (PCL) (Fig. 23-3). Our anatomical studies have shown that the distance of the center of the AM bundle from the RER varies very little individually, and the guide allows a 2.4-mm wire to be reliably positioned into the center of the AM tibial bundle attachment. The wire entry point is on the proximal tibia, just medial to the tuberosity (slightly more anterior than for a routine single bundle), and is passed at 55 degrees to the horizontal. Although the position of this tunnel as it emerges into the joint is a little more anterior than for a single-bundle reconstruction, there is no risk of impingement with the roof of the notch in extension because the graft diameter is smaller and the AM bundle lies more horizontally in the notch due to the position of the femoral tunnel.
After preparing the AM tunnel, the correspondingly sized PL bundle drill guide is used to prepare the second tibial tunnel. This drill guide is designed with two convergent barrels, one of which is introduced into the AM tunnel (Fig. 23-4) until it is just arthroscopically visible in the joint. The barrel has a line marked on its end that indicates the direction of the PL bundle guidewire. After rotating the handle guide so that the line points toward the native PL bundle attachment, a 2.4-mm guidewire is placed. The barrels of the guide converge so that the PL bundle wire is placed 9 mm posteriorly and laterally to the center of the AM bundle tunnel. This tunnel can then be drilled and dilated to the corresponding graft size. The PL bundle tibial tunnel lies less vertically, and the entry point is close to the anterior edge of the superficial medial collateral ligament. The two tunnels converge to leave an approximate 2-mm bony bridge between them as they emerge into the joint.
Discussion
Our group began to use two-bundle reconstruction in 2001. Since then we have performed approximately 1000 procedures. In the light of this experience we have noted that two-bundle reconstruction using four tunnels appears to improve the control of rotational stability. Other authors who previously performed three-tunnel, two-bundle reconstructions (using either a single tibial tunnel with two femoral tunnels, or the inverse) have also switched to using a four-tunnel technique, having found no difference between the three-tunnel techniques compared with routine single-bundle ACL reconstruction.31–33
There is now a consensus as to the positioning of the two femoral tunnels, although the question of whether to prepare them via the AM portal18,20,22,25 or with an outside-in technique13,21,23 is still the subject of debate. These alternative methods both allow anatomical tunnel placement within the native femoral ACL attachment, using slightly differing tunnel orientations. It is also increasingly clear that a transtibial approach does not allow correct anatomical positioning of the PL bundle. However, several questions persist: What is the importance of tensioning the bundles during fixation? Should the AM bundle be tensioned to the same level as the PL bundle? In which order should the bundles be fixed? There also needs to be some consensus about the correct angle of knee flexion for the fixation of each bundle,20,34 and no results are currently available to indicate the correct tibial rotation. Authors vary with regard to their preferred graft fixation methods, with some recommending femoral interference screws. However, there are no results that would indicate superior fixation characteristics using interference screws, and the majority of authors use Endobuttons. We can state from our experience that their use does not appear to be linked to significant tunnel enlargement. Yasuda et al32 found similar results, with only 9% of tunnels widening following two-bundle, four-tunnel reconstruction compared with 46% using a three-tunnel, two-bundle technique and 35% for single-bundle reconstructions. We hypothesize that the lack of tunnel widening may be explained by the two separate drill holes in both the tibia and femur, which provide a larger “footprint” and improve graft healing due to an increased bone-tendon interface. Also, when individual tunnels are used for each bundle, the grafts are more likely to restrain knee kinematics in a more physiological manner compared with a two-tunnel, single-bundle graft.35
Although the size of the doubled tendon grafts may be a problem, tripling or quadrupling the tendons is likely to yield a sufficiently strong graft. Zhoa et al27 published their 1-year results of a four-tunnel technique using two quadrupled hamstring grafts and found that 95.3% of patients had a normal Lachman (KT-1000 at 30 lb), 95% had a normal pivot shift, and 97.7% had a normal or nearly normal (A or B) IKDC score. The use of tibialis anterior and posterior allografts25 is another alternative that allows graft sizes of 8 to 9 mm for the AM bundle and 7 to 8 mm for the PL bundle.
Although some clinical results in the literature show little improvement in the control of AP stability with two-bundle, four-tunnel reconstruction,19 others have shown a tendency toward improved anterior laxity.11,26 However, it is the control of rotational kinematics that is critical; the primary disability experienced by patients with ACL rupture tends to be instability during cutting sports or turning about a weight-bearing leg, not straight anterior laxity. Unfortunately, objective assessment is still laboratory based, and an easy office method for the routine measurement of tibial rotation kinematics remains elusive.
1 Bach BRJr, Tradonsky S, Bojchuk J, et al. Arthroscopically-assisted anterior cruciate ligament reconstruction using patellar tendon autograft. Five- to nine-year follow-up evaluation. Am J Sports Med. 1998;26:20-29.
2 Freedman KB, D’Amato MJ, Nedeff DD, et al. Arthroscopic anterior cruciate ligament reconstruction: a meta-analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med. 2003;31:2-11.
3 Yunes M, Richmond JC, Engels EA, et al. Patellar versus hamstring in anterior cruciate ligament reconstruction: a meta-analysis. Arthroscopy. 2001;17:248-257.
4 Nedeff DD, Bach BRJr. Arthroscopic anterior cruciate ligament reconstruction using patellar tendon autografts: a comprehensive review of contemporary literature. Knee Surgery. 2001;14:243-258.
5 Yagi M, Wong EK, Kanamori A, et al. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30:660-666.
6 Bull AM, Earnshaw PH, Smith A, et al. Intraoperative measurement of knee kinematics in reconstruction of the anterior cruciate ligament. J Bone Joint Surg. 2002;84B:1075-1081.
7 Georgoulis AD, Papadonikolakis A, Papageorgiou CD, et al. Three-dimensional tibiofemoral kinematics of the anterior cruciate ligament-deficient and reconstructed knee during walking. Am J Sports Med. 2003;31:75-79.
8 Tashman S, Collon D, Anderson K, et al. Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:975-983.
9 Zaricznyj B. Reconstruction of the anterior cruciate ligament of the knee using a doubled tendon graft. Clin Orthop Relat Res. 1987;220:162-175.
10 Rosenberg T, Brown G. Anterior cruciate ligament reconstruction with a quadrupled semitendinosus autograft. Sports Med Arthrosc Rev. 1997;5:51-58.
11 Muneta T, Sekiya I, Yagishita K, et al. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with Endobuttons: operative technique and preliminary results. Arthroscopy. 1999;15:618-624.
12 Hara K, Kubo T, Suginoshita T, et al. Reconstruction of the anterior cruciate ligament using a double bundle. Arthroscopy. 2000;16:860-864.
13 Pederzini L, Adriani E, Botticella C, et al. Technical note: double tibial tunnel using quadriceps tendon in anterior cruciate ligament reconstruction. Arthroscopy. 2000;16:E9.
14 Hamada M, Shino K, Horibe S, et al. Single- versus bi-socket anterior cruciate ligament reconstruction using autogenous multiple-stranded hamstring tendons with Endobutton femoral fixation: a prospective study. Arthroscopy. 2001;17:801-807.
15 Mae T, Shino K, Miyama T, et al. Single- versus two-femoral socket anterior cruciate ligament reconstruction technique: biomechanical analysis using a robotic simulator. Arthroscopy. 2001;17:708-716.
16 Franceschi JP, Sbihi A, Champsaur P. Arthroscopic reconstruction of the anterior cruciate ligament using double anteromedial and posterolateral bundles. Rev Chir Orthop. 2002;88:691-697.
17 Bellier G, Christel P, Colombet P, et al. Double stranded hamstring graft for anterior cruciate ligament reconstruction. Arthroscopy. 2004;20:890-894.
18 Yasuda K, Kondo E, Ichiyama H, et al. Anatomic reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20:1015-1025.
19 Adachi N, Ochi M, Uchio Y. Reconstruction of the anterior cruciate ligament: single versus double-bundle multistranded hamstring tendons. J Bone Joint Surg. 2004;86B:515-520.
20 Christel P, Franceschi JP, Sbihi A, et al. Anatomic ACL reconstruction: the French experience. Op Tech Orthop. 2005;15:103-110.
21 Aglietti P, Cuomo P, Giron F, et al. Double-bundle anterior cruciate ligament reconstruction: surgical technique. Op Tech Orthop. 2005;15:111-115.
22 Yagi M, Kurunda R, Yoshiya S, et al. Anatomic anterior cruciate ligament reconstruction: the Japanese experience. Op Tech Orthop. 2005;15:116-122.
23 Shino K, Nakata K, Nakamura N, et al. Anatomic anterior cruciate ligament reconstruction using double-looped hamstring tendon grafts via twin femoral and triple tibial tunnels. Op Tech Orthop. 2005;15:130-134.
24 Brucker PU, Lorenz S, Imhoff AB. Anatomic fixation in double-bundle anterior cruciate ligament reconstruction. Op Tech Orthop. 2005;15:135-139.
25 Vidal AF, Brucker PU, Fu FH. Anatomic double-bundle anterior cruciate ligament reconstruction using tibialis anterior tendon allografts. Op Tech Orthop. 2005;15:140-145.
26 Colombet P, Robinson J, Jambou S, et al. Two-bundle, four-tunnel anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006;14:629-636.
27 Zhao J, Peng X, He Y, et al. Two-bundle anterior cruciate ligament reconstruction with eight-stranded hamstring tendons: four-tunnel technique. Knee. 2006;13:36-41.
28 Giron F, Buzzi R, Aglietti P. Femoral tunnel position in anterior cruciate ligament reconstruction using three techniques. A cadaver study. Arthroscopy. 1999;15:750-756.
29 Arnold MP, Kooloos J, van Kampen A. Single-incision technique misses the anatomical femoral anterior cruciate ligament insertion: a cadaver study. Knee Surg Sports Traumatol Arthrosc. 2001;9:194-199.
30 Cha PS, Chabra A, Harner CD. Single-bundle anterior cruciate ligament reconstruction using the medial portal technique. Op Tech Orthop. 2005;15:89-95.
31 Giron F, Aglietti P, Mondanelli N, et al. Single versus double bundle techniques in ACL reconstruction using a DSTG graft. Preliminary results. Proc 5th ISAKOS Congress. 2005. paper 56
32 Yasuda K, Kondo E, Ichiyama H, et al. Comparisons of clinical outcome after anterior cruciate ligament reconstruction among the one-bundle procedure, the conventional two-bundle procedure, and the anatomical two-bundle procedure. Proc 5th ISAKOS Congress. 2005. paper 59
33 Mae T, Shino K, Hamada M, et al. Comparison of “anatomical” two-bundle ACL reconstruction and Rosenberg’s bi-socket one using autogenous hamstring tendons in laxity-matched initial graft tension. Proc 5th ISAKOS Congress. 2005. paper 162
34 Miura K, Woo S L-Y, Brinkley R, et al. Determination of suitable knee flexion angles for graft fixation in double bundle ACL reconstruction. Proc 5th ISAKOS Congress. 2005. paper 1
35 Ichiyama H, Yasuda K, Kondo E, et al. An in vivo study on tension changes in the anteromedial and posterolateral bundles created with the anatomical two-route anterior cruciate ligament reconstruction procedure. Proc 5th ISAKOS Congress. 2005. paper 119






