Chapter 5 Analysis of Anterior Cruciate Ligament Injury-Prevention Programs for the Female Athlete
Introduction
Since the passage of the Title IX Educational Amendment, there has been an exponential increase of female participation in sports at both the collegiate (fivefold increase over the last 30 years)1 and high-school (tenfold increase over the last 30 years)2 levels. Although participation in organized sports has many physical and psychological benefits, including decreases in obesity, hypertension, diabetes mellitus, and coronary heart disease, this increase has subsequently led to an increase in sports-related injuries.3 While identifying risk factors with regard to sports-related injury, researchers have found an increased rate of ligamentous knee injuries, especially of the ACL, in female athletes compared with their male counterparts participating in similar activities.4–9 Among athletes in pivoting and jumping sports, adolescent females face a fourfold to sixfold increased risk of ACL injury compared with their male counterparts.6,10,11
The ACL is at risk for injury during activities that require pivoting, decelerating, or landing from a jump, such as soccer, basketball, volleyball, and team handball, as well as American football and downhill skiing.12 An estimated 80,000 to 250,000 ACL injuries occur annually in the United States alone.12,13 The highest incidence of these injuries occurs typically in young athletes between the ages of 15 to 25, which constitutes nearly 50% of all reported ACL injuries.3 Furthermore, the incidence among female athletes exceeds their male counterparts by a twofold to eightfold frequency12,13,14 Arendt and Dick examined the increased incidence of ACL injury among NCAA Division I athletes participating in basketball and soccer over a 5-year period.15 These two sports were chosen due to the fact that there is a strong similarity between the men’s and women’s games with regard to rules, training and development, style of play, type of playing surface, and the intensity of the competition. The injury rate was recorded and analyzed per athlete-exposure, where one practice session or game was defined as one exposure. The average ACL injury rate was 0.31 per 1000 athlete-exposures for female soccer and 0.29 per 1000 athlete-exposures for female basketball, compared with 0.13 for male soccer and 0.07 for male basketball per 1000 athlete-exposures. These epidemiological data for ACL injury rates statistically signify the blatant discrepancy that exists between genders.6
ACL rupture is a severe ligamentous knee injury, leading to functional instability in the short term and degenerative joint disease in the long term. Injury to the ligament can lead to prolonged absence from both work and sport and can initiate the early onset of degenerative osteoarthritis.15,16 Although ACL reconstructive procedures are readily available, the injury is painful and costly and can be debilitating. In the United States, at least 50,000 ACL reconstructions are performed each year at a cost of about $17,000 per procedure.14,17 The direct medical cost for reconstructive surgeries alone is just under $1 billion per year ($850,000,000). This figure does not include initial treatment costs of all ACL injuries, the rehabilitation costs after reconstruction, or the costs of conservative treatment and rehabilitation of those injuries that are not repaired.18 Complete ACL injuries can lead to chronic knee pathology, including instability, secondary injury to the menisci and articular cartilage, and an early onset of osteoarthritis. Approximately 66% of all patients with complete ACL injury incur damage to the menisci and the articular cartilage of the femur, patella, and/or tibia. This injury, coupled with the risk of secondary injury, can significantly decrease the ability of patients to complete their activities of daily living and affect their quality of life. The surgical reconstruction of a ruptured ACL can significantly reduce the risk of secondary injury. Seitz et al18a noted that 65% of ACL deficient patients sustained a secondary meniscal injury within 2.5 years of the initial date of injury.
Data show that despite surgical treatment of this injury, patients frequently develop posttraumatic arthritis of the knee.* Despite the most earnest efforts of orthopaedic surgeons to preserve the integrity of the knee joint during ACL reconstructive surgery, ACL reconstructed individuals continue to report with early onset of osteoarthritis. Lohmander et al completed a 12-year longitudinal study to follow up on female athletes who previously underwent ACL reconstruction after sustaining an injury while playing soccer.10 They found that 55 women (82%) had radiographic changes in their index knee and 34 (51%) fulfilled the criterion for radiographic knee osteoarthritis. The mean age for the subjects involved with this study was 31.
Gillquist et al noted that the prevalence of radiographic knee gonarthrosis is significantly higher in the injured knee compared with the unaffected contralateral limb.16 The implications of this research are ominous—hence the increased need for the prevention of these injuries from occurring in the first place.7
A multidisciplinary meeting was held in Hunt Valley, Maryland, in 1999 involving biomechanists, physicians, certified athletic trainers, and physical therapists to delineate specific risk factors thought to be directly correlated to the increased incidence of ACL injuries in the female athlete.5 The identified risk factors included anatomy, hormones, environment, and biomechanics. This meeting spurred the development of various ACL injury-prevention programs and led to increased interest and financial funding in this area of research. This group of researchers reconvened in Atlanta, Georgia, in January 2005 to reevaluate the identified risk factors and to determine what progress has been made since the inaugural meeting in 1999.
Anterior cruciate ligament Injury-Prevention Studies
A growing number of injury-prevention programs targeted at reducing the risk of ligamentous knee injury in general and ACL injury in particular have been reported in the literature. Although a number of risk factors for ACL injury have been proposed, only the biomechanical risk factors have been examined in sufficient depth to support the design and evaluation of prevention interventions.2,14
During passive motion, tension in the ACL decreases from 0 to 35 degrees and then increases again with further flexion.5 Thus, a combination of maximal ACL tension and anterior tibial translation force occurs with quadriceps firing and joint compressive loading at or near full extension. Contraction of the hamstrings decreases ACL strain in all positions. However, co-contraction of the hamstrings is not enough to overcome the strain produced by the quadriceps.7
As the knee moves into extension, female athletes take a significantly longer time to activate their hamstrings than do their male counterparts.8,9 At initial contact, males take approximately 150 ms to achieve their peak flexion angle compared with females, who take approximately 200 ms. Landing from a jump, in-line deceleration, and pivoting all involve eccentric contraction of the quadriceps to prevent the extended knee from collapsing into flexion. In laboratory studies, multiple authors4–6 have demonstrated significant anterior translation of the tibia with quadriceps contraction, particularly at 0 to 45 degrees of flexion. This anterior translation force is even greater when the quadriceps contraction is combined with a joint compressive force.4 These findings are the basis for ACL prevention strategies that emphasize proper biomechanics to address proper landing kinematics (hip and knee flexion while avoiding genu valgum), increase peak flexion angles, and improve hamstring activation and strength.
Nevertheless, a number of common elements tie these programs together. Most include one or more of the following: traditional stretching, strengthening, awareness of high-risk positions, technique modification, aerobic conditioning, sports-specific agility, proprioceptive and balance training, and plyometrics. The relation of these components to specific risk factors for ACL injury has been summarized in Table 5-1.
Table 5-1 Potential Biomechanical Deficits and Suggested Interventions
| Position | Intervention Strategy | Method of Intervention |
|---|---|---|
| Extended knee at initial contact | Knee flexion | Concentric hamstring control and soft landing |
| Extended hip at initial contact | Hip flexion | Iliopsoas and rectus femoral control and soft landing |
| Knee valgus with tibial-femoral loading | Address dynamic control, decrease dynamic valgus | Lateral hip control upon landing |
| Balance deficits | Proprioception drills | Dynamic balance training |
| Skill deficiency | Improve agility | Agility drills to address deceleration techniques and core stability |
Results of Studies Published to Date
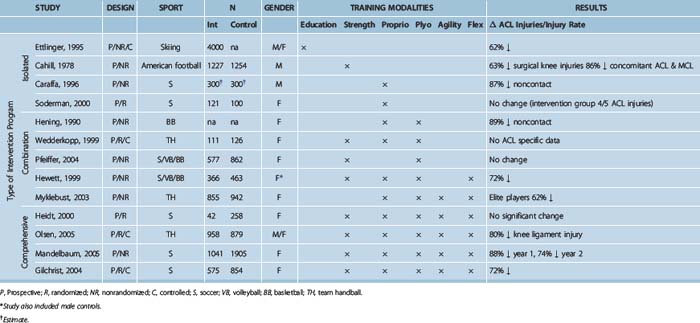
In an attempt to analyze existing ACL prevention programs, the studies are grouped and reviewed by their approach to injury prevention, beginning with the more global interventions and working up to the more comprehensive programs. Ettlinger et al25 looked at the effectiveness of an educational program to prevent ACL injury among downhill skiers by increasing awareness of injury mechanism and avoidance. Several studies have looked at the effect of isolated proprioception training on ACL injury risk, whereas a slightly more involved approach included neuromuscular training in landing and cutting techniques. Another pair of studies looked at the efficacy of technique training coupled with strengthening. Several more studies used a combination of neuromuscular training modalities. Finally, a number of studies have used a comprehensive approach to prevention of ACL injury, working on strength, flexibility, and agility as well as proprioception and plyometric training. The studies to date are summarized in Table 5-2.
Education
Ettlinger et al25 used a relatively simple approach to prevention of ACL injury in downhill skiers, attempting to modify high-risk–related behavior through education and increased awareness. In this prospective nonrandomized trial, 4000 on-slope alpine ski instructors and patrollers in 20 ski areas completed training and reporting requirements during the 1993–1994 ski season. The training kit included a 19-minute ACL awareness training videotape that showed 10 recorded ACL injuries sustained by alpine skiers of various levels, as well as various written materials. The videotape used guided discovery, allowing viewers to visualize carefully selected stimuli and incorporate this information into their skiing to avoid high-risk behavior and manage high-risk situations to reduce the risk of ACL injury. Participants also underwent an awareness training session that included proper body positioning, understanding of the phantom-foot ACL injury mechanism, and strategies to avoid high-risk positions as well as effective reaction strategies.
Isolated Strengthening and Conditioning
Cahill and Griffith26 looked at the effect of incorporating weight training into preseason conditioning for high-school American football teams. Over the 4 years of the study, they noted a reduction in reported knee injuries and knee injuries that required surgery in the intervention group.
Isolated Proprioceptive Training
Two studies have looked at the effect of isolated proprioceptive training on ACL injury risk, both in soccer players. Caraffa et al27 conducted a nonrandomized prospective study with 600 semi-professional and amateur soccer players in Umbria and Marche, Italy. Twenty teams (10 amateur and 10 semi-professional teams; Group A) underwent proprioceptive preseason training in addition to their regular training session. The control group (Group B) consisted of 20 teams (10 amateur and 10 semi-professional teams) and continued training in their usual fashion. The intervention group (A) was subjected to a five-phase progressive balance training program consisting of the following: no balance board, rectangular balance board, round balance board, combination (rectangular/round), and a biomechanical ankle platform system (BAPS) board (Camp Jackson, MI). The duration/frequency was 20 minutes per day for 2 to 6 days per week, including a minimum of 3 times per week during the season. The groups were followed for 3 years, and the senior author evaluated all players with a potential knee injury.
Soderman et al28 conducted a randomized, prospective controlled trial looking at the effectiveness of a balance board training program to reduce injuries in female soccer players. A total of 13 teams in the Swedish second and third division participated in the study, with seven teams (N = 121 players enrolled, 62 completed) in the intervention group and six teams (N = 100 players enrolled, 78 completed) in the age- and skill-matched control group through one outdoor season. The intervention consisted of a 10- to 15-minute balance board training program in addition to regularly scheduled games and practices. The players were instructed to complete the program daily for 30 days and continue with three sessions per week thereafter. Injuries were assessed with regard to number, incidence, type, and location.
Neuromuscular Training: Technique
Injury prevention has also been considered with the design of a neuromuscular training program to modulate existing athletic technique. Henning29 implemented a prevention study in two NCAA Division I female basketball programs over the course of 8 years. Henning proposed that the increased rate of ACL injury in female athletes was primarily functional, being related to knee position and muscle action during dynamic movement. In knee extension, the quadriceps exerts a significant anterior translational force on the tibia, thus imparting a shear force on the ACL. Conversely, as the knee moves into flexion, the anterior translational force on the tibia is decreased, thereby decreasing the torque on the ACL secondary to the contraction of the hamstrings. In order to decrease the risk of ACL injury, Henning proposed that the athletes cut, land, and decelerate with knee and hip flexion. In addition, he proposed a rounded cut maneuver instead of a sharp or more acute angle during the cut cycle. He also proposed that a one-step stop deceleration pattern should be avoided and a three-step quick stop be instituted instead. This intervention program was geared at changing player technique, stressing knee flexion upon landing, using accelerated rounded turns, and decelerating with a multistep stop. This protocol was completed on the basketball court without any additional equipment requirements.
The intervention group was noted to have an 89% reduction in the rate of occurrence of ACL injuries.29 Sadly, Dr. Henning’s death in 1991 prevented the publication of this research. However, his research served as the crucial foundation of numerous prevention programs that ensued.
Neuromuscular Training: Technique and Strengthening
Henning’s concept of athletic modulation has been widely accepted and expounded. Wedderkopp et al31 tested a program including functional strengthening and balance training (use of an ankle disc for 10 to 15 minutes at all practice sessions). Teams were randomized into two groups, with a total of 11 teams (N = 111) in the intervention group and 11 teams (N = 126) in the control group.
Pfeiffer et al32 developed the Knee Ligament Injury-Prevention (KLIP) program, involving 15 minutes of strengthening and plyometric activities, for female high-school soccer, volleyball (VB), and basketball (BB) players. In the first season of a 2-year, nonrandomized prospective study, 43 schools participated in the program (17 BB: N = 191; 11 soccer: N = 189; 15 VB: N = 197) and 69 schools served as the control group (28 BB: N = 319; 14 soccer: N = 244; 27 VB: N = 299). The study design included a training session for the coaches and athletic trainers and weekly compliance checks for athlete participation for both games and practices. No significant difference between the two groups was found after one season: there were three arthroscopically confirmed ACL injuries reported in the intervention athletes (incidence rate 0.167) compared with four (incidence rate 0.078) in the control group. Anecdotally, there were no noncontact ACL injuries in the intervention soccer and volleyball players; all of the injuries in the intervention group occurred among basketball players. Possible explanations for the lack of impact include the abridged duration of this intervention program (9 weeks) and the fact that the program was conducted post-training. Neuromuscular fatigue at the end of training may directly affect biomechanical technique of the athlete and limit any potential protective benefit of ACL injury-prevention programs.
Neuromuscular Training: Varied
Other studies have incorporated additional dimensions of neuromuscular training into ACL prevention efforts. The Cincinnati Sportsmetric includes flexibility, strengthening (through weight training), and plyometric activities over a duration of 60 to 90 minutes. Hewett et al33 researched the effect of this program on the incidence of knee injury in high school–age soccer, volleyball, and basketball athletes. Forty-three teams (N = 1263 athletes), including 15 female teams (N = 366), implemented the program, and 15 additional female teams (N = 463) served as the same-sex untrained control. Thirteen male sports teams (N = 434) served as the male control group. Coaches and trainers implemented the program based on a videotape and manual. The program was performed 3 days per week on alternate days. Seventy percent of the intervention athletes (248/366) completed the entire 6-week program, and the remainder completed at least 4 weeks of training to be included in the study.
When the data were stratified with regard to sport, the distribution of athletes varied widely. The intervention female group included 185 volleyball players, 97 soccer players, and 84 basketball players. The control female group included 81 volleyball players, 193 soccer players, and 189 basketball players. The male control group included 209 soccer players and 225 basketball players. The discrepancy within gender and respective sport cohorts weakens the strength of the study’s conclusion. In addition, the number of ACL injuries reported throughout this prospective study was lower compared with historical controls.2,5,34
ACL injuries have also been problematic for European team handball players. Myklebust et al35 conducted a nonrandomized prospective study looking at 900 Divisions I–III competitive female handball players over a 3-year period in Norway. Sixty teams (942 players in the 1998–1999 season) served as the control athletes (CAs), and 58 teams (855 players in the 1999–2000 season) and 52 teams (850 players in the 2000–2001 season) served as the intervention athletes (IAs). The intervention consisted of a 15-minute program focused on landing, cutting, and planting technique with 5 minutes spent on each of three exercise components: floor, balance mat, and wobble board. The program was 5 weeks long, with different exercises introduced each week. The program was to be completed three times per week during the first 5 to 7 weeks and then once per week during the season. A physical therapist was designated to each team to assess compliance during the second intervention season (2000–2001). Special equipment included an instructional videotape, a poster delineating the tasks to be completed, six balance mats, and six balance boards.
Neuromuscular Training: Comprehensive
A number of comprehensive ACL injury programs have been proposed in the literature. These programs incorporate a full range of neuromuscular training, including strengthening, flexibility, agility, proprioception, and plyometrics. Heidt et al34 developed the Frappier Acceleration Program (FAP) as a 7-week preseason training program to address ACL injuries in the high-school–age female soccer population. Three hundred female soccer players were followed over the course of 1 year (one high-school season and one club/select season). The control group included 258 athletes, whereas the intervention group included 42 athletes. The Frappier Acceleration Program consisted of sports-specific aerobic conditioning, plyometrics, sports cord resistance drills, strength training, and flexibility that was individually customized by sport, player position, and specific deficits. The plyometric progression was from unidirectional to bidirectional to multidirectional and vertical challenge (2-inch increments using foam obstacles). Injuries were defined as a player missing practice or a game, and athletic exposures were not recorded in this study.
Olsen et al36 studied a program designed to prevent lower limb injury in youth team handball. European team handball clubs (120 teams; intervention = 61 teams, 958 players; control = 59 teams, 879 players) participated in an 8-month intervention program that consisted of four sets of exercise lasting 15 to 20 minutes. The training consisted of warm-up exercises (jogging, backward running, forward running, sideways running, and speed work), technique (plant, cut, and jump shot landing), balance (passing, squats, bouncing, perturbation), and strength and power (squats, bounding, jumps, hamstrings). Each club was instructed on how to perform the program and was issued a training handbook, five wobble boards (Norpro, Norway), and five balance mats (Airex, Switzerland). The program focused on proper biomechanics during landing, core stability, and inter-rater feedback between team members. The intervention teams consisted of 16- to 17-year-old males and females who completed 15 consecutive training sessions at the start of the season, followed by 1 training session per week for the remainder of the season.
Many of these intervention programs require special equipment, specialized training, or significant time commitment. In 1999 an expert panel convened by the Santa Monica (California) Orthopedic and Sports Medicine Research Foundation designed the ACL “PEP Program: Prevent Injury and Enhance Performance.” This prevention program consists of warm-up, stretching, strengthening, plyometrics, and sport-specific agilities to address potential deficits in the strength and coordination of the stabilizing muscles around the knee joint. It was designed as an alternative warm-up so that the desired activities could be performed on the field during practice without specialized equipment for ease of implementation. The program consists of an educational videotape or DVD that demonstrates proper and improper biomechanical technique of each prescribed therapeutic exercise. An entire team can complete the 19 components in less than 20 minutes.37
An early nonrandomized study among highly competitive 14- to 18-year-old female club soccer players using the program demonstrated promising results.37 During the first year of the study (2000), 1041 female club soccer players (52 teams) performed the PEP program, and 1902 players (95 teams) served as the age- and skill-matched controls. There were 2 ACL tears (0.2 ACL injuries per athlete-exposure) in enrolled subjects versus 32 ACL tears (1.7 ACL injuries per athlete-exposure) in the control group—an 88% decrease in ACL ligament injury. In year 2 (2001) of the study, four ACL tears were reported in the intervention group, with an incidence rate of 0.47 injuries per athlete-exposure. Thirty-five ACL tears were reported in the control group, with an incidence rate of 1.8 injuries per athlete-exposure. This corresponds to an overall 74% reduction in ACL tears in the intervention group compared with an age- and skill-matched control group in year 2.
This aforementioned study was followed by a randomized controlled trial using the PEP Program in Division I NCAA women’s soccer teams in the 2002 fall season.38 Sixty-one teams with 1429 athletes completed the study, with 854 athletes participating on 35 control teams and 575 athletes participating on 26 intervention teams. No significant differences were noted between intervention and control athletes with regard to age, height, weight, or history of past ACL injuries.
Areas for Further Research
Program Specifics
Practically, a cost-benefit analysis needs to be considered prior to initiating an injury-prevention program on a large scale. First, what equipment, if any, is necessary, and at what cost? Extensive and more expensive equipment is necessary for programs such as the Frappier Acceleration Program,34 the Cincinnati Sportsmetric program,33 and the various programs using some form of a balance board.30,31,34,35 Other successful programs such as PEP37,38 and the Henning program29 do not have such prohibitive requirements. Secondly, what is the minimal time commitment needed to provide adequate protection? How long and how frequent should training sessions be? When should these programs be introduced? What is the minimum duration of an injury-prevention program, or does it need to be continued, perhaps at a lesser frequency throughout the course of the season? When initiating a neuromuscular intervention program, it takes approximately 4 to 6 weeks to impart a benefit onto the athlete. Most of the programs studied to date have a relatively intense start-up period for 4 to 6 weeks followed by less frequent, and in some cases, no additional training.
Effect on Performance
Another important issue is the effect of ACL injury-prevention programs on athletic performance. This is particularly important when the relatively poor compliance with some of the injury-prevention programs reviewed previously is compared with the much higher rates of compliance, upwards of 80% to 90%, that have been reported with training targeted toward improving performance.39–43
Recent studies have begun to assess this issue, and the results are encouraging. In 1996, before the program had been found to decrease ACL injury risk, Hewett et al44 reported that the Sportsmetric program increased vertical jump, improved control of dynamic loading of the knee, and increased hamstring strength, power, and peak torque in female volleyball players. Wilkerson et al45 looked at the impact of the Cincinnati Sportsmetric program on performance in a small cohort of female collegiate basketball players. They found significantly increased hamstring strength in the intervention group but no other changes in either group. Meyer et al43 looked at the effect of an enhanced training program based on the Cincinnati Sportsmetric program on performance. In this study, female athletes demonstrated increased strength and power and improved knee biomechanics after training compared with no change in the control group. Paterno et al47 created their own program of exercises similar to those described in the literature for injury prevention and found improved single-limb total stability and anteroposterior stability. There was no control group in this study. Holm et al48 looked at the influence of the program used by Myklebust35 on female team handball players and found an improvement in dynamic balance but no other significant changes. Again, there was no control group for this study. Thus, although these studies suggest there may be some improvement in performance from participation in ACL injury-prevention programs, further study, particularly with larger, well-designed studies, is needed to more precisely assess the impact of such programs on performance.
1 Garrick JG, Requa RK. Anterior cruciate ligament injuries in men and women: how common are they? In: Griffin LY, editor. Prevention of noncontact ACL injuries. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2001:1-9.
2 Bahr R, Holme I. Risk factors for sports injuries—a methodological approach. Br J Sports Med. 2003;37:384-392.
3 Feagin JAJr, Lambert KL, Cunningham PR, et al. Consideration of the anterior cruciate ligament injury in skiing. Clin Orthop Relat Res. 1987;216:13-18.
4 Frank CB, Jackson DW. The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am. 1997;79:1556-1576.
5 Griffin LY, Agel J, Albohn MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8:141-150.
6 Myklebust G, Holm I, Maehlum S. Clinical, functional and radiological outcome 6–11 years after ACL injuries in team handball players—a follow-up study. Am J Sports Med. 2003;31:981-989.
7 Daniels DM, Stone MI, Dobson BL, et al. Fate of the ACL injured patient: a prospective outcome study. Am J Sports Med. 1994;22:632-644.
8 Ferretti A, Conteduca F, DeCarli A, et al. Osteoarthritis of the knee after ACL reconstruction. Int Orthop. 1991;15:367-371.
9 Fithian DC, Paxton EW, Stone ML, et al. Prospective trial of a treatment algorithm for the management of anterior cruciate ligament injured knee. Am J Sports Med. 2005;33:23-28.
10 Lohmander LS, Osteber A, Englind M, et al. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Ann Rheum Dis. 2004;10:314-352.
11 Myklebust G, Maehlum S, Holm I, et al. A prospective cohort study of ACL injuries in elite Norwegian team handball. Scand J Med Sci Sports. 1998;8:149-153.
12 Roos H, Adalberth T, Dahlberg L. Osteoarthritis of the knee after injury to the anterior cruciate ligament or meniscus. The influence of time and age. Osteoarthr Cart. 1995;3:261-267.
13 Sommerlath K, Lysholm J, Gillquist J. The long term course after treatment of acute anterior cruciate ligament ruptures. Am J Sports Med. 1991;19:156-162.
14 Von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: a study of radiographic and patient relevant outcomes. Ann Rheum Dis. 2004;63:269-273.
15 Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med. 1995;23:694-701.
16 Gillquist J, Messner K. Anterior cruciate ligament reconstruction and the long-term incidence of gonarthrosis. Sports Med. 1999;27:143-156.
17 Chandy TA, Grana WA. Secondary school athletic injury in boys and girls: A three year comparison. Phys Sportsmed. 1985;13:106-111.
18 Gray J, Taunton JE, McKenzie DC, et al. A survey of injuries to the anterior cruciate ligament of the knee in female basketball players. Int J Sports Med. 1985;6:314-316.
18a Seitz H, Marlovits S, Wielke T, Vescei V. Meniscus lesions after isolated anterior cruciate ligament rupture. Wien Klin Wochenschr. 1996;22:727-730.
19 Lindenfeld TN, Schmitt DJ, Hendy MP, et al. Incidence of injury in indoor soccer. Am J Sports Med. 1994;22:364-371.
20 Malone TR, Hardaker WT, Garrett WE, et al. Relationship of gender to ACL injuries in intercollegiate basketball players. J South Orthop Assoc. 1992;2:36-39.
21 Strand T, Wisnes AR, Tvedte R, et al. ACL injuries in team handball. J Nor Med Assoc. 1990;110:45-48.
25 Ettlinger CF, Johnson RJ, Shealy JE. A method to help reduce the risk of serious knee sprains incurred in alpine skiing. Am J Sports Med. 1995;23:531-537.
26 Cahill BR, Griffith EH. Effect of preseason conditioning on the incidence and severity of high school football injuries. Am J Sports Med. 1978;6:180-184.
27 Caraffa A, Cerulli G, Projetti M, et al. Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surg Sports Traumatol Arthrosc. 1996;4:19-21.
28 Soderman K, Werner S, Pietila T, et al. Balance board training: prevention of traumatic injuries of the lower extremities in female soccer players? A prospective randomized intervention study. Knee Surg Sports Traumatol Arthrosc. 2000;8:356-363.
29 Henning CE, Griffis ND. Injury prevention of the anterior cruciate ligament (videotape). Wichita, KS: Mid-America Center for Sports Medicine, 1990.
31 Wedderkopp N, Kaltoft M, Lundgaard B, et al. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9:41-47.
32 Pfeiffer RP, Shea K, Grandstrand S, et al. Effects of a knee ligament injury prevention (KLIP) program on the incidence of noncontact ACL injury: a two-year prospective study of exercise intervention in high school female athletes. Podium presentation at the American Orthopaedic Society for Sports Medicine (AOSSM), Specialty Day, San Francisco, CA. March, 2004.
33 Hewett TE, Lindenfeld TN, Riccobene JV, et al. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:669-706.
34 Heidt RSJr, Sweeterman LM, Carlonas RL, et al. Avoidance of soccer injuries with preseason conditioning. Am J Sports Med. 2000;28:659-662.
35 Myklebust G, Engebretsen L, Braekken IH, et al. Prevention of anterior cruciate ligament injuries in female team handball players: a prospective intervention study over three seasons. Clin J Sport Med. 2003;13:71-78.
36 Olsen OE, Myklebust G, Engebretsen L, et al. Exercises to prevent lower limb injuries in youth sports: cluster randomised controlled trial. BMJ. 2005;330:449.
37 Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular and proprioceptive training program in preventing anterior cruciate ligmaent injuries in female athletes. 2-year follow-up. Am J Sports Med. 2005;33:1003-1010.
38 Gilchrist J, Mandelbaum BR, Silvers HJ. AAOS Annual Meeting, AOSSM Specialty Day, San Francisco, CA. March 2004.
39 Ben-Sira D, Ayalon A, Tavi M. The effect of different types of strength training on concentric strength in women. J Strength Cond Res. 1995;9:143-148.
40 Hakkinen K, Alen M, Kraemer WJ, et al. Neuromuscular adaptations during concurrent strength and endurance training versus strength training. Eur J Appl Physiol. 2003;89:42-52.
41 Kraemer WJ, Duncan ND, Volek JS. Resistance training and elite athletes: adaptations and program considerations. J Orthop Sports Phys Ther. 1998;28:110-119.
42 Kraemer WJ, Hakkinen K, Triplett-McBride NT, et al. Physiological changes with periodized resistance training in women tennis players. Med Sci Sports Exerc. 2003;35:157-168.
43 Wroble RR, Moxley DR. The effect of winter sports participation on high school football players: strength, power, agility and body composition. J Strength Cond Res. 2001;15:132-135.
44 Hewett TE, Stroupe AL, Nance TA, et al. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765-773.
45 Wilkerson GB, Colston MA, Short NI, et al. Neuromuscular changes in female collegiate athletes resulting from a plyometric jump-training program. J Athl Train. 2004;39:17-23.
47 Paterno MV, Myer GD, Ford KR, et al. Neuromuscular training improves single-limb stability in young female athletes. J Orthop Sports Phys Ther. 2004;34:305-316.
48 Holm I, Fosdahl MA, Friis A, et al. Effect of neuromuscular training on proprioception, balance, muscle strength, and lower limb function in female team handball players. Clin J Sport Med. 2004;14:88-94.






