Focal amyloid involvement may be low signal on T2WI
• Fluoroscopic findings
Stomach: Thick folds (which may appear nodular or mass-like) ± calcification
Small intestine: Symmetrical thickening of folds, impaired motility, and slow transit
Colon: Luminal narrowing, loss of haustrations, and thickened transverse folds
CLINICAL ISSUES
• Symptoms depend on site of protein deposition
• Most common sites are kidneys, heart, liver, and GI tract
• Renal failure due to amyloid deposition in kidneys is most common cause of death (50%)
• GI tract involvement: GI bleeding, intestinal dysmotility, malabsorption, and protein-losing gastroenteropathy
(Left) Axial NECT shows an abnormally hypodense and mildly enlarged liver and spleen in this patient with biopsy-proven primary amyloid of the liver.
(Right) Spot film from a small bowel follow-through shows diffuse fold thickening throughout the jejunum. This is a very nonspecific finding, one that required biopsy for the diagnosis of amyloidosis.
(Left) Axial CECT in a patient with amyloidosis demonstrates rind-like soft tissue thickening surrounding the left kidney with internal calcification .
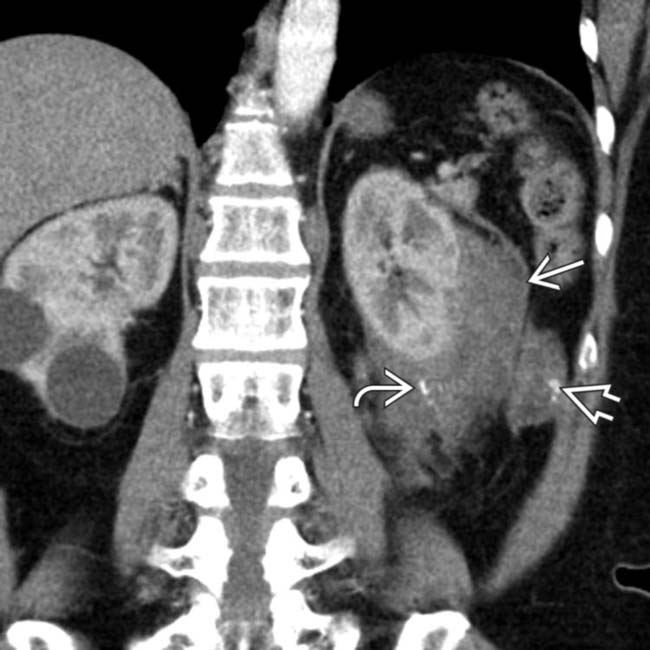
(Right) Coronal CECT in the same patient demonstrates similar thickening and calcification surrounding the left kidney, as well as a more focal soft tissue mass (amyloidoma) in the adjacent retroperitoneum.
TERMINOLOGY
Synonyms
• Systemic amyloidosis
Definitions
• Group of diseases characterized by deposition of abnormal protein (amyloid) in various tissues
May be systemic (involving multiple organs in 80%) or localized (in single organ or tissue in 20%)
Classified based on type of protein being deposited
– 30 different amyloidogenic proteins in humans
• Primary: Due to monoclonal plasma cell dyscrasia (associated with no other underlying disease)
• Secondary: Develops in setting of a number of different chronic inflammatory diseases
IMAGING
General Features
• Best diagnostic clue
Small bowel wall thickening and hypomotility in patient with underlying chronic illness
• Location
Small intestine, stomach, colorectum, esophagus, liver, kidney, heart
• Morphology
Nonspecific small bowel fold thickening and hypomotility
Nonspecific hepatomegaly (1/2 of patients)
Nonspecific splenomegaly
Nonspecific enlarged kidneys
Imaging Recommendations
• Best imaging tool
Small bowel enteroclysis or small bowel follow-through for intestinal involvement; CECT for other organs
Radiographic Findings
• Small intestine: Symmetrical thickening of folds, impaired motility, and slow transit
• Stomach: Thickened folds (which may appear nodular or mass-like) ± calcification
• Colon: Luminal narrowing, loss of haustrations, and thickened transverse folds
CT Findings
• Genitourinary tract
Acute disease: Enlarged kidneys
Chronic disease: Small kidneys with cortical thinning
Focal masses (amyloidomas) may develop in kidneys
Perinephric mass-like soft tissue thickening extending downwards along ureters
• Gastrointestinal tract
Small bowel, large bowel, and stomach can be involved
– Bowel wall thickening, distension, intramural hemorrhage, and intussusceptions
– Wall thickening can be focal or diffuse ± calcification
Can be nodular and mimic tumor/mass
Hepatosplenomegaly
– Patchy or diffuse parenchymal hypoattenuation ± calcification
– Spleen at increased risk of spontaneous rupture
Gallbladder wall thickening
Mass-like amyloidomas in soft tissues ± calcification
Hereditary amyloidosis: Liver transplantation (protein produced by liver)
Axial NECT demonstrates extensive calcifications in the subcutaneous soft tissues in a patient with amyloidosis.
Axial NECT in the same patient demonstrates a calcified soft tissue mass in the left abdomen. Amyloid deposits can be focal and mass-like, as in this case.
Axial CECT in a patient with amyloidosis demonstrates extensive mediastinal and hilar lymphadenopathy with subtle calcification .
Coronal CECT in the same patient demonstrates nodular deposits in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
Coronal CECT in the same patient demonstrates nodular deposits in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
Axial NECT shows primary amyloidosis in a patient initially misdiagnosed as having multiple myeloma. Note the enlarged and hypodense liver that simulates steatosis. However, liver biopsy revealed amyloid and no steatosis or myeloma. In a patient with myeloma or other malignancy, one would also have to consider diffuse tumor infiltration.
Axial CECT in the same patient shows primary amyloidosis in a patient initially misdiagnosed as having multiple myeloma. There is characteristic patchy hypoattenuation throughout the liver parenchyma. While this finding simulates steatosis, liver biopsy revealed amyloid and no steatosis. There is a hypervascular mass that represents an incidental focal nodular hyperplasia.












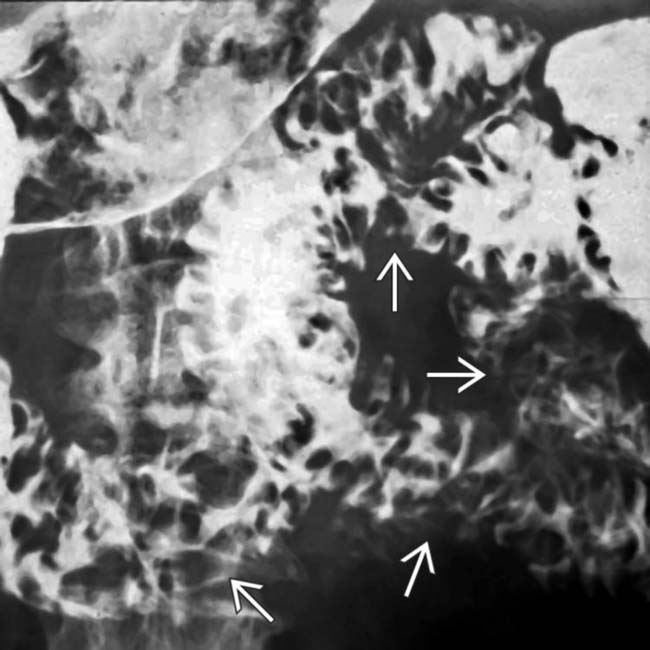
 throughout the jejunum. This is a very nonspecific finding, one that required biopsy for the diagnosis of amyloidosis.
throughout the jejunum. This is a very nonspecific finding, one that required biopsy for the diagnosis of amyloidosis.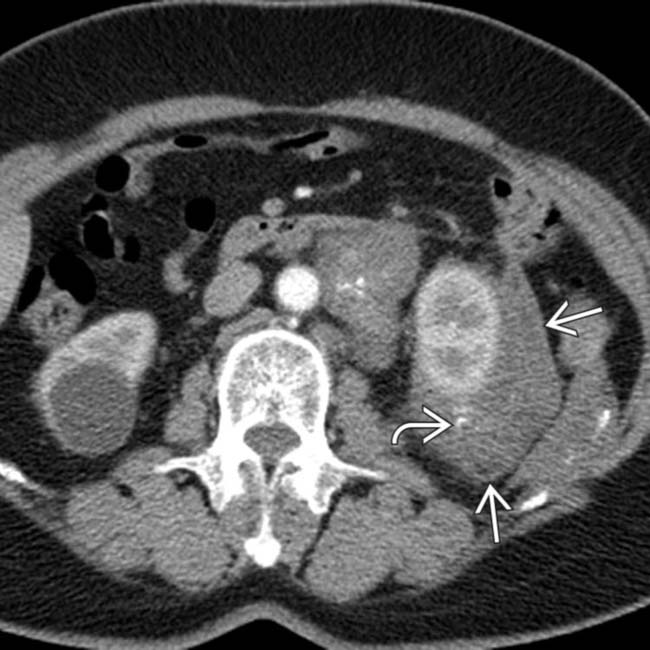
 surrounding the left kidney with internal calcification
surrounding the left kidney with internal calcification  .
.
 and calcification
and calcification  surrounding the left kidney, as well as a more focal soft tissue mass
surrounding the left kidney, as well as a more focal soft tissue mass  (amyloidoma) in the adjacent retroperitoneum.
(amyloidoma) in the adjacent retroperitoneum.































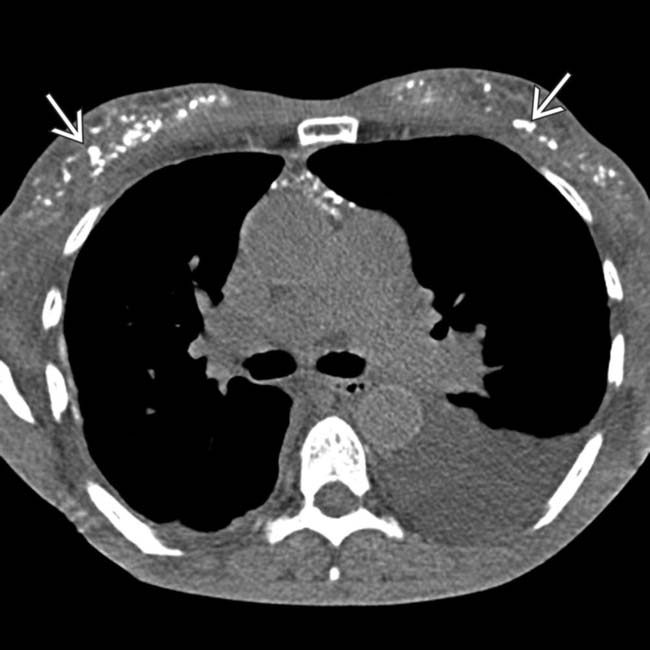
 in the subcutaneous soft tissues in a patient with amyloidosis.
in the subcutaneous soft tissues in a patient with amyloidosis.
 in the left abdomen. Amyloid deposits can be focal and mass-like, as in this case.
in the left abdomen. Amyloid deposits can be focal and mass-like, as in this case.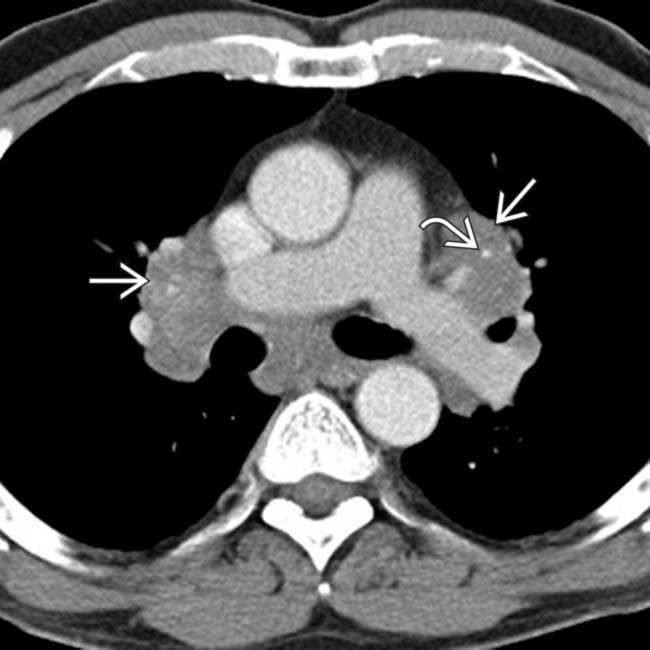
 with subtle calcification
with subtle calcification  .
.
 in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
 in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
in the walls of the small bowel in multiple locations. Amyloidosis can present with nodular, focal wall thickening.
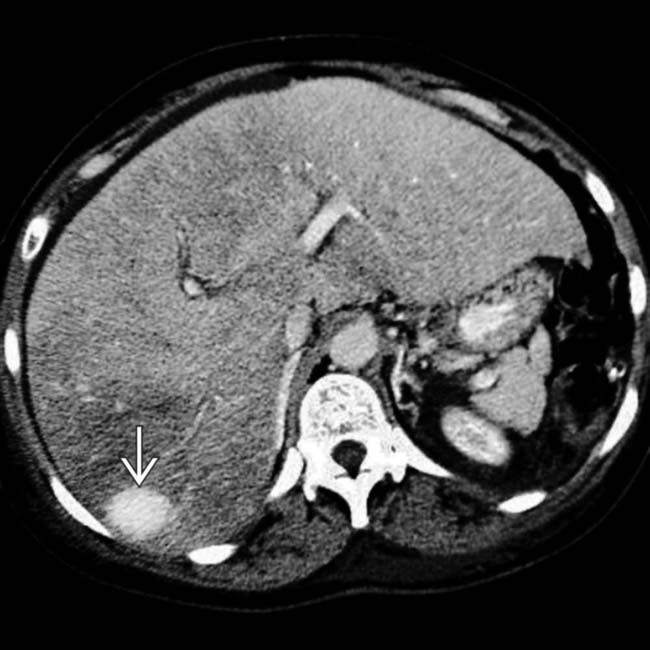
 that represents an incidental focal nodular hyperplasia.
that represents an incidental focal nodular hyperplasia.


