Chapter 28 Acute Myocardial Infarction
1 Who is at risk for acute myocardial infarction (AMI)?



3 How are patients typically seen initially with an AMI?



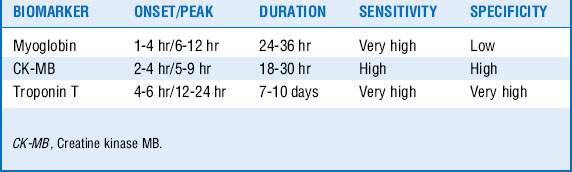
4 Which biomarkers diagnose AMI?
The recently adopted universal definition of AMI includes elevation in cardiac biomarkers above the 99th percentile of the upper reference limit. See Table 28-1.
5 How do you diagnose an ST-elevation MI (STEMI)?



6 In whom does cardiogenic shock develop?



7 What is the prognosis of a patient with AMI and out-of-hospital cardiac arrest?


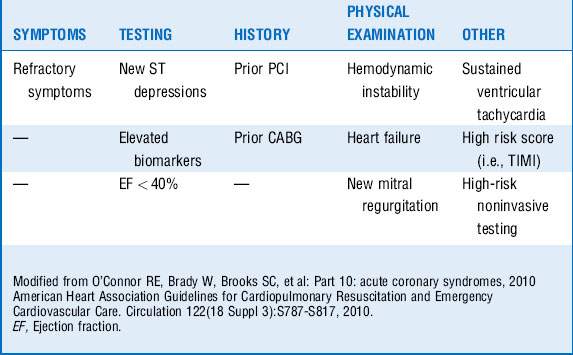
12 You are evaluating a patient with unstable angina. What patient characteristics would sway you to choose an early referral to the catheterization laboratory and possible invasive revascularization?
17 What are the indications for cooling or hypothermia after AMI and cardiac arrest?
 Adult successfully resuscitated from a witnessed out-of-hospital or in-hospital cardiac arrest and now hemodynamically stable
Adult successfully resuscitated from a witnessed out-of-hospital or in-hospital cardiac arrest and now hemodynamically stable

Key Points Treatment of Acute Myocardial Infarction
1. Distinguish between unstable angina [UA]–NSTEMI and STEMI: STEMI is an occluded artery and requires immediate reperfusion with PCI or fibrinolysis; UA-NSTEMI requires medical therapy and invasive approach (within 4-48 hours of presentation) for all patients at increased risk.
2. Oral antiplatelet therapy should be initiated including aspirin and clopidogrel, prasugrel, or ticagrelor.
3. Antithrombotics (heparin, enoxaparin, fondaparinux, or bivalirudin) should be administered with weight- and glomerular filtration rate–adjusted dosing to avoid bleeding risks.
4. Statin, β-blocker, and ACE inhibitors should be considered in all patients with AMI regardless of baseline LDL level, blood pressure, and heart rate.
5. Revascularization (PCI, CABG) is warranted immediately (STEMI–primary PCI) or urgently (STEMI-postlytic, pharmacoinvasive approach) or within 4 to 48 hours of presentation (high-risk UA-NSTEMI).
1 Antman E.M., Cohen M., Bernink P.J., et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842.
2 Dauerman H.L. Challenges in oral antiplatelet therapy: ST-segment elevation myocardial infarction. Am J Cardiol. 2009;104(5 Suppl):39C–43C.
3 Dauerman H.L., Sobel B.E. Synergistic treatment of ST-segment elevation myocardial infarction with pharmacoinvasive recanalization. J Am Coll Cardiol. 2003;42:646–651.
4 De Backer D., Biston P., Devriendt J., et al. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362:779–789.
5 Holzer M. Targeted temperature management for comatose survivors of cardiac arrest. N Engl J Med. 2010;363:1256–1264.
6 Redpath C., Sambell C., Stiell I., et al. In-hospital mortality in 13,263 survivors of out-of-hospital cardiac arrest in Canada. Am Heart J. 2010;159:577–583. e1
7 Reynolds H.R., Hochman J.S. Cardiogenic shock: current concepts and improving outcomes. Circulation. 2008;117:686–697.
8 Sleeper L.A., Ramanathan K., Picard M.H., et al. Functional status and quality of life after emergency revascularization for cardiogenic shock complicating acute myocardial infarction. J Am Coll Cardiol. 2005;46:266–273.
9 Stone G.W., Maehara A., Lansky A.J., et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–235.
10 Thygesen K., Alpert J.S., White H.D., et al. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50:2173–2195.
11 White H.D., Chew D.P. Acute myocardial infarction. Lancet. 2008;372:570–584.
12 Wiviott S.D., Braunwald E., McCabe C.H., et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357:2001–2015.
