Chapter 620 Abnormalities of the Lens
Cataracts
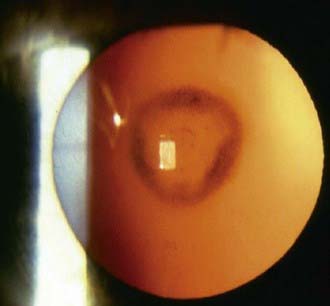
A cataract is any opacity of the lens (Fig. 620-1). Some are clinically unimportant; others significantly affect visual function. The incidence of infantile cataracts is approximately 2-13/10,000 live births. An epidemiologic study of infantile cataracts published in 2003 suggests that approximately 60% of cataracts are an isolated defect; 22% are part of a syndrome; and the remainder is associated with other unrelated major birth defects. Cataracts are more common in low birthweight infants. Infants at or below 2,500 g have a 3- to 4-fold increased odds of developing infantile cataracts. Some cataracts are associated with other ocular or systemic disease.

Differential Diagnosis
The differential diagnosis of cataracts in infants and children includes a wide range of developmental disorders, infectious and inflammatory processes, metabolic diseases, and toxic and traumatic insults (Table 620-1). Cataracts may also develop secondary to intraocular processes, such as retinopathy of prematurity, persistent hyperplastic primary vitreous, retinal detachment, retinitis pigmentosa, and uveitis. A portion of cataracts in children are inherited (Fig. 620-2).
Table 620-1 DIFFERENTIAL DIAGNOSIS OF CATARACTS
DEVELOPMENTAL VARIANTS
Prematurity (Y-suture vacuoles) with or without retinopathy of prematurity
GENETIC DISORDERS
Simple Mendelian Inheritance
Major Chromosomal Defects
Multisystem Genetic Disorders
Inborn Errors of Metabolism
ENDOCRINOPATHIES
CONGENITAL INFECTIONS
OCULAR ANOMALIES
MISCELLANEOUS DISORDERS
IDIOPATHIC
Metabolic Disorders
Cataracts are a prominent manifestation of many metabolic diseases, particularly certain disorders of carbohydrate, amino acid, calcium, and copper metabolism. A primary consideration in any infant with cataracts is the possibility of galactosemia (Chapter 81.2). In classic infantile galactosemia, galactose-1-phosphate uridyl transferase deficiency, the cataract is typically of the zonular type, with haziness or opacification of 1 or more of the perinuclear layers of the lens Haziness or clouding of the nucleus also often occurs. In its early stages, the cataract generally has a distinctive oil droplet appearance and is best detected with the pupil fully dilated. Progression to complete opacification of the lens may occur within weeks. With early treatment (galactose-free diet), the lens changes may be reversible.
The distinctive sunflower cataract of Wilson disease is not commonly seen in children. Various lens opacities may be seen in children with certain of the sphingolipidoses, mucopolysaccharidoses, and mucolipidoses, particularly Niemann-Pick disease, mucosulfatidosis, Fabry disease, and aspartylglycosaminuria (Chapters 80 and 82).
Chromosomal Defects
Lens opacities of various types may occur in association with chromosomal defects, including trisomies 13, 18, and 21; Turner syndrome; and a number of deletion (11p13, 18p, 18q) and duplication (3q, 20p, 10q) syndromes (Chapter 76).
Miscellaneous Disorders
The list of multisystem syndromes and diseases associated with lens opacities and other eye anomalies is extensive (see Table 620-1).
Ectopia Lentis
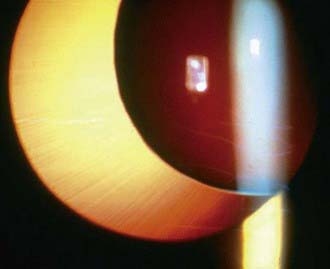
Normally, the lens is suspended in place behind the iris diaphragm by the zonular fibers of the ciliary body. Abnormalities of the suspensory system resulting from a developmental defect, disease, or trauma may result in instability or displacement of the lens. Displacement of the lens is classified as luxation (dislocation–complete displacement of the lens) (Fig. 620-3) or as subluxation (partial displacement–shifting or tilting of the lens) (Fig. 620-4). Symptoms include blurring of vision, which is often the result of refractive changes such as myopia, astigmatism, or aphakic hyperopia. Some patients experience diplopia (double vision). An important sign of displacement is iridodonesis, a tremulousness of the iris caused by the loss of its usual support. Also, the anterior chamber may appear deeper than normal. Sometimes the equatorial region (“edge”) of the displaced lens may be visible in the pupillary aperture. On ophthalmoscopy, this may appear as a black crescent. Also, the difference between the phakic and aphakic portions can be appreciated when focusing on the fundus.
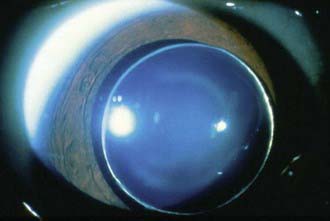
Figure 620-3 Complete dislocation of lens into the anterior chamber seen in Weill-Marchesani syndrome.
Differential Diagnosis
Systemic disorders associated with displacement of the lens include Marfan syndrome, homocystinuria, Weill-Marchesani syndrome, and sulfite oxidase deficiency (Chapter 79). Ectopia lentis occurs in approximately 80% of patients with Marfan syndrome, and in about 50% of patients; the ectopia is evident by the age of 5 yr. In most cases, the lens is displaced superiorly and temporally; it is almost always bilateral and relatively symmetric. In homocystinuria, the lens is usually displaced inferiorly and somewhat nasally. It occurs early in life and is often evident by 5 yr of age. In Weill-Marchesani syndrome, the displacement of the lens is often downward and forward, and the lens tends to be small and round.
Anterior Lenticonus
Rupture of the anterior capsule may occur, requiring prompt surgical intervention.
Anteby I, Isaac M, BenEzra D. Hereditary subluxated lenses: visual performances and long-term follow-up after surgery. Ophthalmology. 2003;110:1344-1348.
Bhatti TR, Dott M, Yoon PW, et al. Descriptive epidemiology of infantile cataracts in metropolitain Atlanta, GA, 1968–1998. Arch Pediatr Adolesc Med. 2003;157:341-347.
Chugh KS, Sakhuja V, Agarwal A, et al. Hereditary nephritis (Alport’s syndrome)—clinical profile and inheritance in 28 kindreds. Nephrol Dial Transplant. 1993;8:690-695.
Fallaha N, Lambert SR. Pediatric cataracts. Ophthalmol Clin North Am. 2001;14:479-492.
Léonard A, Bernard P, Hiel AL, et al. Prenatal diagnosis of fetal cataract: case report and review of the literature. Fetal Diagn Ther. 2009;26:61-67.
Levin AV, Edmonds SA, Nelson LB, et al. Extended-wear contact lenses for the treatment of pediatric aphakia. Ophthalmology. 1988;95:1107-1113.
McClatchey SK, Hofmeister EM. The optics of aphakic and pseudophakic eyes in childhood. Surv Ophthalmol. 2009;55:174-182.
Peterseim MW, Wilson ME. Bilateral intraocular lens implantation in the pediatric population. Ophthalmology. 2000;107:1261-1266.
Plager DA, Yang S, Neely D, et al. Complications in the first year following cataract surgery with and without IOL in infants and older children. J AAPOS. 2002;6:9-14.
Russell-Eggit IM. Non-syndromic posterior lenticonus a cause of childhood cataract: evidence for X-linked inheritance. Eye (Lond). 2000;14(Pt 6):861-863.
SanGiovanni JP, Chew EY, Reed GF, et al. Infantile cataract in collaborative perinatal project: prevalence and risk factors. Arch Ophthalmol. 2002;120:1559-1565.
Tesser RA, Hess DB, Buckley EG. Pediatric cataracts and lens anomalies. In: Nelson LB, Olitsky SE, editors. Harley’s pediatric ophthalmology. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2005:255-284.





