[level-membership-for-surgery-category]
CHAPTER 12 Abdominal wall and hernia
Herniae
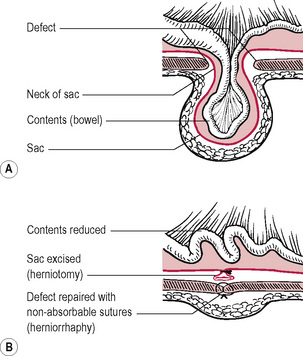
Reducible hernia
This is one in which the contents of the sac reduce spontaneously or can be pushed back manually.
Classification of hernia
Types of hernia
Inguinal hernia
This is the most common form of hernia. There are two types: indirect and direct.
Direct
Both types may occur and straddle the inferior epigastric artery, the so-called ‘pantaloon’ hernia.
Treatment
Uncomplicated
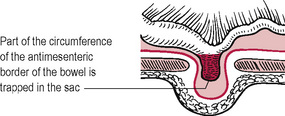
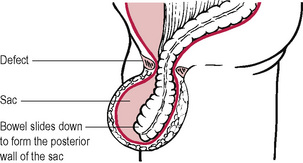
Obstructed and strangulated herniae
These require emergency surgery, with resection of bowel if necessary followed by surgical repair.
Femoral hernia
Treatment
Repair of femoral hernia (low approach)
Incisional hernia
This occurs through a defect in the scar of a previous abdominal incision.
Other conditions of the abdominal wall
Swellings in the groin and scrotum
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 12 Abdominal wall and hernia
Herniae
Reducible hernia
This is one in which the contents of the sac reduce spontaneously or can be pushed back manually.
Classification of hernia
Types of hernia
Inguinal hernia
This is the most common form of hernia. There are two types: indirect and direct.
Direct
Both types may occur and straddle the inferior epigastric artery, the so-called ‘pantaloon’ hernia.
