[level-membership-for-radiology-category] CT: Linear high-density foci within dilated biliary tree
 US: Tubular echogenic structure, 3-6 mm in diameter, with central anechoic area (digestive tract of worm)
US: Tubular echogenic structure, 3-6 mm in diameter, with central anechoic area (digestive tract of worm)• Clonorchiasis: Flukes typically involve peripheral intrahepatic ducts, not GB, CBD, or PD


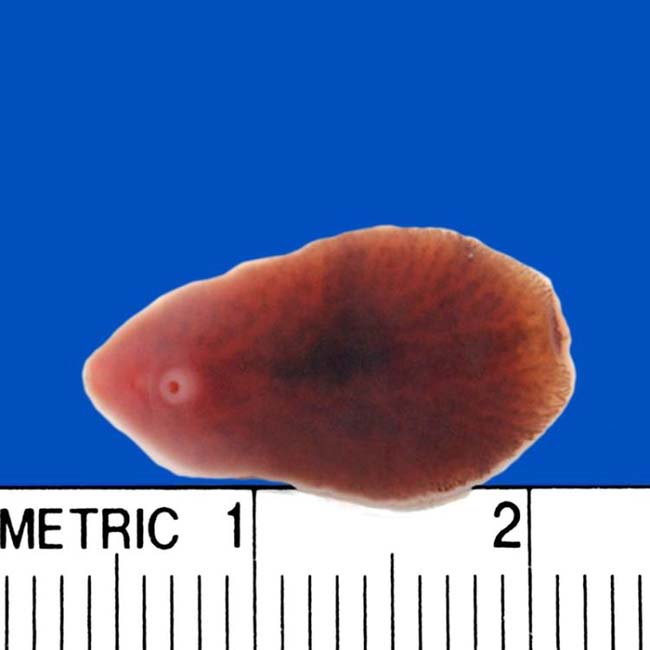
• Fascioliasis: Flukes usually involve large intrahepatic ducts, extrahepatic duct, and GB (after liver involvement)

• Echinococcosis: Communication of hepatic hydatid cyst with small biliary radicles or rupture of cyst into bile ducts




 from a biliary Ascaris worm.
from a biliary Ascaris worm.
 . The worm was mobile at real-time examination. Central hypoechogenicity is thought to represent the digestive tract of the worm. (Courtesy A. Dasyam, MD.)
. The worm was mobile at real-time examination. Central hypoechogenicity is thought to represent the digestive tract of the worm. (Courtesy A. Dasyam, MD.)IMAGING
General Features
• Best diagnostic clue










CT Findings
• Ascariasis/clonorchiasis: Intraductal high-density foci within dilated biliary tree due to biliary worms/flukes or debris




MR Findings

• Clonorchiasis: Preferential peripheral biliary dilatation with low-signal filling defects on T2WI or MRCP


Ultrasonographic Findings
• Grayscale ultrasound
 Ascariasis: Ultrasound very sensitive for worms in biliary system, but insensitive for worms in duodenum or ampulla (sensitivity for pancreatobiliary ascariasis only 50%)
Ascariasis: Ultrasound very sensitive for worms in biliary system, but insensitive for worms in duodenum or ampulla (sensitivity for pancreatobiliary ascariasis only 50%)
Ascariasis: Ultrasound very sensitive for worms in biliary system, but insensitive for worms in duodenum or ampulla (sensitivity for pancreatobiliary ascariasis only 50%)






DIFFERENTIAL DIAGNOSIS
Bacterial Cholangitis
Recurrent Pyogenic Cholangitis
• Disease associated with formation of pigment stones throughout biliary tree, as well as multiple biliary strictures and repeated bouts of cholangitis
PATHOLOGY
General Features
• Etiology
 Clonorchiasis : Flukes ingested with uncooked freshwater fish → metacercariae excyst in duodenum → move to ampulla of Vater and ascend biliary tree
Clonorchiasis : Flukes ingested with uncooked freshwater fish → metacercariae excyst in duodenum → move to ampulla of Vater and ascend biliary tree
 Clonorchiasis : Flukes ingested with uncooked freshwater fish → metacercariae excyst in duodenum → move to ampulla of Vater and ascend biliary tree
Clonorchiasis : Flukes ingested with uncooked freshwater fish → metacercariae excyst in duodenum → move to ampulla of Vater and ascend biliary tree




CLINICAL ISSUES
Presentation






Demographics
• Age
 Ascariasis more common in children, but hepatobiliary involvement more common in adults (pediatric biliary tree may be too small for parasites to enter)
Ascariasis more common in children, but hepatobiliary involvement more common in adults (pediatric biliary tree may be too small for parasites to enter)
 Clonorchis can colonize bile ducts for 25 years, and symptomatic infections are more common in older adults as disease burden can increase over time
Clonorchis can colonize bile ducts for 25 years, and symptomatic infections are more common in older adults as disease burden can increase over time
Ascariasis more common in children, but hepatobiliary involvement more common in adults (pediatric biliary tree may be too small for parasites to enter) Clonorchis can colonize bile ducts for 25 years, and symptomatic infections are more common in older adults as disease burden can increase over time








Treatment
• Antihelminthic drugs are primary treatment: Praziquantel is moderately effective for clonorchiasis (20% cure rate with single dose), albendazole is very effective for ascariasis, and triclabendazole is very effective for fascioliasis


 in the main pancreatic duct. Pancreatic duct involvement is much less common than biliary invasion, likely because of the relatively small caliber of the pancreatic duct. Ascariasis-induced pancreatitis is due to either invasion of the pancreatic or biliary ducts.
in the main pancreatic duct. Pancreatic duct involvement is much less common than biliary invasion, likely because of the relatively small caliber of the pancreatic duct. Ascariasis-induced pancreatitis is due to either invasion of the pancreatic or biliary ducts.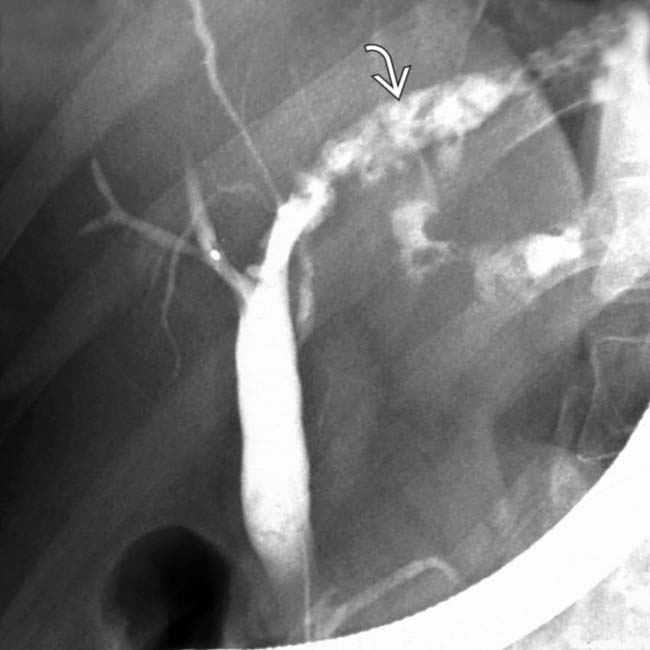
 and filling defects from intrahepatic flukes. The elongated configuration of the defects suggests flukes rather than intrahepatic biliary calculi.
and filling defects from intrahepatic flukes. The elongated configuration of the defects suggests flukes rather than intrahepatic biliary calculi.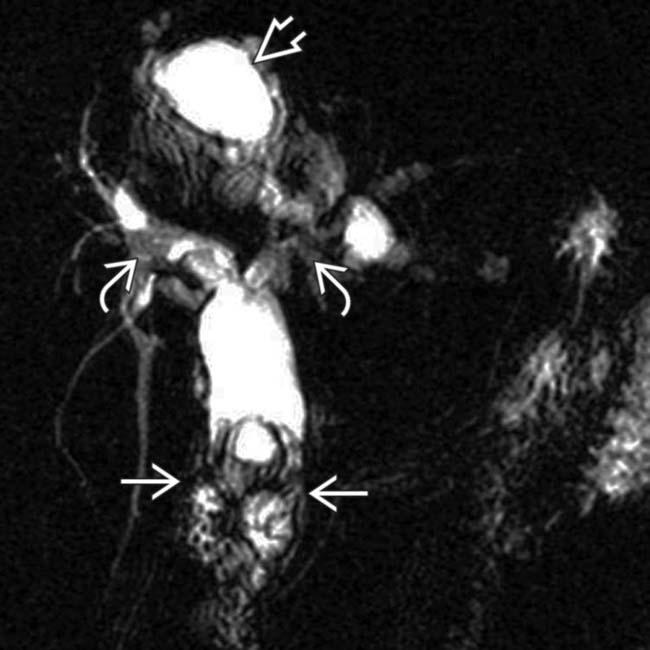
 , irregular right and left hepatic ducts
, irregular right and left hepatic ducts  , and an adjacent hydatid cyst
, and an adjacent hydatid cyst  . (Courtesy A. Dasyam, MD.)
. (Courtesy A. Dasyam, MD.)
 , biliary ductal dilatation, and communication with a partially opacified, ruptured hydatid cyst
, biliary ductal dilatation, and communication with a partially opacified, ruptured hydatid cyst  . Stents may relieve biliary obstruction, but surgical resection of the cyst is ultimately needed. (Courtesy A. Dasyam, MD.)
. Stents may relieve biliary obstruction, but surgical resection of the cyst is ultimately needed. (Courtesy A. Dasyam, MD.)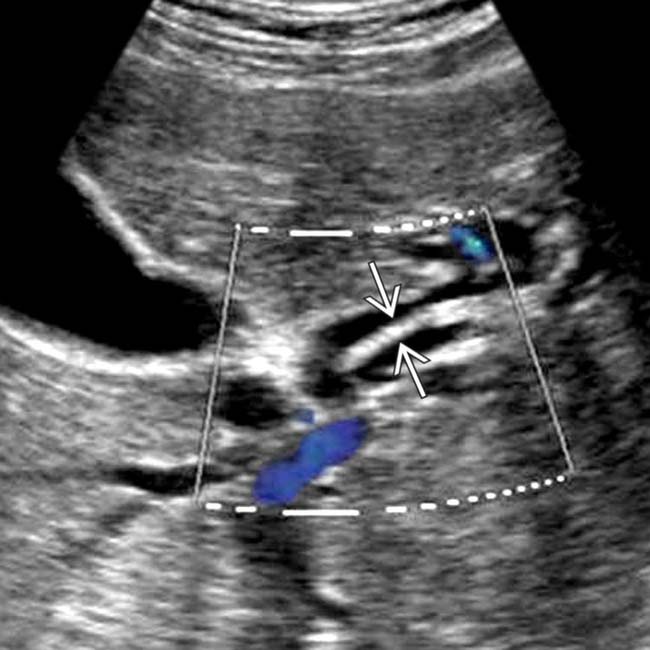
 within a dilated left bile duct representing a worm. (Courtesy A. Dasyam, MD.)
within a dilated left bile duct representing a worm. (Courtesy A. Dasyam, MD.)
 . The distal duct filling defect
. The distal duct filling defect  was ultimately shown to be cholangiocarcinoma, a known complication of ascariasis. (Courtesy A. Dasyam, MD.)
was ultimately shown to be cholangiocarcinoma, a known complication of ascariasis. (Courtesy A. Dasyam, MD.)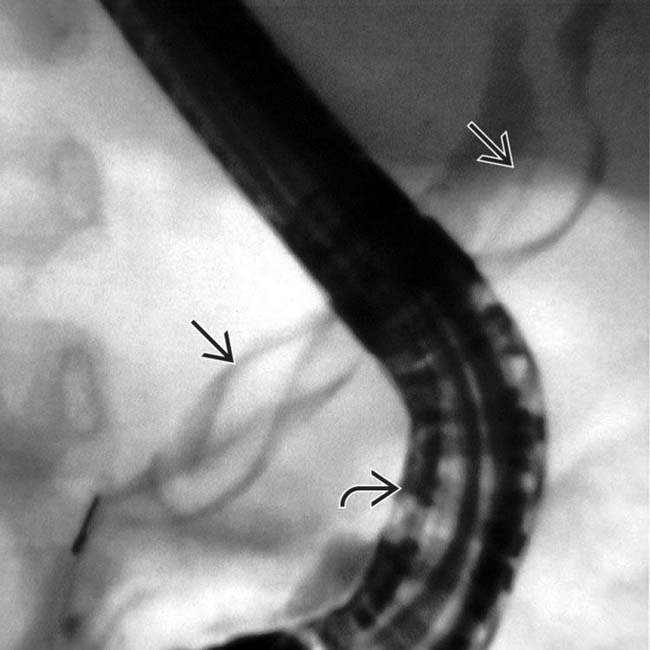
 , which represents the adult worm lodged in the common bile duct. Note the overlying endoscope
, which represents the adult worm lodged in the common bile duct. Note the overlying endoscope  .
.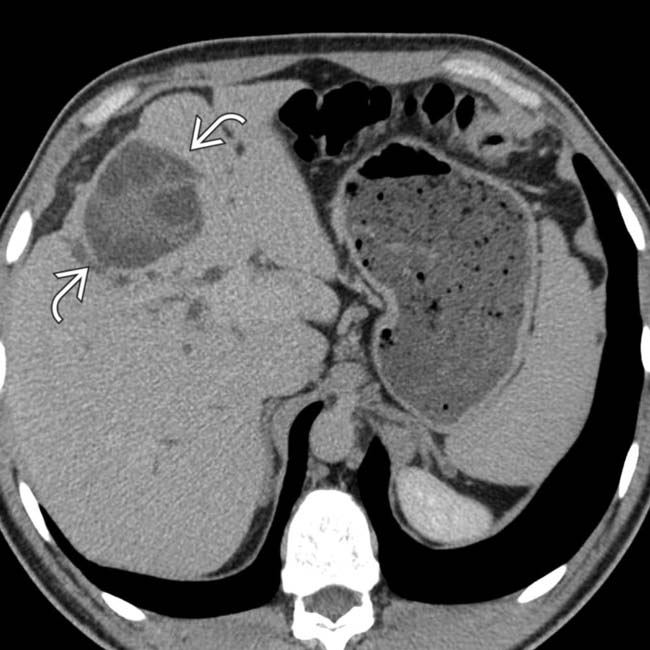
 within the medial segment and mild intrahepatic biliary ductal dilatation.
within the medial segment and mild intrahepatic biliary ductal dilatation.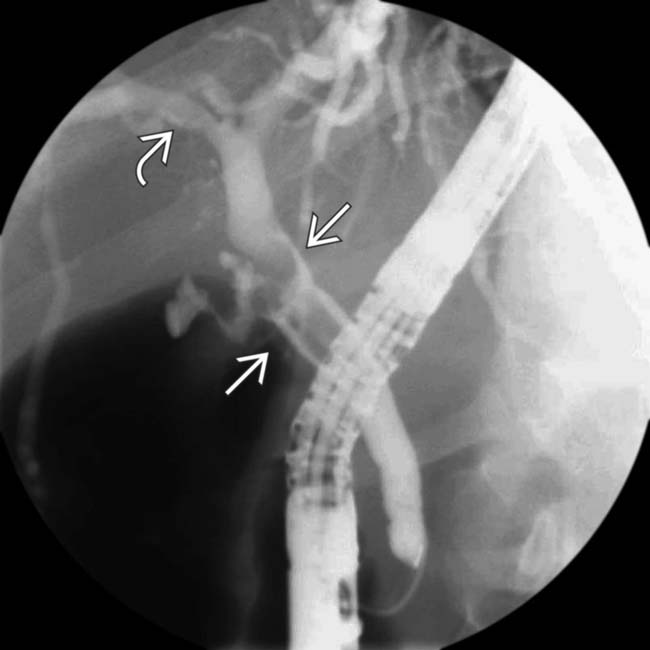
 and proximal right duct
and proximal right duct  . (Courtesy M. Harisinghani, MD.)
. (Courtesy M. Harisinghani, MD.)
 .
.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] CT: Linear high-density foci within dilated biliary tree
US: Tubular echogenic structure, 3-6 mm in diameter, with central anechoic area (digestive tract of worm)• Clonorchiasis: Flukes typically involve peripheral intrahepatic ducts, not GB, CBD, or PD
• Fascioliasis: Flukes usually involve large intrahepatic ducts, extrahepatic duct, and GB (after liver involvement)
• Echinococcosis: Communication of hepatic hydatid cyst with small biliary radicles or rupture of cyst into bile ducts
from a biliary Ascaris worm.. The worm was mobile at real-time examination. Central hypoechogenicity is thought to represent the digestive tract of the worm. (Courtesy A. Dasyam, MD.)IMAGING
General Features
• Best diagnostic clue
CT Findings
• Ascariasis/clonorchiasis: Intraductal high-density foci within dilated biliary tree due to biliary worms/flukes or debris
MR Findings
• Clonorchiasis: Preferential peripheral biliary dilatation with low-signal filling defects on T2WI or MRCP
Ultrasonographic Findings
• Grayscale ultrasound
Ascariasis: Ultrasound very sensitive for worms in biliary system, but insensitive for worms in duodenum or ampulla (sensitivity for pancreatobiliary ascariasis only 50%)
Ascariasis: Ultrasound very sensitive for worms in biliary system, but insensitive for worms in duodenum or ampulla (sensitivity for pancreatobiliary ascariasis only 50%)
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
