[level-membership-for-radiology-category] Only 50% of hepatic angiomyolipomas have substantial fat component
• Arterial phase: Prominent enhancement of nonfatty portion of lesion
Central vessels within lesion if mass is large
• Fatty component of tumor results in hyperintense (high signal) foci on T1WI and T2WI
• MR, fat suppression ± opposed-phase GRE imaging
TOP DIFFERENTIAL DIAGNOSES
• Hepatocellular carcinoma
• Postoperative state, liver
• Focal steatosis
• Hepatic adenoma
• Hepatic lipoma
• Metastases
Teratoma or liposarcoma
PATHOLOGY
• Associated with tuberous sclerosis in < 10% of cases
But some patients likely have forme fruste tuberous sclerosis
DIAGNOSTIC CHECKLIST
• Small, fat density hepatic mass in patient with tuberous sclerosis is almost certainly benign
• Angiomyolipoma that is primarily myeloid or angioid may be indistinguishable from other hepatic tumors, including hepatocellular carcinoma
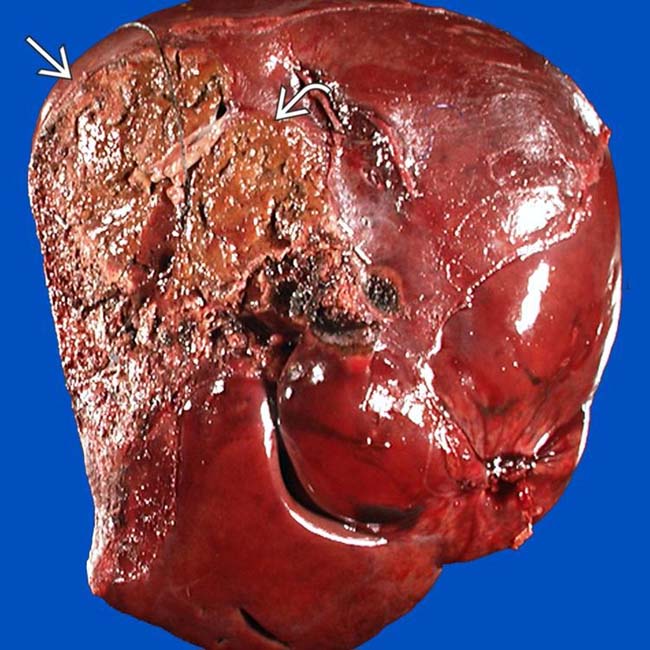
(Left) Gross photograph of a fixed specimen shows a heterogeneous mottled tan, yellow, and brown tumor with areas of hemorrhage and degeneration . Note that the background liver is not cirrhotic. (Courtesy J. Misdraji, MD.)
(Right) H&E-stained section shows a tumor composed of 3 elements: Adipose tissue , vessels , and plump spindle cells . (Courtesy J. Misdraji, MD.)
(Left) Axial T2WI MR shows a heterogeneously bright mass with a fatty component that is nearly isointense to subcutaneous fat . The rest of the tumor has the moderate hyperintensity typical of most neoplasms on T2WI MR.
(Right) Axial T1WI MR in the same patient shows that most of the mass is hyperintense, an unusual feature of most neoplasms and generally indicative of the presence of fat or hemorrhage within the mass. This tumor was resected and proved to be an isolated angiomyolipoma (AML).
TERMINOLOGY
Abbreviations
• Hepatic angiomyolipoma (AML)
Synonyms
• Benign hepatic hamartoma
Definitions
• Benign mesenchymal tumor composed of variable amounts of smooth muscle (myoid), fat (lipoid), and proliferating blood vessel (angioid) components
IMAGING
General Features
• Best diagnostic clue
Well-circumscribed, mostly fatty mass in liver
• Location
Liver is 2nd most common site (kidney is 1st)
• Size
Variable; 0.3-36 cm in diameter
• Key concepts
Round or lobulated solitary mass or multiple lesions with variable shape
Only 50% of hepatic angiomyolipomas have substantial fat component
– Those without much fat are difficult to distinguish from other hepatic tumors
CT Findings
• NECT
Well-defined mass with heterogeneous attenuation values due to presence of fat and soft tissue densities
– May be almost completely fat or soft tissue density mass
• CECT
Arterial phase: Prominent enhancement of nonfatty portion of lesion
Portal phase: Lesion shows hypoattenuation throughout mass
• CTA
Central vessels within lesion if mass is large
MR Findings
• T1WI
Hypointensity or hyperintensity on T1WI
– Depends on amount of fat and whether fat-suppressed technique is used
Fatty component of tumor results in hyperintense (high signal) foci on T1WI
Relative loss of signal intensity on opposed-phase images compared with in-phase
Frequency-selective fat-saturation techniques are useful
• T2WI
High signal intensity of fatty components
Heterogeneous hyperintensity
• T1WI C+
Enhancement of soft tissue elements within lesion
Ultrasonographic Findings
• Grayscale ultrasound
Homogeneous or heterogeneous echogenic mass due to fat
If muscle, vascular elements, or hemorrhage predominate, lesion may be hypoechoic
Angiographic Findings
• Heterogeneously hypervascular tumor
Imaging Recommendations
• Best imaging tool
MR with fat suppression ± opposed-phase GRE imaging
DIFFERENTIAL DIAGNOSIS
Hepatocellular Carcinoma (HCC)
• Fat within tumor may be localized or show diffusely scattered or mosaic pattern
• Fat-containing mass in cirrhotic liver is usually HCC
Postoperative State, Liver
• Omental fat may be placed into surgical defect in liver
Focal Steatosis
• Often periligamentous or periportal distribution
• Shows normal blood vessels traversing lesion
Hepatic Adenoma
• Well defined, often surrounded by capsule
• Heterogeneously hypervascular; areas of hemorrhage and fat within
• Typically seen in young women who take oral contraceptives
Hepatic Lipoma
• No enhancement on CECT (indistinguishable from AML with mostly fat content)
Metastases (Teratoma or Liposarcoma)
• Fat containing, ± fluid, calcification in teratoma
• Most liposarcomas are large, well-circumscribed, vascular structures with soft tissue attenuation
PATHOLOGY
General Features
• Associated abnormalities
Associated with tuberous sclerosis (TS) in < 10% of cases
– AMLs (+ cysts) in kidneys, plus extrarenal masses
– Some patients likely have forme fruste of TS
Gross Pathologic & Surgical Features
• Fat content varies from < 10% to > 90% of tumor volume
• Usually yellow to light tan, secondary to fat content
• May have large foci of necrosis
Microscopic Features
• Epithelioid smooth muscle cells, admixture of mature fat cells, and proliferating blood vessels
CLINICAL ISSUES
Presentation
• Asymptomatic and discovered incidentally at imaging
• Pain results from intratumoral hemorrhage (rare)
Demographics
• Gender
Marked female predominance
Natural History & Prognosis
• Spontaneous hemorrhage or rupture (rare)
• No malignant potential
Treatment
• Conservative; embolization
Resect large peripheral lesions and those of uncertain histology
DIAGNOSTIC CHECKLIST
Consider
• Small, fat density hepatic mass in patient with TS is likely benign
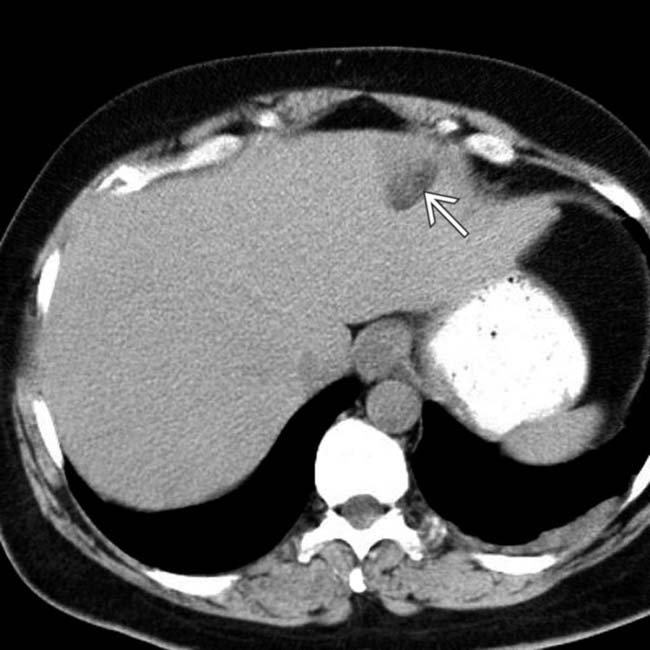
(Left) Axial NECT of a 56-year-old man who presented with nonspecific symptoms and no clinical evidence of tuberous sclerosis shows 1 of several partially fat-density masses in the liver.
(Right) Axial NECT of the same patient shows a fat-density mass and simple cysts in the kidneys.
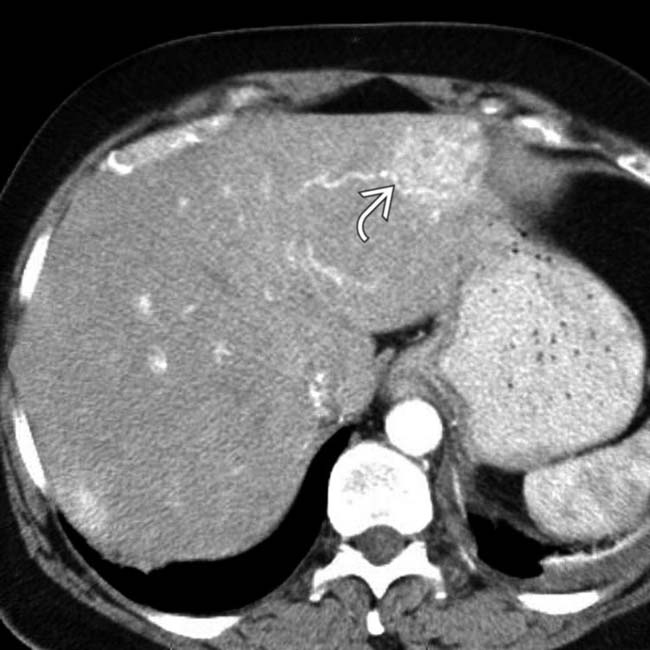
(Left) Axial CECT of the same patient shows bright enhancement of a portion of the hepatic mass that has other components measuring fat density .
(Right) Axial CECT of the same patient shows that most of the hepatic mass is hypervascular with large feeding vessels .
(Left) Axial CECT of the same patient shows a renal mass that is also characterized by large vessels and macroscopic fat, which are characteristic features of AML. This patient probably has a forme fruste of tuberous sclerosis with incomplete or atypical clinical manifestations.
(Right) H&E-stained section shows epithelioid smooth muscle cells with a rarefied cytoplasm that resembles “spider webs.” Note the enlarged oval nuclei and distinct nucleoli . (Courtesy J. Misdraji, MD.)
(Left) Axial CECT of a 36-year-old woman with tuberous sclerosis (TS) shows 2 nodules within the liver. One of them has the fat-density characteristic of AML, but the other is of soft tissue density likely representing lipid-poor AML.
(Right) Axial CECT of the same patient shows that the right kidney is absent (removed due to spontaneous hemorrhage from an AML). The left kidney is distorted by multiple fat-containing AMLs . This patient also had lymphangiomyomatosis of the lungs, another feature of the TS complex.
(Left) This 43-year-old woman had vague RUQ discomfort. Axial NECT shows a large hepatic mass with small foci of fat density .
(Right) Axial CECT in the same patient shows marked hypervascularity of the tumor, raising concern for hepatic adenoma or a malignant tumor. The mass was resected and proved to be an AML with predominantly smooth muscle and vascular components.
(Left) The resected specimen in this case is a large mass that had small foci of fat, large blood vessels, and areas of necrosis .
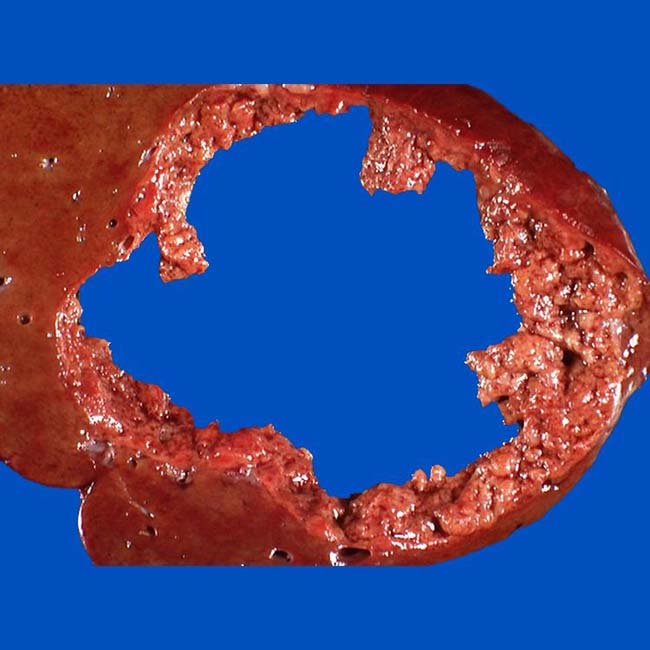
(Right) The bivalved resected specimen was a large mass, the center of which had become necrotic and “shelled out” on cross sectioning. The final diagnosis was hepatic AML.



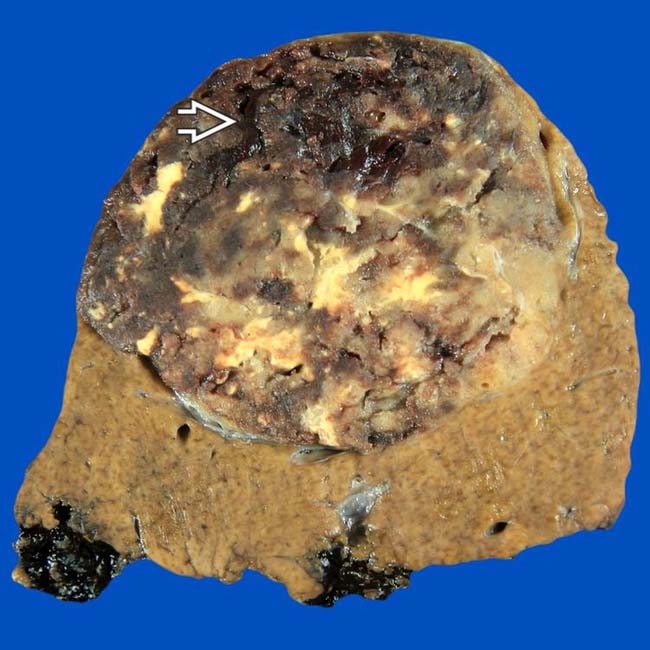
 . Note that the background liver is not cirrhotic. (Courtesy J. Misdraji, MD.)
. Note that the background liver is not cirrhotic. (Courtesy J. Misdraji, MD.)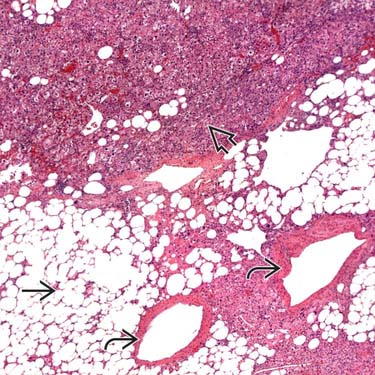
 , vessels
, vessels  , and plump spindle cells
, and plump spindle cells  . (Courtesy J. Misdraji, MD.)
. (Courtesy J. Misdraji, MD.)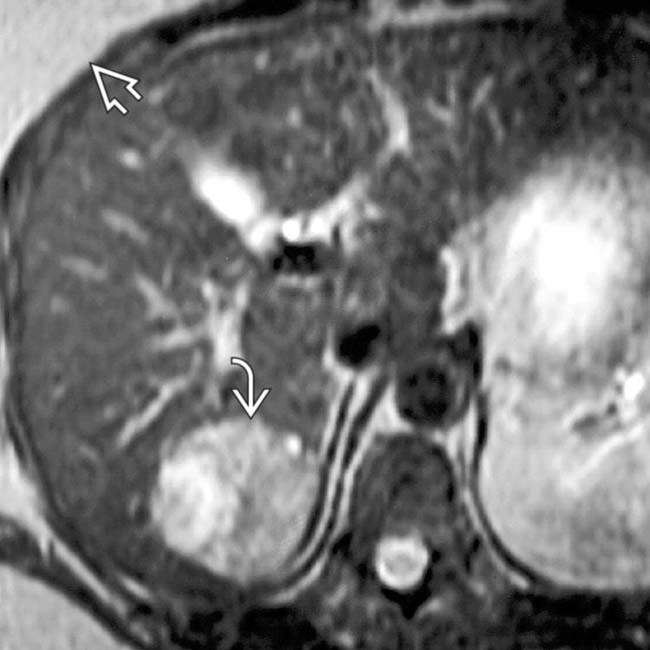
 that is nearly isointense to subcutaneous fat
that is nearly isointense to subcutaneous fat  . The rest of the tumor has the moderate hyperintensity typical of most neoplasms on T2WI MR.
. The rest of the tumor has the moderate hyperintensity typical of most neoplasms on T2WI MR.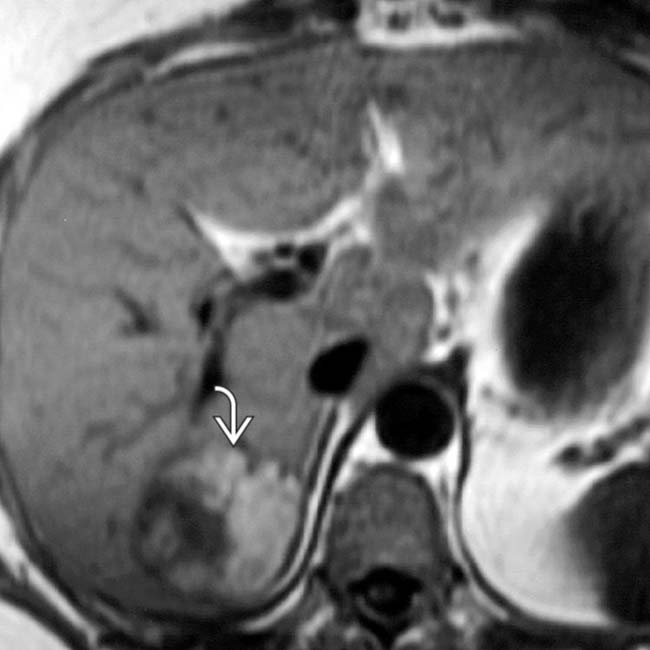
 is hyperintense, an unusual feature of most neoplasms and generally indicative of the presence of fat or hemorrhage within the mass. This tumor was resected and proved to be an isolated angiomyolipoma (AML).
is hyperintense, an unusual feature of most neoplasms and generally indicative of the presence of fat or hemorrhage within the mass. This tumor was resected and proved to be an isolated angiomyolipoma (AML).





















 partially fat-density masses in the liver.
partially fat-density masses in the liver.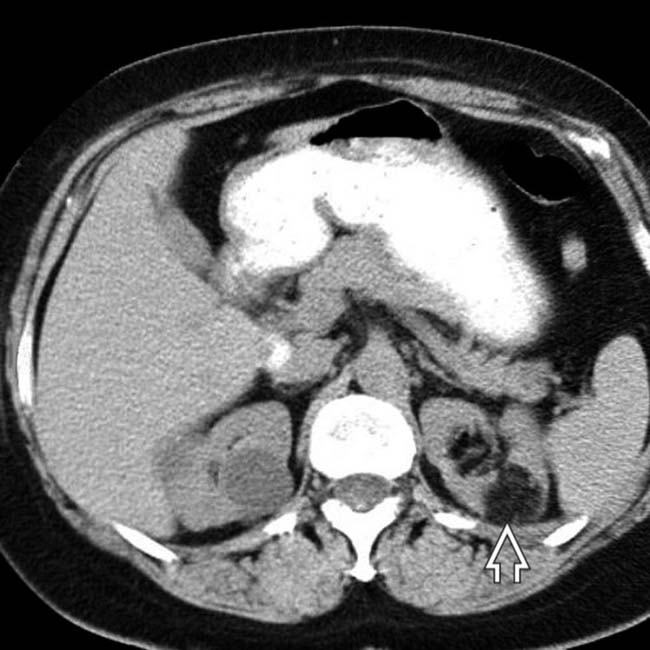
 and simple cysts in the kidneys.
and simple cysts in the kidneys.
 that has other components measuring fat density
that has other components measuring fat density  .
.
 .
.
 that is also characterized by large vessels and macroscopic fat, which are characteristic features of AML. This patient probably has a forme fruste of tuberous sclerosis with incomplete or atypical clinical manifestations.
that is also characterized by large vessels and macroscopic fat, which are characteristic features of AML. This patient probably has a forme fruste of tuberous sclerosis with incomplete or atypical clinical manifestations.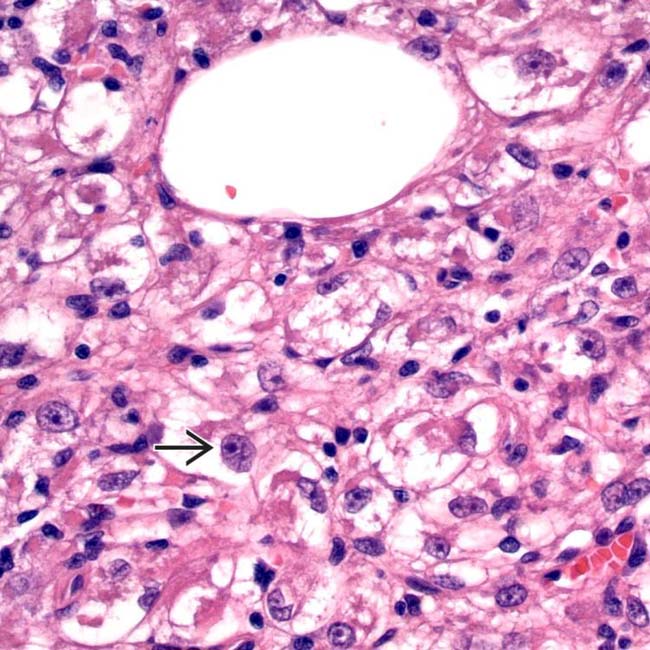
 . (Courtesy J. Misdraji, MD.)
. (Courtesy J. Misdraji, MD.)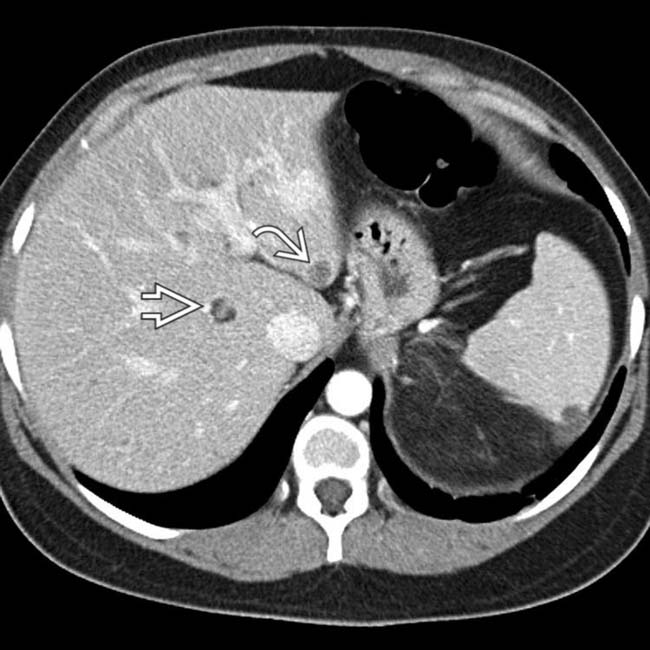
 characteristic of AML, but the other is of soft tissue density
characteristic of AML, but the other is of soft tissue density  likely representing lipid-poor AML.
likely representing lipid-poor AML.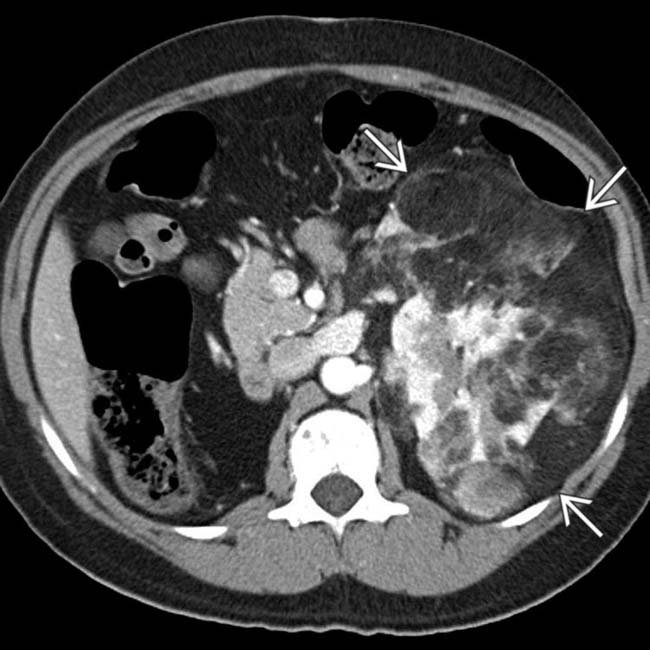
 . This patient also had lymphangiomyomatosis of the lungs, another feature of the TS complex.
. This patient also had lymphangiomyomatosis of the lungs, another feature of the TS complex.
 .
.
 that had small foci of fat, large blood vessels, and areas of necrosis
that had small foci of fat, large blood vessels, and areas of necrosis  .
.