[level-membership-for-emergency-medicine-category]
5.9 Cardiac Arrhythmias
Normal conduction system
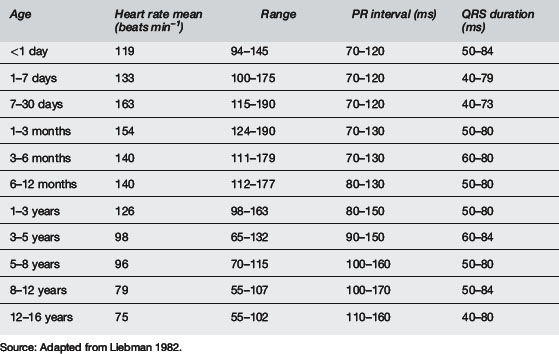
The SA node is normally the dominant (fastest) cardiac pacemaker but this can change if sinus node dysfunction occurs or if other parts of the conduction system develop increased automaticity. As stated above, the SA node is located near the junction of the superior vena cava (SVC) and the right atrium. The SA node is innervated by both sympathetic and parasympathetic nerve endings. Parasympathetic tone predominates during rest. Children are known to have relatively greater parasympathetic tone than adults and are also known to have developmental and age-dependent differences in action potential amplitude and conduction speed. Accordingly, there are age-dependent normal values for resting heart rate as well as PR interval and QRS duration, in addition to many other electrophysiology parameters (see Table 5.9.1).
The cardiac action potential
The cardiac action potential is divided into five phases: 0, 1, 2, 3, 4.
Pathogenesis of arrhythmias





General principles for arrhythmia management



Sinus bradycardia





Conduction disturbances: atrioventricular block









Alexander M.E., Berul C.I. Ventricular arrhythmias: When to worry. Pediatr Cardiol. 2000;21(6):532-541.
Anonymous. The International Liason Committee on Resuscitation (ILCOR) consensus on science with treatment recommendations for paediatric and neonatal patients: paediatric basic and advanced life support. Pediatrics. 2006;117(5):e955-e977.
Bink-Boelkens M.T.E. Pharmacologic management of arrhythmias. Pediatr Cardiol. 2000;21(6):508-515.
Celiker A., Ayabakan C., Ozer S., et al. Sotalol in the treatment of pediatric cardiac arrhythmias. Pediatr Int. 2001;43:624-630.
Chun T.U., Dehart G.F. Advances in the approach to treatment of supraventricular tachycardia in the pediatric population. Curr Cardiol Rep. 2004;6:322-326.
Kudenchuk P.J., Cobb L.A., Copass M.K., et al. Amiodarone for resuscitation after out-of-hospital cardiac arrest due to ventricular fibrillation. N Engl J Med. 1999;341(12):871-878.
Liebman J. Tables of normal standards. In: Liebman J., Plonsey R., Gillette P.C., editors. Pediatric electrocardiography. 1st ed. Baltimore: Williams & Wilkins; 1982:82-133.
Luedtke S.A., Kuhn R.J., McCaffrey F.M. Pharmacologic management of supraventricular tachycardias in children. Part 1, WPW and AV nodal re-entry. Ann Pharmacother. 1997;31:1227-1243.
Luedtke S.A., Kuhn R.J., McCaffrey F.M. Pharmacologic management of supraventricular tachycardias in children. Part 2, Atrial flutter, atrial fibrillation and junctional and atrial ectopic tachycardia. Ann Pharmacother. 1997;31:1347-1359.
McKee M.R. Amiodarone – an ‘old’ drug with new recommendations. Curr Opin Pediatr. 2004;15:193-199.
Saul J.P., Scott W.A., Brown S., et al. Intravenous amiodarone for incessant tachyarrhythmias in children: a randomized, double-blind, antiarrhythmia drug trial. Circulation. 2005;112:3470-3477.
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
5.9 Cardiac Arrhythmias
Normal conduction system
The SA node is normally the dominant (fastest) cardiac pacemaker but this can change if sinus node dysfunction occurs or if other parts of the conduction system develop increased automaticity. As stated above, the SA node is located near the junction of the superior vena cava (SVC) and the right atrium. The SA node is innervated by both sympathetic and parasympathetic nerve endings. Parasympathetic tone predominates during rest. Children are known to have relatively greater parasympathetic tone than adults and are also known to have developmental and age-dependent differences in action potential amplitude and conduction speed. Accordingly, there are age-dependent normal values for resting heart rate as well as PR interval and QRS duration, in addition to many other electrophysiology parameters (see Table 5.9.1).
The cardiac action potential
The cardiac action potential is divided into five phases: 0, 1, 2, 3, 4.
