CHAPTER 6. Patients’ rights to and in health care
L earning objectives
▪ Discuss the relationship between patients’/clients’ rights and moral rights.
▪ Consider the right to health and health care and:
• discuss the right to health
• discuss the right to health care and at least four senses in which it can be claimed
• outline some controversial arguments raised both for and against the right to health care
• explain why an economic framework is morally inadequate for deciding issues of health care justice.
▪ Consider the right to make informed choices and:
• outline the doctrine of informed consent
• explore the notion of the ‘sovereignty of the individual’ and its implications for informed consent practices
• examine critically the five analytical components of informed consent
• discuss critically at least five common objections raised against the right to give an informed consent
• discuss critically the right of competent patients to refuse nursing care.
▪ Examine the notion of competency and its implications for patients with impaired decision-making capacity.
▪ Discuss critically the notion of ‘surrogate decision-making’ in the case of rational incompetence.
▪ Discuss the nature and moral implications of paternalism in nursing and health care.
▪ Consider the right to confidentiality and:
• state the International Council of Nurses’ position on confidentiality
• outline the moral basis and requirements of the principle of confidentiality
• discuss briefly the conditions under which demands to keep information confidential may be justly overridden.
▪ Discuss critically the right to dignity.
▪ Discuss critically the right to be treated with respect.
▪ Discuss critically the right to cultural liberty.
I ntroduction
In 1996, in what has been described by media commentators as ‘the first case of its kind’ in North America, a patient sued his treating physician for ‘keeping him alive’ against his expressed wishes and for not offering him an ‘elective demise’ (Reed 1996: 14). The patient in this case was a 66-year-old man who had been diagnosed with amyotrophic lateral sclerosis, a degenerative nerve disorder. Despite having made a ‘living will’ that clearly stated his wishes ‘not to be attached to a respirator’ should his condition deteriorate, the patient was nevertheless placed on an artificial life-support machine when he began experiencing breathing difficulties. As a result of this paternalistic medical decision, he was left totally dependent on 24-hour nursing care, depleted of his life-savings, and deprived of what he regarded as a ‘dignified death’ (Reed 1996: 14). The patient’s life expectancy was estimated at the time of the report to be 5–10 years.
A little over 1 year later, in New Zealand, a case of a very different kind unfolded. In this case, Rau Williams, a 63-year-old Maori man with early stage dementia and suffering a complication of diabetes, was denied kidney dialysis treatment on ‘economic grounds’ (Field 1997: 10). In keeping with national resource allocation guidelines in operation at the time, clinicians concluded that, since Mr Williams was unable to ‘co-operate with active therapy’ (he was unable to perform home dialysis independently), was unable to live independently (even though his family were willing to supervise him), and was not expected to derive more than 1 year of life benefit from dialysis, he was ‘unsuitable for entry on to the [dialysis] program’ (Manning & Paterson 2005: 686–7).
Outraged by the hospital’s decision not to treat their father, and in a desperate bid to secure life-saving treatment for him, Rau William’s family applied to the New Zealand Court of Appeal to intervene. The patient’s evidence was that he did not want to die, and enjoyed some quality of life while on dialysis ‘including pleasure from seeing his family’ (Manning & Paterson 2005: 687). The court determined, however, that the hospital managers ‘did not need to resume kidney dialysis treatment’ (Field 1997: 10). In reaching its decision, the court took the stance that it would be ‘inappropriate for the Court to attempt to direct a doctor as to what treatment should be given to a patient’ (Manning & Paterson 2005: 687). This decision reflected two issues:
first, a recognition that clinical judgment is beyond the expertise of the courts; and secondly, that a court should not make orders with consequences for the utilization of scarce resources since it lacks knowledge of the competing claims to those resources.
(Manning & Paterson 2005: 687)
In response to the case, the then associate Health Minister was reported to have said that ‘health rationing was now a fact of life’. It was subsequently observed that:
Although formal rationing has not previously been acknowledged here [New Zealand], from July every New Zealander referred for surgery in the public health system will be scored for points on clinical and social criteria to determine when they will be treated.
(Field 1997: 10)
Today, in New Zealand, there are no guarantees of access to publicly funded ‘none-core’ health services (Manning & Paterson 2005). Moreover, exclusions from even ‘core treatments’ on the grounds of age and disability are legally justified ‘provided there is an objective, evidential basis to justify [the] exclusions’ (Flood et al 2005: 638; see also Manning & Paterson 2005). The stance taken by New Zealand officials on this issue has earned them a reputation among some international experts as being ‘among the “leading bunch” in the move to explicit rationing’ (Manning & Paterson 2005: 683). Although politicians and health officials prefer to use the term ‘prioritising access’ to health care (rather than ‘rationalising’ or ‘limiting’ access to it), ‘justified discrimination’ in health care has become a poignant reality for New Zealanders (Flood et al 2005: 638; Manning & Paterson 2005).
In 2002, a major Australian newspaper reported on the assault and substandard care of an 87-year-old woman in a state government-run aged care facility (Miller 2002). The report stated that the woman was allegedly assaulted (by another resident) on at least four occasions, found smeared with faeces a number of times, and had had at least six falls resulting in injuries. The woman’s daughter is reported as also alleging that ‘some of the ward emergency buzzers were broken, the toilets were often found in a disgraceful condition’ and that she had seen ‘rats and mice on the ground floor of the aged care centre’ (Miller 2002: 3). The daughter is also reported as stating that ‘for months she complied with the hospital’s internal complaints procedures but abandoned it “when it proved itself to be a futile process” ’ (Miller 2002: 3).
These reports on treating patients against their will, denying patients life-saving treatment for economic reasons, and the provision of substandard care are just some among many examples of patients’ rights violations that can and do occur in health care contexts. Other examples of patients’ rights violations include: breaches of confidentiality, inadequate consent practices, not being treated with respect, and being stigmatised and discriminated against in health injurious and harmful ways. It is to examining patients’ rights and their implications for members of the nursing profession that this and the following chapters now turn.
T he issue of patients’ rights
People requiring or receiving health care are not, and never have been, obliged to be the passive recipients of unnegotiated care. Yet the more we examine the realities of health care practice and the way our health care institutions and services operate, the more apparent it becomes that the rhetoric surrounding the idealism of people’s rights to and in health care does not always match the reality. As the bioethics, legal, professional and lay literature, and our own everyday experience, make plain, people continue to be denied equitable access to both the quantity and quality of health care they need; they continue to be denied the opportunity to make informed choices about their care and treatment options; and they continue to be harmed physically, psychologically, spiritually and morally as a result of morally questionable practices in our health care services and institutions.
Over the past three decades, the issue of patients’ rights has received considerable attention both in Australia and overseas. There exists a vast body of literature on the subject (too numerous to list here), and there has been a proliferation of dramatised accounts of people’s ‘life stories’ on the matter both in books and films. There have also been significant policy and law reforms in the area of patients’ rights, for instance, in relation to:
▪ clarifying people’s common law right to refuse orthodox medical treatment
▪ the lawful appointment of ‘surrogate decision-makers’ (e.g. persons with medical power of attorney) in the case of patients who become incompetent to decide their own medical treatment options
▪ formulating ‘living wills’
▪ the right to an ‘assisted death’
▪ the establishment of clinical ethics committees (CECs) and ‘client support’ persons
▪ the establishment of statutory health services complaints mechanisms
▪ the role of a public advocate in the case of disagreement about treatment decisions
▪ the development of public consumer advocacy groups
▪ the establishment of national ethics committees and commissions.
Despite these important innovations, however, the area of patients’ rights remains problematic.
There is no denying that enormous progress has been made over the past three decades in regard to patients’ rights: violations are monitored more carefully; redress of violations is more substantial; and more effort is now being put into preventing patients’ rights violations from occurring (notably under the rubric of corporate risk/clinical risk management). Nevertheless it is evident that we still have a long way to go in order to ensure that the rights of patients are properly respected and protected in health care domains: dispute remains about who has rights to and in health care; there are disagreements about what rights patients can meaningfully and reasonably claim in certain contexts; there is a lack of certainty about who has corresponding duties to patients’ rights claims; and there is no consensus on how best to resolve disputes in cases where patients’ rights claims compete and conflict — particularly in contexts of diminished health care resources. Important questions remain of: How and what can we learn about the disputes and disagreements that remain concerning patients’ rights? How might we prevent patients’ rights from being violated in the domains in which we work? and How do those who have violated patients’ rights, and the patients whose rights have been violated, come to terms with the aftermath of those violations?
In 1990, the Consumers’ Health Forum (CHF) pointed out that the Australian legal system had not been responsive to protecting the needs of health care consumers. In its report on the Legal Recognition and Protection of the Rights of Health Consumers, CHF states (pp 1–2):
For some consumers the diversity of the Australian legal system has provided some benefits. Unfortunately, for the majority it has been far more effective in creating an inequitable and unresponsive legal maze. As it currently stands:
– there is no clear direction for consumers as to how they should act, how others should act, and what redress they have if things go wrong (their rights depend upon which State consumers live in or even whether they attend a public or private health facility); and
– the interests of bureaucrats and professional groups are better reflected in existing law than the interests of consumers and the community in such matters as information, participation, accountability and openness.
At the time of writing, these issues remain in need of attention. Although health law and ‘therapeutic jurisprudence’ are being increasingly recognised as a foremost area of legal practice, discourse and research in Australia, questions remain ‘about the legitimacy and coherence of health law’ and its ultimate impact on the health interests of individual consumers and communities alike (Freckelton & Petersen 2006: 3). In the case of the legitimating individual and community health as a fundamental objective, for instance, Australian courts, like their overseas counterparts, are generally reluctant to affirm a positive right to health care (Flood et al 2005). Although human rights discourse in Australian law is gaining increasing importance ‘in relation to matters of life, death and health’ (Freckelton 2006), its commitment to affirming consumers’ positive right to health care is at best dubious.
It can be seen then that the issue of patients’ (clients’) rights is of obvious importance to the nursing profession. If nurses are to respond effectively to this issue, however, they need to have knowledge and understanding of, first, what patients’ rights are, and second, how these rights can best be upheld. It is to advancing an understanding of these matters that this discussion will now turn.
W hat are patients’ rights?
To put it simply, patients’ or clients’ rights are a subcategory of human rights. Statements of patients’ or clients’ rights are merely statements about particular moral interests that a person might have in health care contexts and that require special protection when a person assumes the role of a patient or client. Referring to this particular set of interests in terms of ‘patients’ rights’ or ‘clients’ rights’ serves more the purposes of manageability than those of philosophy. For example, when the notion patients’ rights or clients’ rights is used, we know immediately what kind of context and what kind of rights claims are likely to be encountered. The notion of patients’ rights or clients’ rights in this instance immediately ‘sets the scene’, or identifies the domain of concern. In the case of human rights language, the scene that is set is much broader. Some might consider human rights language in health care contexts to be somewhat cumbersome to manage. This is not to say that it would be inappropriate to use the notion of human rights in health care contexts; quite the reverse. In many respects, using human rights language might be more compelling and more effective in drawing attention to and commanding respect of the deserving moral interests of people in health care domains.
It is perhaps important to clarify that patients’ rights statements tend to include a mixture of civil rights, legal rights and moral rights. Popular examples of patients’ rights include: a right to health care, a right to be informed, a right to participate in decision-making concerning treatment and care, a right to give an informed consent, a right to refuse consent, a right to have access to a qualified health interpreter, a right to know the name, status and practice experience of attending health professionals, a right to a second medical opinion, a right to be treated with respect, a right to confidentiality, a right to bodily integrity, a right to the maintenance of dignity, and many others. Many of these rights statements derive from the broader moral principles of autonomy, non-maleficence, beneficence and justice, already discussed in this book. Unfortunately there is insufficient space here to discuss every type of patients’ right that has been formulated at some time or another. For the purposes of this discussion, attention is given to only six broad categories of rights, under which many other narrower rights claims fall. These category claims include the rights to health and health care, to make self-determining choices (informed consent), to confidentiality, to be treated with dignity, to be treated with respect and to cultural liberty.
T he right to health and health care
In keeping with the Universal Declaration of Human Rights, all people have a right to health. The World Health Organization (WHO 2002a) has clarified that the right to health does not entail the right to be healthy, but the right to the highest attainable standard of health, as articulated in General Comment 14 of article 12 of the United Nations’ International Covenant on Economic, Social and Cultural Rights (United Nations CESCR 2000). This, in turn, has been interpreted as requiring governments and public authorities to ‘put in place policies and action plans which will lead to available and accessible health care for all in the shortest possible time’ (WHO 2002a: 9).
The right to health and health care is complex and controversial. As well as being a sensitive moral issue, it is also a highly charged political issue, as ongoing debates on population health and health care resource allocation make plain (see, e.g. Daniels 2006; Dyck 2005; Powers & Faden 2006).
Bioethicists have yet to find a happy medium between the many competing and conflicting views on the subject. Some philosophers argue that health and health care is something all people are equally entitled to, regardless of the cost. Where human life is at stake, they contend, decisions about health and health care should not be constrained by economic considerations (Brody 1986; Powers & Faden 2006). Moreover, in keeping with what is known as the ‘rescue principle’ which imposes a duty on individuals and communities to ‘save and rescue human life’ and to ‘prevent and avoid illness, injuries, and violations of human rights generally’ (Dyck 2005: 280), it is ‘intolerable when a society allows people to die who could have been saved by spending more money on health care’ (Beauchamp & Childress 2001: 246). If more money is required, the solution is relatively simple: redirect society’s resources — for example, away from gross expenditures on arsenals of arms and other life-threatening instruments of war; and towards improving health promotion and illness-injury prevention programs and towards redressing existing inefficiencies in the system (Dyck 2005: 317–21). In addition, attention should be given to containing costs of needed medical care by containing the risks of medical malpractice litigation and the related high costs of insurance premiums that are being built into and hence adding to the costs of medical services (Dyck 2005: 317–18).
Others argue that it is implausible and impossible to ensure ‘good health’ and to provide a high standard of health care to all persons equally. In the case of health care, at best, all that people can reasonably claim is a ‘decent minimum’ of health care, as measured in terms of the amount necessary to secure a minimally decent or ‘tolerable’ life (Sreenivasan 2007; Engelhardt 1986: 336; Buchanan 1984; Fried 1982). Some theorists further argue that having access to only a ‘decent minimum’ of health care is particularly compelling when it is considered that, since social determinants are a more reliable precursor of health — and that having universal access to health care as such does not necessarily ensure health — the assumed ‘equal right to a high standard of health care’ is not only unsustainable, but lacks sound moral justification (Sreenivasan 2007). Still others argue that there is no such thing as a right to health care. One philosopher even claims that it is immoral to speak of health care as a ‘right’ (Sade 1983), and another that the expression ‘a right to health care’ is nothing but a ‘dangerous slogan’ (Fried 1982).
Charles Fried (1982: 400) claims that the ‘impossible dilemma posed by the promise of a right to health care’ is really nothing more than a product of ‘our culture’s inability to face and cope with the persistent facts of illness, old age, and death’. He goes on to assert provocatively that (p 400):
Because we are little able to come to terms with the hazards which illness proposes, because the old are a burden and an embarrassment, because we pretend that death does not exist, we employ elaborate ruses to put these things out of the ambit of our ordinary lives.
Whether the right to health and health care is a bogus claim or a dangerous slogan or a cultural quirk will, however, depend very much on how the notions of ‘health’ and ‘health care’ are interpreted. There is room to suggest that criticism of the right to health care derives from the erroneous equation of ‘health care’ with ‘medical care’. Since medical care makes up only a small proportion of overall health care, it is obviously not synonymous with health care. Moreover, as the vast body of literature on the social determinants of health make plain, even if medical care was the major form of health care, it would not necessarily guarantee ‘good health’ (Wilkinson & Marmot 2003; Sreenivasan 2007). Once the notions of ‘health’ and ‘health care’ are understood in more holistic terms, the right to these things may not seem so outrageous or fraudulent or even culturally odd as a claim. Every culture has its way of promoting health and preventing ill-health, of dealing with sickness, illness, pain and suffering, and of caring for the ill and injured. However, not every culture embraces Western scientific medicine as the most effective way of dealing with health, sickness and related illness experiences. And thus not every culture is posed with the dilemma of economic restrictions on resource allocation. Once health and health care, in their more holistic and socially determined sense, are seen as an important means of promoting a person’s total (and not merely physical) wellbeing, it becomes increasingly difficult to deny that claims to it are valid and morally justified.
What makes a claim to health and health care compelling is precisely that, once it is accepted, it has the moral power to prescribe actions to relieve the distressing symptoms caused by illness and injuries, to promote human wellbeing (a moral end) and, indeed, to promote human life itself (also a moral end) (Powers & Faden 2006; see also Dyck 2005, Chapter 11‘Justice and nurture: rescue and health care as rights and responsibilities’). If we deny entitlements to health and health care, we must also deny entitlements to a range of other interests, including those of life, happiness and even the exercise of self-determining choices.
It is beyond the scope of this text to deal with the many arguments and counter-arguments raised in response to the question of whether people have a right to health and health care. What is of concern here is to clarify the nature of the claim to a right to health and health care, and what might be meant by such a claim.
People’s entitlement to receive health and health care first received global recognition with the signing of the United Nations Universal Declaration of Human Rights on 10 December 1948. Article 25 states:
Everyone has the right to a standard of living adequate for the health and wellbeing of himself [sic] and his [sic] family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his [sic] control.
(United Nations 1978: 8)
It is worth noting here that the right to health and health care embodied by this statement extends far beyond a claim of mere medical care, and embraces a more holistic and socially determined interpretation of health and health care.
Since the signing of this declaration the question of the right to health and health care has taken on a new meaning, and has emerged largely as a result of what people perceive to be an ‘unjust or unfair state of affairs’ involving present structures of health and social care, which are seen as diminishing and even eliminating possibilities for the enhancement of the quality of human life and for human life itself (Powers & Faden 2006; Teays & Purdy 2001; McCullough 1983).
In speaking of the more specific right to health care, it is important to distinguish at least four different senses in which it can be claimed: that is, the right to equal access to health care; the right to have access to appropriate care; the right to quality care; and the right to safe care.
The right to equal access to health care
Access to health care refers to ‘whether people who are — or should be — entitled to health care services receive them’ (Emanuel 2000: 8). The right to equal access to health care raises questions of distributive justice and of how the benefits and burdens associated with health care service delivery ought to be distributed. It also raises questions of whether people or institutions can be found morally negligent for failing to provide equal access to health care for persons requiring it. Responses refuting this sense of a right to health care typically centre on such arguments as: ‘there is not a “bottomless pit” of health care resources, and somebody has to do without’.
Specifically, the ‘scarce resources, but unlimited wants’ argument tends to be constructed as follows:
1. the demand for health care has outstripped supply
2. this is fundamentally because health care resources are limited
3. different people have different health needs, and different views on how existing resources should be used to meet these needs
4. it is true that existing health care resources can be used in alternative ways
5. nevertheless, health care resources are limited, so it is not possible to satisfy everybody’s needs and wants (Beauchamp & Childress 2001; Dyck 2005; Teays & Purdy 2001).
The ultimate conclusion drawn from these premises — the ‘bottom line’, so to speak — is that, inevitably, choices will have to be made. In particular, borrowing from Sheehan and Wells (1985: 59), choices will have to be made about:
1. the conditions for which scarce resources should be made available
2. the priority with which given conditions should be treated.
It remains an open question, however, whether we have to accept the premises of this ‘scarce resources, but unlimited wants’ argument and, further, whether we have to accept its apparent ‘inevitable’ conclusions. It is far from clear that we do have to accept them — particularly when the politics of health and health care resource allocation are considered fully, including the vested and powerful interests that the whole health and health care economics debate is serving. Further, it is also open to serious question whether we are obliged to accept that economic principles ought to supplant morality as the ultimate test of conduct, as an economic rationalisation approach to health care dictates. Human life is not something that can be reduced, like an object, to mere economic worth, and as moral beings we ought to resist attempts to do so; if we do not resist, we risk seeing ‘worthless’ human beings (increasingly characterised as ‘unproductive burdens on society’) denied the health care entitlements they would otherwise be entitled morally to receive.
It is important to recognise that the issue of resource allocation goes far beyond the simple question of merely how to allocate dollars and cents. It involves much broader questions of how to measure quality of life, efficacy of health care and medical treatment, and quality of care, and of how to calculate cost-effectiveness, as well as complex socio-cultural questions pertaining to power, politics and profit (see David Lindorff’s controversial and provocative text Marketplace medicine: the rise of the for-profit hospital chains [1992]). Fundamentally, it also involves questions of how best to promote health, not merely access to health care services in ‘bricks and mortar’ hospitals (Faden & Powers 2006; Johnstone 2002b; Teays & Purdy 2001; Emanuel 2000).
Unless nurses address these other broader questions — both academically and professionally — they will never be in a position to offer a convincing account of why health care (whatever form this may take), not merely hospital or medical care, needs to be better recognised and why it must be more appropriately resourced. A strong stand must be taken on the need to recognise and to fund the promotion of health better (not just health care services), and there is considerable scope to suggest that it would be appropriate for the nursing profession to lead such a stand (see also Christensen et al 2001). More than this, the nursing profession has a moral obligation to lobby effectively for the community as a whole, and the individuals who comprise it, to have better access to the processes that promote health, not merely to hospital or medical care and related services (Johnstone 2002b; Christensen et al 2001).
The right to have access to appropriate care
The right to have access to appropriate care is a second sense in which a right to health care can be claimed. This sense raises important questions concerning the cultural competency and cultural safety of care (see Department of Health and Human Services [DHHS] 2001a, 2001b; Johnstone & Kanitsaki 2007a, 2007b; Papadopoulos 2006) as well as its ability generally to accommodate people’s personal preferences, health beliefs, health values and health practices. As examples given in Chapter 4 of this book have already shown, failing to provide health care in a culturally appropriate, responsive and informed manner can have harmful consequences (clinically, legally and morally) (see also Johnstone & Kanitsaki 2006b; Smedley et al 2003). Other examples given throughout this book will lend further weight to claims that failure to provide people with access to appropriate care can result in otherwise preventable adverse outcomes for both patients and health service providers alike.
Many other examples can be given here. The complementary therapy movement, for instance, has posed all sorts of new dilemmas for the scientific health professional, particularly in instances where patients prefer to try scientifically ‘ unproven’ vitamin or herbal remedies, meditation and other ‘alternative’ therapeutic agents for serious diseases, rather than risk the known and unpleasant side effects of more orthodox medical treatments. To some extent this type of problem has been overcome on account of alternative therapies being better researched, and more widely accepted by health professionals. Today, it is not uncommon for patients to receive a combination of orthodox and unorthodox treatments (e.g. performing surgery as well as administering vitamin and herbal therapies, or administering orthodox drugs as well as performing spinal manipulation, acupuncture and acupressure, facilitating meditation, and the like).
Another aspect of ‘appropriate care’ entails patients having access to people (lay folk and professional) of their own choosing. It also includes patients’ entitlements to seek a second medical opinion, to refuse a recommended medical therapy or folk therapy, to choose an alternative health therapy, to be surrounded by family and friends, to have unrestricted visiting rights, and to decline to be ‘ordered’ to do anything they do not wish to do (including getting out of bed, having a shower every day, and taking prescribed medication). As the Australian Consumers’ Association (1988: 16) pointed out long ago, patients do not need a doctor’s or nurse’s ‘permission’ (to be distinguished here from advice) for anything!
If nurses are to respond to this sense of a right to health and health care, they need to gain knowledge and understanding of their patients’ health beliefs and health practices and to negotiate ways in which these can be accommodated and met appropriately.
The right to quality care
A right to quality care is the third sense in which the right to health care can be claimed. This sense raises questions concerning the accountability, responsibility and competency of health professionals and health care providers, and about the standard of care that is actually delivered. Not only are practical and technical skills at issue here, but also attitudinal factors such as a health care provider’s attitude towards patients as human beings with needs and interests, who are entitled to participate in decision-making concerning their care. A claim to receive quality care also raises questions concerning what should be done in the case of the ‘impaired professional’— that is, someone who functions below an otherwise acceptable professional standard.
Quality health care as a right is an ambiguous and complex notion. Nevertheless, an attempt must be made to understand and use it in a meaningful way. This can be achieved by appealing to the agreed standards of the profession, experience, commonsense (e.g. concerning the distinctions that can be readily made between ‘quality care’ and ‘substandard care’), formal quality assurance processes, formal measures of patient outcomes, and the like. The task for the nursing profession is to ensure that health care delivery never falls to a level that compromises patient safety and wellbeing; nurses in many parts of the world have already demonstrated their willingness to ‘blow the whistle’ or to take strike action when patient safety is compromised by substandard conditions and resources (some examples of which will be considered in Chapter 13 of this book).
The right to safe care
It is generally accepted that all people receiving health care have the right to be safe (Kohn et al 2000; Sharpe 2004). This right has been interpreted to mean ‘the right to be kept free of danger or risk of injury while in health care domains’, which in turn has been further interpreted as entailing ‘a correlative duty on the part of health service providers to ensure that people who are receiving care are kept free of danger or risk of injury while receiving that care’ (Johnstone & Kanitsaki 2007c: 186; see also Johnstone 2007a, 2007b). These moral requirements are unremarkable in that they ‘reflect the well-established principle in health care of “do no harm” and the associated moral duty on the part of health care providers to avoid commissions and omissions that could otherwise result in preventable harm to patients’ (Johnstone 2007b: 82). Underpinning this stance is the universal recognition that ‘people generally have a special interest in their significant moral interests (e.g. to life, quality of life, dignity, respect) in not being harmed and that this special interest ought to be protected — provided this can be done without sacrificing other significant moral interests’ (Johnstone 2007b: 82).
The International Council of Nurses (ICN) regards patient safety as being ‘fundamental to quality health and nursing care’ and asserts that all nurses have a fundamental responsibility to ‘address patient safety in all aspects of care’, including (but not limited to) ‘informing patients and others about risk and risk reduction’, ‘advocating for patient safety’ and ‘reporting adverse events to an appropriate authority promptly’ (ICN 2002: 1). In keeping with the principles of a ‘system approach’ to human error management, the ICN explains:
Early identification of risk is key to preventing patient injuries, and depends on maintaining a culture of trust, honesty, integrity, and open communication among patients and providers in the health care system. ICN strongly supports a system-wide approach, based on a philosophy of transparency and reporting — not on blaming and shaming the individual care provider — and incorporating measures that address human and system factors in adverse events.
(ICN 2002: 1)
A noteworthy feature of the right to safe care is the impetus it is providing, via its encompassment in the new patient safety movement, for the development of a non-punitive systems approach to human error management in health care and to reducing the incidence and impact of preventable adverse events in patient care domains. Although the global push to improve patient safety is not without various tensions and controversies (see Johnstone 2007a, 2007b; Johnstone & Kanitsaki 2006a, 2007d; Sharpe 2004), it is unequivocally heralding a new global understanding, commitment and approach to the historical maxim of ‘do no harm’ and to designing and implementing better systems for reducing the incidence and impact of preventable adverse events and the harms that can and do result from these to all concerned (WHO 2005a, 2005b, 2006).
Challenges posed by the right to health care
It can be seen that all four senses of the right to health care pose a significant challenge to the nursing profession. As far as the right to equal access is concerned, nurses have much to contribute. Nurses know very well the areas in which access to health care has effectively been denied to people, and why (e.g. lack of appropriate resource allocation, inappropriate structuring of health care delivery, obstructive institutional policies and legal laws, cultural and language barriers). Despite their knowledge and experience in relation to these matters, however, nurses are not always included in the processes for deciding important policy or health resource allocation matters.
Nurses must directly participate in high-level decision-making concerning health care matters, an imperative already well argued for by Paul Gross (1985) over two decades ago. If nurses fail to influence policy and decision-making, the prospects for patients’ rights, not to mention the nursing profession’s ability to promote and protect these, will remain limited.
The right to health care, in the senses pertaining to appropriate, quality and safe health care, also poses significant challenges to the nursing profession, in terms not only of its own standards, but also of those applied in health care contexts generally. If the nursing profession is to succeed in providing appropriate nursing care (a subcategory of health care), it needs to pay careful and continuous attention to developing its curricula and to ensuring that its members are educationally prepared to meet and to respond to the needs of society, and in particular the needs of the culturally and individually diverse people comprising it. As well as this, the nursing profession must pay careful attention to developing reliable mechanisms for guiding its members in their attempts to deliver safe, quality, therapeutically effective, culturally competent and morally accountable care, and for censuring those of its members who fail to do so.
Nurses, individually and collectively, have a moral responsibility to respond to the demonstrable threats that are mounting against people’s rights to health and health care. How well they can and will succeed in fulfilling this responsibility, however, will depend on how they view justice and the demands it places on them. As Dyck (2005: 322) reminds us, ‘In the end, health care is one of the areas that test whether members of the community in question are aware of, and willing to meet, the moral demands of the moral requisites of community.’ Moreover, in the context of claims to a ‘decent minimum of health care’:
To ask what justice demands of us, to ask what we owe one another, is to ask what kind of community we aspire to be in our relations to one another, particularly when some among us are ill and otherwise in need. What we do about health care reflects what kind of community we are, and what we think ought to be done about health care reflects what kind of community we think we ought to be.
(Dyck 2005: 307–8)
Meanwhile, what we as nurses do about health care reflects what kind of profession we are, and what we think ought to be done about health care reflects what kind of profession we think we ought to be.
T he right to make informed decisions
The right of people (including ‘mature minors’ and the very old) to make informed decisions and to formally consent (or refuse to consent) to treatment in health care contexts is now widely recognised as a ‘basic ethical and legal precondition to conscientious medical practice’ and the conscientious provision of nursing care (Dickens & Cook 2004: 309; see also Alderson et al 2006; Derish & Vanden Heuvel 2000; Dickens & Cook 2005; Dudzinski & Shannon 2006a, 2006b; Forrester & Griffiths 2005; Kerridge et al 2005). Of all the patients’ rights which might be claimed in a given health care context, however, none is perhaps more challenging to the power, authority and sometimes the integrity of attending health professionals than the patient’s right to make informed choices about his or her care and treatment. This might help to explain why, despite the apparent success of the patients’ rights movement over the past few decades, the right of patients to give an informed consent to care and treatment continues to be problematic in some areas. For example, over the past 20 years I have conducted numerous workshops and seminars addressing ethical issues in nursing. Disturbingly, nurses attending these educational activities have consistently identified the following problems in relation to consent to treatment practices:
▪ patients signing consent forms without having any comprehension of what it is they are consenting to
▪ nurses assuming incorrectly that treating doctors have explained a recommended medical procedure or treatment to a patient/relatives before obtaining the patient’s consent
▪ relatives/chosen carers being upset at discovering that a recommended medical procedure had not been properly explained to a loved one before being performed
▪ signed consent forms being treated as generic; that is, as signifying a consent to ‘anything deemed necessary’ during the period of hospitalisation
▪ patients giving consent to a particular procedure being performed, only to discover later that a different procedure was performed without any ‘real choice’ being given (e.g. the patient may have consented to having laparoscopic surgery only; upon recovery, however, he or she finds that a more radical open surgical procedure has been performed)
▪ verbal consents being obtained from relatives/chosen carers over the telephone in situations which are not of a true ‘emergency’ nature (e.g. where there has been a last-minute cancellation from a private list and a bed has become vacant for a new elective surgery patient)
▪ consents being obtained from people of non-English-speaking backgrounds without the assistance of qualified health interpreters
▪ patients consenting to a procedure, knowing what the procedure involves, but having no knowledge of associated risks or potential adverse side effects of the procedure in question
▪ consent being obtained from patients after they have received a pre-medication or when they are under the influence of alcohol or other mind-altering drugs
▪ procedures performed without consent being obtained from the patient at all.
In disclosing these problems, the nurses have also expressed considerable distress at what they see as their inability ‘to do anything about the problem’.
The issue of informed consent has obvious implications for nurses, not least on account of them being at the forefront of receiving requests from patients and relatives for ‘information’. As well, nurses are at the forefront of being expected to take appropriate action when patients’ information needs are not being met and/or when their (the patients’) entitlements in regard to consent practices are unjustly violated. It is therefore important that nurses have a thorough understanding of the nature and function of informed consent, as well as their responsibilities as nurses in relation to facilitating a patient making informed choices about recommended care and treatment options and as are specified in their respective codes of ethics and conduct (see Australian Nursing and Midwifery Council [ANMC] 2008a, 2008b; ICN 2006). It is to exploring these two issues that this discussion will now turn.
What is informed consent?
The doctrine of informed consent, although having a profound ethical dimension, is essentially a legal doctrine developed partially out of recognition of the patient’s right to self-determination and partially out of the doctor’s duty to give the patient ‘information about proposed treatment so as to provide him or her with the opportunity of making an “informed” or “rational” choice as to whether to undergo the treatment’ (Robertson 1981: 102; see also Beauchamp & Childress 2001; Gert et al 1997; Kerridge et al 2005).
In distinguishing the differences between a legal and a moral approach to informed consent, Faden and Beauchamp (1986) explain that the legal law’s approach to informed consent ‘springs from pragmatic theory’, which focuses more on a doctor’s duty to disclose information to patients and not to injure them. By contrast, moral philosophy’s approach to informed consent ‘springs from a principle of respect for autonomy that focuses on the patient or subject, who has a right to make an autonomous choice’ (p 4).
Whether such a clear-cut distinction can be drawn between a legal and a moral approach to informed consent is a matter of some controversy, however. The moral demand to respect autonomy is clearly the prime motivator of the doctor’s duty to disclose information, and the moral principle of non-maleficence is the prime motivator of the doctor’s duty not to injure or harm patients. It seems that, while the moral and legal approaches to informed consent can be loosely distinguished, they are nevertheless inextricably linked. It is this linkage which highlights the other important functions, besides the promotion of patient autonomy, that the application of the doctrine of informed consent also serves, namely those of protecting patients, avoiding fraud and duress (i.e. as occurs when information is not disclosed), of encouraging self-scrutiny by health professionals, of promoting ‘rational’ and systematic moral decision-making, and of involving the public ‘in promoting autonomy as a general social value and in controlling biomedical research’ (Capron 1974; Gert et al 1997; Beauchamp & Childress 2001).
There is no question that consent practices have improved considerably over recent decades. Health professionals have increasingly recognised the benefits of ensuring that patients (and their proxies) are informed appropriately about their care and treatment options, and patients (and their proxies) are more willing to question the information that they have been provided in order to inform their choices and consent to treatment (Chaboyer 2000; Kerridge et al 2005; Tweeddale 2002). Nevertheless nurses continue to witness instances in which consent practices have been questionable and where patients’ rights to make informed choices have been violated. Patients who do not speak or read English proficiently are particularly vulnerable in this regard, as illustrated by the following case of a 66-year-old Greek-born woman (‘Mrs G’) who had been admitted to hospital for elective surgery to treat a kidney disorder (Kanitsaki 1992). In this case informed consent was not obtained. Describing the circumstances surrounding the failure to obtain an informed consent from this woman, Kanitsaki writes (1992: 2–3):
The morning of Mrs G’s operation arrived, and it was observed by the nurse who was to prepare her for theatre, that Mrs G’s consent form was not signed. The nurse reported this to the charge nurse who rang the relevant doctor to come and obtain Mrs G’s signature on the consent form. The surgical registrar arrived, and in an irritable tone asked ‘why this was not done the day before’. The nurse remarked that Mrs G only spoke a few words of English, and would need an interpreter to explain to her what she was signing and why. The doctor replied ‘I know. But I have no time to wait. It will be alright’. He then proceeded to instruct Mrs G how to sign the consent form. Mrs G sat up in bed, however, and looking puzzled, uttered ‘Me no understand. Me no understand.’ The doctor then proceeded to pick up Mrs G’s hand, placed a pen into it, and by holding and directing her hand, made a cross on the consent form. Once this was achieved, the doctor gently touched Mrs G’s hand and said ‘Good. Good.’ He then left the ward.
More recently a 2005 Australian study has suggested that, in some situations, because of not having access to qualified health interpreters, doctors sometimes rely on diagnostic testing (often subjecting patients to an unnecessary barrage of expensive diagnostic investigations) rather than direct diagnostic questioning of patients to find out what might be wrong with them. Consent practices in these situations were, at best, ‘dubious’. The study found that a testing rather than a communicative questioning approach to medical care was most likely to occur in situations where attending health professionals took the stance of treating patients ‘as if’ they were unconscious — sometimes referred to colloquially as ‘veterinary medicine’ (Johnstone & Kanitsaki 2005: 152).
One reason why consent practices in Australia and New Zealand are problematic relates to the model they are based on. Unlike the United States (US) and Canada, which use a reasonable patient standard (also called ‘reasonable person standard of disclosure’) model of consent (emphasising trespass and battery), Australia and New Zealand tend to use a reasonable doctor standard (also called ‘professional practice standard of disclosure’) model (emphasising negligence and malpractice) — although, following the High Court of Australia case of Rogers v Whittaker (1992), Australia has moved somewhere between the two, adopting a ‘subjective person standard’ (emphasising a ‘duty to disclose’ information that an individual patient may require (Kerridge et al 2005: 217–18; see also Russell 1987: 18). Understanding the difference between these three models is important to any debate on informed consent, and I will briefly outline them here. (For a more detailed discussion on the legal aspects of informed consent to medical treatment, see Andrews 1985; Dickens & Cook 2004; Faden & Beauchamp 1986; Forrester & Griffiths 2005; Kerridge et al 2005; Kirby 1995; Law Reform Commission of Victoria et al 1987).
In the reasonable doctor standard model of consent, a consensus of reasonable and established medical opinion provides the ‘objective’ measure. On the basis of this model, a doctor has the duty to use reasonable skill and may withhold information if, in the doctor’s opinion, its disclosure would be injurious to the patient. If patients are to successfully sue for damages on account of a failure to disclose information relevant to the consent process, they have to show, first, that the doctor failed to provide information and advice to a patient that accords with the ‘practice existing in the medical profession’ (Law Reform Commission of Victoria et al 1987: 8), and, second, that injury was suffered as a (causally) direct result of this negligence. In establishing whether the doctor did in fact use ‘reasonable skill’, the law would appeal to the reasonable doctor standard model and would ask what most or many reasonable and competent doctors in a given particular branch of medicine would do and say in such circumstances; that is, what would be considered ‘accepted medical practice’ in this situation? If there were conflict, the answer to this question would be sought from an expert medical witness, or witnesses, who would testify what they, as reasonable and competent doctors in a particular branch of medicine, would probably do or say in the circumstances under question.
For example, the question of whether a doctor should have disclosed to a patient a 0.1–0.2% risk of quadriplegia in cases involving cervical spinal surgery would ultimately be decided on the basis of whether other reasonable and competent doctors in the field usually disclose this information. If it could be established that other reasonable doctors do not disclose to their patients a 0.1–0.2% risk of quadriplegia in cases involving cervical spinal surgery, it is likely that a doctor who failed to disclose such information to a patient would not be found negligent or causally responsible for the patient’s injuries in the case of a material risk manifesting itself (such as quadriplegia).
In the reasonable patient standard model, on the other hand, the standard is set ‘by reference to hypothetical behaviour of adult, competent people in the sorts of situations which are presented to courts and other tribunals for decision’ (Law Reform Commission of Victoria et al 1987: 8). On the basis of this model, a doctor has the duty to disclose to the patient all the information necessary to making an intelligent and ‘rational’ choice (including information pertaining to small material risks). For example, consider the hypothetical case of a patient who has suffered the complication of quadriplegia following a cervical spinal fusion. Consider further that the patient claims that, had information been given about the associated risk of quadriplegia, the operation would never have been consented to in the first place. The famous Sidaway case provides an instructive example of this kind of situation (Law Reform Commission of Victoria et al 1987: 3–4, 37–9; Andrews 1985: 14). In the hypothetical case, the question of whether a doctor should have disclosed to the patient a 0.1–0.2% risk of quadriplegia in cases involving cervical spinal surgery would ultimately be decided on the basis of whether:
1. the information that was withheld was critical to the patient’s making an intelligent choice
2. the information would have caused the patient to make a different choice had she or he been informed of the associated risks before giving consent
3. the patient’s desire to know of the given associated material risks was consistent with the desires of a hypothetical reasonable and competent adult
4. the risk was considered to be severe (i.e. the injury, were it to occur, would be of a serious nature; quadriplegia in this instance is clearly ‘severe’ viz ‘of a serious nature’)
5. the probability of the risk occurring was high.
If it could be established, in this instance, that the patient would not have consented to the procedure, and that the patient’s declining to give consent would have been consistent with what a hypothetical reasonable and competent adult would do in a similar situation, then the patient’s original consent would be vitiated and the doctor would be found guilty of trespass and battery.
In the subjective person model, the standard is based on the requirement to tell ‘each individual patient exactly what they would wish to know’ [emphasis original] (Kerridge et al 2005: 218). According to this standard:
If a patient wants or would need certain information in order to make an informed decision that is congruent with her or her life-goals, then non-disclosure of such information may infringe upon personal autonomy.
(Kerridge et al 2005: 218)
The influence of this standard has been most evident in the High Court of Australia case of Rogers v Whittaker (1992), involving a 47-year-old woman who developed sympathetic opthalmia and who became completely blind after undergoing reparative eye surgery for a penetrating eye injury. This case is widely credited with representing the Australian position ‘not only in relation to the standards of the duty of care for health professionals, but also in relation to “whether the standards of care is a matter of medical judgment only”’ (Forrester & Griffiths 2005: 96). Evidence was given at the court hearing that the treating surgeon told the woman that the surgery would improve both her appearance and her vision; it was further revealed that the surgeon regarded the risk of sympathetic opthalmia as being so remote that he did not disclose it to her. The Court, however, took a different view and affirmed that health professionals (and the surgeon in this case) have a stringent duty to disclose information that an individual patient may require — including being warned about the material risks of given treatments — ‘even when the patient does not seek information through specific questions’ (Kerridge et al 2005: 218; see also Forrester & Griffiths 2005: 96). In North America a similar stance has been assumed with legal scholars arguing that, in addition to being given information about material risks, patients should also be given information on how to ask any additional questions that may occur to them during the ongoing process of their care (Dickens & Cook 2004: 313).
All models depend on the further consideration of a patient’s rational or legal competence — a matter that, rightly or wrongly, only the courts can decide (the question of patient competency will be considered later in this discussion).
Whatever the legal considerations and arguments for or against these models, from a moral point of view (and, indeed, a pragmatic point of view) neither is free of difficulties. For example, the reasonable doctor standard can be unreliable on account of doctors often being reluctant to testify against their colleagues. Commenting on Australia’s medical defence unions, Stephen Rice writes (1988: 124):
… the medical defence unions operating in Australia claim they do not object to their members testifying against colleagues. But they stress to members in newsletters: — ‘Avoid unnecessary criticism of the work or conduct of other practitioners.’
The reasonable patient and ‘subjective person’ standards, however, can also be unreliable. For example, who is to say what is to count as a ‘reasonable’ patient, hypothetical or otherwise? Is it realistic to believe and accept that an abstract ‘hypothetical reasonable and competent adult’ — divorced from any cultural, social, historical and spiritual context of living — is able to represent reliably and truthfully what an actual person whose ‘reasonableness’ is at issue would ultimately desire? What one patient or ‘subjective person’ might consider reasonable, another might equally reject; and vice versa. The case of Jehovah’s Witnesses and their well- recognised refusal to accept life-saving blood transfusions is a point in question. It is not difficult to imagine a ‘reasonable patient’ of the Jehovah’s Witness faith refusing a blood transfusion against an overwhelming body of public opinion that such a refusal was ‘unreasonable’ and even ‘mad’ or ‘idiotic’.
The case of children (mature minors) reasonably refusing burdensome medical treatment against adult opinion is another example. A particular example of this can be found in the controversial English case involving a 15-year-old girl who underwent a heart transplant by order of a British High Court. The girl did not want the transplant explaining ‘I would feel different with someone else’s heart — that is a good enough reason not to have a heart transplant, even if it saved my life’ (Boseley & Dyer 1999: 19). Treating doctors and the Court disagreed, however, and the girl’s wishes were overridden on the ‘reasonable’ grounds that the heart transplant would save her life.
In dealing with these and other difficulties, as well as with other more general objections which may be raised against the doctrine of informed consent, it is important not to lose sight of the various theoretical perspectives underpinning and justifying the right of people to make informed choices about their care and treatment. For instance, key to both the legal doctrine and moral right of informed consent is (1) the liberal democratic notion of the sovereignty of the individual, and (2) ethical principlism, considered under separate subheadings below.
Informed consent and the sovereignty of the individual
Informed consent rests heavily on the view that the individual is sovereign alias the sovereignty of the individual. This highly individualistic notion characterises the person (patient) as a solitary competent individual who possesses ‘a sphere of protected activity or privacy free from unwanted interference’; by this view, although ‘influence is acceptable’, coercion in any form is not (Kuczewski 1996: 30). Kuczewski explains that (p 30):
Within this zone of privacy, one is able to exercise his or her liberty and discretion. Within this protected sphere take place disclosure, comprehension, and choice, which express the patient’s right of self-determination … The person is opaque to others and therefore the best judge and guardian of his or her own interests. Although the physician may be the expert on the medical ‘facts’, the patient is the only individual with genuine insight into his [sic] private sphere of ‘values’. Because treatment plans should reflect personal values as well as medical realities, the patient must be the ultimate decision-maker.
One serious and significant implication of this view is that the patient’s family, friends and/or chosen carers (acknowledging here that not all patients have families or, if they do, desire the involvement of their families) are conceived ‘as comprising competing interests’; they are also seen as having no entitlements whatsoever in regard to any consent to medical treatment processes that the ‘sovereign individual’ might otherwise engage in (Kuczewski 1996). This may help to explain some of the tensions examined previously in Chapter 4 (pages 78, 80, 91) in regard to family members of traditional cultural backgrounds seeking active participation in consent to medical treatment processes and the reluctance by some doctors and nurses to involve these family members in such processes.
Bioethicists and clinicians (particularly palliative care physicians) are, however, rethinking their traditional opposition to the involvement of family or chosen carers in consent to treatment practices (Chaboyer 2000). There is increasing recognition that illness can seriously undermine the patient’s capacity to make prudent self-determined choices (autonomy) and to be an effective judge and guardian of his or her own self-interests. This has been matched by an increasing questioning of the traditional legalistic approach to informed consent that, among other things, presupposes that the values of the ‘sovereign individual’ are well developed, fixed and adequate to the task of choosing between difficult treatment options, and that all the chooser needs in order to make an informed choice is ‘information’ (Gert 2002; Kuczewski 1996).
Increasingly, as previously discussed in Chapter 4 of this book, family members and chosen carers are recognised as having a vital role to play in consent processes and care of loved ones. By being intimately acquainted with (‘knowing well’) the patient, family members or chosen carers are able to provide appropriate and meaningful feedback to their loved ones, and to generally assist in ‘reality checking’ their loved one’s choices and the values, beliefs (new and old), and deliberations influencing these choices. In sum, the involvement of family members and/or chosen carers in consent to treatment processes can play a vital role in restoring the otherwise diminished autonomy of their sick loved ones (Kuczewski 1996). Furthermore, by fulfilling this role, they are also able to strengthen the bonds of their relationship with the patient and with each other — in short, to express their care of and for each other.
Informed consent and ethical principlism
Informed consent also rests heavily on ethical principlism (discussed in Chapter 3 of this book), both for its content and justification as an action guide. The principles of particular importance here include those of:
▪ autonomy — which demands respect for patients as self-determining choosers, and justifies allowing them the option of accepting risks
▪ non-maleficence — which demands the protection of patients from battery, assault, trespass, exploitation and other harms that may result from inadequate or inappropriate consent processes (including the inadequate or inappropriate disclosure of information)
▪ beneficence — which demands the maximisation of patient wellbeing via consent processes
▪ justice — which demands fairness and that patients not be unduly or intolerably burdened by consent processes.
It should be noted that while autonomy is a value underlying the doctrine of informed consent it is not the value, nor an absolute value. As Faden and Beauchamp (1986: 18) point out, at best autonomy is only a prima-facie value, and to regard it as having overriding value would be both historically and culturally ‘odd’. This is not to say that autonomy does not have a significant place in a moral approach to informed consent. It merely means that it does not have a sole place, and can be justly restricted by other competing moral principles, such as those already mentioned.
Having now reviewed the function and theoretical underpinnings of informed consent, let us proceed critically to examine the constituents and nature of informed consent.
The elements of an informed and valid consent
It is generally recognised within bioethics that disclosure, comprehension, voluntariness, competence and consent itself form the analytical components of the concept of informed consent (Faden & Beauchamp 1986: 274).
Morally speaking, for a consent to be regarded as informed, it must satisfy a number of criteria, including those relating to the informational aspect of the consent and those relating to the giving of consent itself. Beauchamp and Childress (2001: 77–98) argue that for consent to be informed: there must be a disclosure of all the relevant information (including both benefits and risks); the patient must fully understand (comprehend) both the information which has been given and the implications of giving consent; the consent must be voluntarily given (i.e. the patient must be free of coercion or manipulation); and, lastly, the patient must be competent to consent (i.e. be both ‘rational’ and prudent). Faden and Beauchamp (1986: 54) argue along similar lines, and recommend what they believe are less ‘over demanding’ and plausible criteria, notably:
(1) a patient or subject must agree to an intervention based on an understanding of (usually disclosed) relevant information, (2) consent must not be controlled by influences that would engineer the outcome, and (3) the consent must involve the intentional giving of permission for an intervention.
It needs to be noted that patients frequently do not realise that in giving consent they are not merely acknowledging the receipt of information concerning a recommended medical treatment or procedure, but are also actually giving permission to an attending health professional to go ahead and perform the treatment or procedure in question.
Faden and Beauchamp’s (1986) foundational work and theory of informed consent is probably one of the most comprehensive to date, and one which, although written from the cultural perspective of the US, deserves to be given serious attention by those furthering the informed consent debate in Australia, New Zealand and other common law countries. As well as advancing their ethical theory, these authors also make a number of useful practical suggestions on how informed consent practices could be made more ‘workable’.
It should be noted that the doctrine of informed consent has been the subject of much controversy, most notably among health professionals. Common objections include:
▪ obtaining an informed consent is unacceptably time-consuming
▪ when patients are told the information they need to know, they forget it
▪ most patients do not want to know all the details of the risks and benefits associated with a recommended medical treatment or procedure, and forcing information on them would be just as paternalistic as withholding it
▪ most patients would not understand the information required to make an informed choice
▪ giving information to patients can be harmful (e.g. they might refuse a life-saving procedure or drug because of a negligible risk)
▪ informed consent is impractical and thus unworkable.
These and similar objections are, however, difficult to sustain in the face of research findings, anecdotes and professional experience. For example, it is well recognised that people in stressful and unfamiliar situations are vulnerable both to information overload and short-term memory loss. The stress of being admitted to hospital; of coping with feelings of pain, fear and anxiety; of being separated from the familiarity of one’s home, family and friends; the general disruption of one’s life, not to mention the effort required to adapt to a new (hospital) environment characterised by strange smells, sights, noises, tastes, routines, faces, procedures and sensations — may all contribute to lessening an individual’s capacity to pay attention to and to recall information that has been disclosed. It is thus understandable that patients might sometimes forget or have their capacity to understand the information that has been given to them compromised by these factors.
To complicate matters, health professionals seeking consent or giving information do not always manage their encounters with patients very well. Some use a hurried, uninterested and sometimes intimidating approach when seeking a patient’s consent. When seeking consent from a patient, health professionals may fail to give due attention to such things as: controlling their tone of voice, choosing a suitable time and place to approach the patient, ensuring privacy, using the appropriate body language and facial expressions, choosing the right words, avoiding complicated jargon, sitting at the patient’s level, being generally respectful, and so on.
When dealing with non-English-speaking patients, these problems are considerably worse. For example, health professionals may shout unnecessarily (a problem which also sometimes occurs when they are dealing with blind or physically handicapped people who nevertheless have perfect hearing), or they may use inappropriate body language and facial expressions, use the wrong intonations in speech, or use terms which cannot be readily interpreted into the patient’s spoken language.
As far as patients who do not want to know the details of an impending medical procedure are concerned, there are few who seem to fit into this category. In some instances patients have declined information (on the basis of personal and cultural health beliefs and practices), but even then only certain select pieces of information have been declined; in these instances, patients have not voiced a blanket and unconditional rejection of all relevant information. In many instances, what has superficially appeared to be a ‘refusal’ was in fact more a demand that the information be given in a culturally appropriate manner (see discussion in Chapter 4 of this book). If, however, patients do make an informed and authentic choice not to receive certain relevant pieces of information, and on reflection are not open to changing their minds about receiving the information in question, then to give this information to the patients would certainly count as a paternalistic act (the subject of ‘paternalism’ will be considered shortly below).
The objection that patients would not be able to understand the necessary information in order to make an intelligent and informed choice is also difficult to sustain. It is sometimes difficult to avoid the impression that the claim that a patient cannot understand is more an assumption than a matter of sound deliberation and determination. Buchanan (1978: 386), for example, argues that to assume a patient would not understand given information is to make a ‘dubious and extremely broad psychological generalisation’, which, of course, ordinary doctors and nurses are not particularly qualified to make. Faden and Beauchamp (1986) also argue that most patients are able to understand the information given to them, and, what is more, that a patient’s level of understanding can be ascertained and measured.
Even if patients do not fully understand the information given, this does not always imply that it is the fault of the patient. A patient’s inability to understand may be directly related to a doctor’s or a nurse’s inappropriate behaviour and communication (Roth et al 1983: 176). The onus then is on those seeking to obtain consent to improve their approach to patients, and to presume a patient’s ability to understand information rather than an inability to understand. On this point Muyskens (1982a: 119) argues:
as in a court of law in which one’s innocence is presumed until proven otherwise, the client’s ability to comprehend and understand what is going on and to be able to make judgments based on the data must be presumed until firm evidence establishes the contrary.
Just as there is no compelling evidence to suggest that patients would not understand information disclosed to them about a proposed medical or nursing procedure, there is no compelling evidence to suggest that patients would be unduly injured or harmed by disclosures. Bok (1980) has long contended that very few patients withdraw their consent when informed of material risks or other so-called ‘harmful’ pieces of information concerning a proposed medical procedure. She further contends that in fact ‘it is what patients do not know but vaguely suspect that causes them corrosive worry’ (Bok 1980: 234).
Buchanan (1978) is even more critical of the view that the disclosure of information material to a treatment decision may cause harm to patients, arguing that such a view reeks of nothing more than wide and unfounded ‘psychiatric generalisations’, which ordinary doctors and nurses are not qualified to make. He argues further that even qualified psychiatric specialists would probably find it very difficult to judge correctly whether a patient would be significantly harmed by disclosure.
The ‘information causing harm’ objection, of course, also ignores the point that, even if a patient refused to undergo a recommended medical procedure on the basis of information received about certain material risks, this is, after all, something which any competent patient is morally entitled to do — whatever the risks involved and regardless of what others might think of their refusal (see also Tweeddale 2002; Forrester & Griffiths 2005; Kerridge et al 2005). At best, all attending health professionals can morally do is to persuade patients non-coercively about the known benefits of undergoing a given medical procedure; but they are not entitled to interfere with the patient’s choice if such persuasion fails (Faden & Beauchamp 1986).
Even if critics concede that these objections cannot be sustained, the objection still remains that informed consent procedures are impractical because they are unrealistically and unacceptably time-consuming. It is likely that obtaining a voluntary consent (i.e. one free of coercive or manipulative influences) and informed consent from a patient will take more time than obtaining an involuntary and uninformed consent. Nonetheless, health professionals have a responsibility to take the time required to interact and communicate with their patients in a way that facilitates making informed choices and realising morally just outcomes. Moreover, there can be no excuse (except possibly in an emergency life-threatening situation) for denying patients the time needed to deal with an anxiety, to answer a worrisome question, or to be reassured. Patients must have sufficient time to make an adequate decision and must have sufficient time to contemplate viable and real alternatives; anything less may result in information overload and may undermine their ability to make voluntary and informed choices (Faden & Beauchamp 1986: 326).
In a culture so heavily dominated and constrained by considerations of ‘time’, it may be tempting to accept ‘time constraint’ as a valid reason for abrogating one’s moral responsibilities. This, however, is not acceptable morally. Moreover there are many ways in which the difficulties posed by time constraints can be overcome. One possible solution is to involve others (including lawful proxies, family and/or chosen carers) in the processes of transferring and sharing information with patients. While it is obviously and properly the responsibility of treating doctors to obtain informed consents to medical treatment from the patients they are treating, there is nevertheless considerable room to suggest that a collaborative approach to meeting patients’ information needs would contribute substantially to maximising the patients’ moral interests.
Rightly or wrongly, nurses already play a major, although unacknowledged, role in meeting patients’ information needs. This situation has arisen for many reasons, including the problem that treating doctors sometimes fail, for various reasons, to meet the information needs of their patients. In situations like this, an attending nurse is often the only immediately available person patients (and their families) have to turn to in order to obtain the information they want. Indeed, nurses are very often the ones whom patients ask directly about what to expect of a given or pending medical procedure or treatment. In such instances, nurses can find themselves in a very difficult situation — particularly if an attending doctor will not respond appropriately to a patient’s request for information. The nurses’ dilemma is compounded by the fact that they know they can contribute a great deal to allaying patient anxiety related to knowledge deficits concerning proposed and rendered medical care and treatment options, but do not have the legitimated authority to undertake this role. Thus, if and when they are giving information to patients about medical treatments, nurses know they are ‘taking a risk’, since this could be construed as ‘interfering with the physician–patient relationship’ — as, indeed, has happened in a number of high-profile legal cases (see Johnstone 1994).
Studies have long shown that nurses can greatly assist patients in coming to understand their illness experience and physician directives given during medical consultations (Uyer 1986). One study also shows that the task of giving information to patients and satisfying patients’ information needs is ‘ impossible without systematic collaboration between medical and nursing staff’ (Engstrom 1986, emphasis added). It is clear that this is a matter which requires much greater attention than it has been given up until now with a view towards legitimating the role of nurses in meeting patients’ information needs.
A second obvious strategy which could be used to help resolve the time-constraint problem is to restructure the time frame itself during which consents are usually sought. In elective admissions, consents are usually sought on the day before or evening before a scheduled medical or surgical procedure. The moral disadvantages of this are obvious. As Faden and Beauchamp ask (1986: 325):
who would want, on the eve of surgery after having disrupted one’s life, gathered one’s courage, and entered the hospital, to change one’s mind? And thus who would want to pay attention to information that challenges the wisdom of the decision?
Such a short time frame is not conducive to patients exercising voluntary and informed consent. One possible solution — and one that is routinely practised in some areas — would be to give patients all the ‘usual’ information during a pre-admission clinic a week or so before the procedure. In this way, patients have time to go home, contemplate the information received, discuss it with family and friends, formulate any further questions they would like to ask, or even change their minds and decline the recommended therapy or procedure if they so desired. If patients are allowed time to reflect on the information given to them, not only would their consents to treatment be of better quality, but so too would their decisions to enter hospital.
The time factor involved in obtaining consent is crucial to the realisation of morally just outcomes. If sufficient time is not allocated for the purposes of gaining a patient’s consent, a very real risk exists that the voluntary and informed nature of the consent will be seriously compromised, thus having the domino effect of violating underlying moral principles such as autonomy, non-maleficence, beneficence and justice. In other words, a complete moral collapse of the situation could occur. In emergency or life-threatening situations, of course, it is not always possible to seek an informed consent and it could be hazardous to try and do so. The law recognises that in emergency or life-threatening situations consent can be ‘waived’; morality likewise recognises situations in which consent can be justly waived.
The challenge to doctors and nurses and other health professionals is to restructure their thinking on informed consent, and to view it as something which ‘should help overcome the inclination that many people have to yield compliantly to proposals from powerful authority figures’ (Faden & Beauchamp 1986: 372). Faden and Beauchamp (p 305) argue that the questions that all health professionals and policy and law makers should be asking are not what patients should be told or even who should tell them, but: ‘What can professionals do to facilitate obtaining informed consents based on substantial understanding?’ or ‘How can professionals enable patients and subjects to make informed autonomous choices?’
If informed consent procedures are to work and to achieve their desired ends, a number of other practical considerations need to be attended to. First, consent forms should be made available in the patient’s own language and obtaining consent facilitated by the involvement of qualified health interpreters. It was once the practice to ask cleaners or orderlies or kitchen hands who speak languages other than English to interpret for a non-English-speaking patient (see Stone 1991: 4). This situation still arises on occasion despite being proscribed by government policy and deemed as an unacceptable standard of practice (Johnstone & Kanitsaki 2005). One reason why it is regarded as unacceptable practice is that orderlies and cleaners and kitchen hands are neither trained nor credentialed as health interpreters and thus may seriously misinterpret the information being relayed, or may give their own assessment of and interpretation of a question being asked. For example, Olga Kanitsaki (who is Greek-speaking) describes a case involving a Greek-speaking patient. In this case, a cleaner called in to interpret for the doctor exclaimed to the patient, in Greek, ‘Well, if you only have a headache why don’t you take an aspirin? What did you come into hospital for? Why are you bothering the doctor?’ (personal communication). Other studies have likewise found that people used as interpreters in the health care system sometimes ‘edit out’ information that is of importance to the patient’s health care (Brough 2006: 26).
Another problem, and one often overlooked by health professionals, is that orderlies and cleaners and kitchen hands do not have a professional relationship with the patient; thus, involving them as interpreters is tantamount to breaching confidentiality. Who is to know whether these ‘informal’ interpreters will keep confidential the information disclosed during an interpreting session? Since they are not bound by any professional code of ethics, they may not fully appreciate their moral responsibilities not to disclose the confidential information they have become privy to while acting as interpreters.
A second practical consideration is that patients’ consent must be continuously re-evaluated so as to check whether their original consent still holds. This is particularly crucial in situations involving ‘Not For Resuscitation’ directives (also called ‘Do Not Resuscitate’ directives) or refusal to consent to given life-saving therapies. In some instances, the terms of a patient’s original consent may need to be modified. It has been asserted informally by those working in the area that the term ‘informed consent’ should be abandoned in favour of the term ‘informed decision-making’. The rationale given is that the notion of informed consent has an air of finality about it — that is, once consent has been obtained that is the end of the process. With the notion of informed decision-making, however, the connotations are quite different. In contrast, it has an air of ‘open-endedness’ about it — of a process that is ongoing. Given this, it is thought, the notion of informed decision-making, unlike the notion of informed consent, seems to invite the continuous re-evaluation of any decisions made about care and treatment options. Although yet to be fully embraced, this change in thinking is slowly beginning to be reflected in literature on the subject (see, e.g. Dickens & Cook 2004).
A third consideration is that patients must be informed of their entitlement to refuse a recommended medical or nursing procedure, and the opportunity to refuse must always be present without prejudice to the patients — even when refusals may give rise to significant moral distress in care providers (see, in particular, the case study of a competent patient’s refusal of nursing care, including turning and incontinence management, examined by Dudzinski & Shannon [2006a, 2006b], and the related commentary by Tong [2006]). Fourth, patients must be kept up to date on the relevant details pertaining to their cases. Details which are not readily understood should be explained (in understandable language), and reinforced through planned patient health education programs (something that nurses are educationally prepared to undertake).
Lastly, health professionals need to remind themselves constantly that many factors can deter patients from exercising informed and voluntary choices, including, but not limited to, fear of victimisation. For example, patients may fear that if they refuse to give consent to some aspect of the proposed procedure they may be victimised by being denied other forms of treatment or by being verbally and emotionally abused. Other factors include: feelings of guilt where patients might feel, for example, that somehow they ought to give consent for the sake of their families (see Roberts 1987; Hyun 2002); fear of unknown outcomes; frank disagreement and value conflict, where patients might refuse simply because they do not agree with a given recommended medical therapy and would prefer to try an alternative health modality; pain or grief states which can cloud patients’ prudence; ‘rational incompetence’, and an associated inability to exercise self-determining choices; and incompetent or impaired health professionals who may, for instance, be poor communicators, have poor interpersonal skills, be rushed or hurried, or lack the relevant information to give to the patient.
Before concluding this discussion two further issues remain to be addressed — the problem of the so-called ‘rationally incompetent’ patient and medical paternalism.
The problem of rational competency
Critical to satisfying the requirements of informed consent is competency to decide. The issue of competency is, however, controversial and complicated. This is because there is no substantial agreement on the characteristics of a ‘competent person’ or on how ‘competency’ should be measured. Nor is there any legal test of competency that ‘commands general acceptance’ (Gert et al 1997: 131). To complicate this matter further, there is also no substantial agreement on what constitutes rationality which, as has been argued elsewhere, is very much a matter of subjective interpretation (Johnstone 1999a: 122). As Gibson (1976) points out in an early article on the subject, rationality cannot escape the influences of the social patterns and institutions around it and, for this reason, any value-neutral account of rationality is quite inadequate. She further suggests that at most rationality should be regarded as a value, rather than a property that all ‘normal’ people have (Gibson 1976: 193). In summary, the notion of ‘rational competency’ is problematic because there is no precise definition of, or agreement on, what it is.
Even if there was agreement on what constitutes rational competency, there remains the problem of ‘whereby the definition of competence changes in different clinical situations’ (Gert et al 1997: 135). For example, an elderly demented resident may be deemed competent to eat his/her evening meal alone, but deemed not to be competent to refuse treatment (e.g. suturing) of a deep and bloody laceration to his/her arm. As Gert et al (p 132) go on to explain, we need to appreciate that persons as such are ‘not globally “competent” but rather “competent to do X”, where X is some specific physical or mental task’. In other words, competence is always ‘task-specific’ and determining or measuring competence is thus always ‘context-dependent’ (see also Mukherjee & Shah 2001).
Significantly the issue of competency rarely arises in contexts where the patient agrees with and consents to a doctor’s recommended or prescribed treatment. Gert et al (1997: 142) suggest controversially that this is because ‘doctors almost always recommend treatments that it would be rational for patients to choose’. They go on to argue that it is mostly in ‘cases of treatment refusals, especially those that appear to be irrational, that the question of a patient’s competence most frequently and appropriately arises’ (p 142). A good example of this can be found in the much publicised Australian case of John McEwan that occurred in the mid-1980s and which sparked an unprecedented public inquiry into the so-called ‘right to die with dignity’ (Social Development Committee 1987).
John McEwan, a former Australian water-skiing champion, was left a ventilator-dependent quadriplegic after a diving accident at Echuca, Victoria. Throughout his hospitalisation, he repeatedly asked to be allowed to die. At one point, desperate to achieve his wish, he went on a hunger strike and instructed his solicitor to draw up a ‘living will’, which stated ‘that he did not wish to be revived if and when he fell into a coma’ ( Bioethics News 1985: 2). According to media reports, this act led to a psychiatrist certifying him as rationally incompetent, thereby enabling John McEwan to be treated (fed) against his will. The psychiatrist’s judgment was revoked a few days later, however, when John McEwan ‘agreed to end his hunger strike and accept a course of antidepressants’ (p 2).
A little over a year after his accident, and despite still being ventilator-dependent, John McEwan was discharged home. The round-the-clock day care he required was given by family members and friends who had received special training in how to care for him. In the weeks following his discharge from hospital, John McEwan continued to express his wish to be allowed to die (Social Development Committee 1987: 310–11). This prompted the general practitioner who was medically responsible for him to inform the senior nursing assistant that:
John McEwan at his own request could come off the ventilator from time to time but had to be reconnected if he became distressed even if it was against his own wishes.
(Social Development Committee 1987: 312, emphasis added)
During one incident, while at home, John McEwan was observed to be angry at having been reconnected to the ventilator against his wishes. And in another incident shortly before his death, he talked openly with his general practitioner about ‘hiring someone to blow his [John McEwan’s] brains out or kill him as he felt his wish to die was being frustrated’ (Social Development Committee 1987: 316). There was no reason to suspect that John McEwan’s wishes were irrational. Before his accident he had been a committed sportsman and for him the life of a helpless quadriplegic was intolerable.
At four o’clock in the morning on 3 April 1986, John McEwan was found dead by his nursing attendant. At the time of discovery he was disconnected from his ventilator.
It is perhaps easy to think of competency in cases such as this in purely medical or psychiatric terms. In their classic and still frequently cited work, Roth et al (1983) argue, however, that the concept of competency is not merely a psychiatric or medical concept, as some might assume, but is also fundamentally social and legal in nature. They go on to warn that there is no magical definition of competency, and that the problems posed by so-called ‘incompetent’ persons are very often problems of personal prejudices and social biases, or of other difficulties associated with trying to find the ‘right’ words.
The critical issue in developing tests of competency is how to strike a happy balance between serving a rationally incompetent person’s autonomy and also serving that person’s health care, nursing care and medical treatment needs. Also of critical concern is finding a competency test which is comprehensive enough to deal with diverse situations, which can be applied reliably, and which is mutually acceptable to health care professionals, lawyers, judges and the community at large.
Roth et al (1983: 173) suggest that competency tests proposed in the literature basically fall into five categories:
1. evidencing a choice
2. ‘reasonable’ outcome of choice
3. choice based on ‘rational’ reasons
4. ability to understand
5. actual understanding.
The test of evidencing a choice is as it sounds, and is concerned only with whether a patient’s choice is ‘evident’; that is, whether it is present or absent. For example, a fully comatose patient would be unable to evidence a choice, unlike a semi-comatose patient or a brain-injured person, who could evidence a choice by opening and shutting their eyes or by squeezing someone’s hand to indicate ‘yes’ or ‘no’. The quality of the patient’s choice in this instance is quite irrelevant. One problem with this test, however, is whether, say, the blinking of a patient’s eyes can be relied upon as evidencing a choice; in a life and death situation one would need to be very sure that a patient’s so-called ‘evidencing a choice’ is more than just a reflex.
The test of reasonable outcome of choice is again as it sounds, and focuses on the outcome of a given choice, as opposed to the mere presence or absence of a choice. The objective test here is similar to that employed in law, and involves asking the question: What would a reasonable person in like circumstances consider to be a reasonable outcome? The reliability of this measure is, of course, open to serious question — as previously objected, what one person might accept as reasonable another might equally reject.
The test of choice based on ‘rational’ reasons is a little more difficult to apply. Basically, it asks whether a given choice is the product of ‘mental illness’ or whether it is the product of prudent and critically reflective deliberation. A number of objections can be raised here. For example, contrary to popular medical opinion, there is nothing to suggest that a person’s decision to suicide is always the product of mental disease or depression. A patient could without contradiction ‘rationally’ choose to suicide as a means of escaping an intolerable life characterised by suffering intractable and intolerable pain. Alternatively, a depressed and so-called ‘irrational’ person might refuse a particular psychiatric treatment, such as psychotropic drugs, electroconvulsive therapy (ECT), or psychosurgery, out of a very ‘rational’ and well-founded fear of what undesirable effects these treatments might ultimately have.
The test of ability to understand, on the other hand, asks whether the patient is able to comprehend the risks, benefits and alternatives to a proposed medical procedure, as well as the implications of giving consent. Here objections can be raised concerning just how sophisticated a patient’s understanding needs to be. The problem also may arise of patients perceiving a risk as a benefit. Roth et al (1983: 175), for example, cite the case of a 49-year-old woman psychiatric patient who was informed that there was a one in three thousand chance of dying from ECT. When told of this risk she replied, happily: ‘I hope I am the one!’
The fifth and final competency test is that of actual understanding. This test asks how well the patient has actually understood information which has been disclosed. This can be established by asking patients probing questions and inviting them to reiterate the information they have received. On the basis of educated skill and past experience, the health professional is usually able to ascertain the level at which the patient has understood the information received and what data gaps or misunderstandings remain.
A variation of this test is advanced by Grisso and Appelbaum (1998: 31), and includes assessing patients for their abilities to:
1. express a choice
2. understand information relevant to treatment decision-making
3. appreciate the significance of that information for [their] own situation, especially concerning [their own] illness and the probable consequences of [their] treatment options
4. reason with relevant information so as to engage in a logical process of weighing treatment options [emphasis original].
Issues raised by this test criteria are much the same as those already considered above in relation to Roth et al’s competency test (Gert et al 1997).
Whatever the patients’ competency to decide and quality of their autonomous choice may be, any duty of respect owed would still ultimately depend on the demands of other competing moral considerations, as already discussed. Thus, what may appear to be a dilemma involving whether to respect a patient’s autonomy may not in fact be a dilemma at all. For example, if an elderly demented patient keeps wandering aimlessly from his bed, and is at risk of falling and fracturing his hip, overriding considerations do exist which would justify interfering with the choice to wander. If, after careful analysis of all available alternatives, the only way to stop this elderly patient from sustaining a fractured hip is to restrain him, it may well be that the use of a comfortable restraining device is the morally compelling option in this case. If, however, the elderly person is not at risk of falling and sustaining a fractured hip, and his wandering is merely an ‘inconvenience’ to staff, the solution might be better found in securing door locks so as to prevent the patient from wandering out onto the street where there is a very real risk of injury — say, of being hit by a car. This solution is already employed in a number of residential care homes which have installed combination locks on all their doors; only those residents who know the combination of the locks on the doors can freely come and go. Either way, entitlements and corresponding duties in the case of ‘rational incompetence’ must ultimately be determined by critical reflection and not, as can happen, by misguided or unfounded assumption.
It should be noted that competency is a key issue not just in aged care or psychiatric nursing, but in any health care context where judgments of competency are critical to deciding: (1) whether a patient can or should decide and/or be permitted to decide for herself or himself, and (2) the point at which another or others will need to or should decide for the patient — that is, become what Buchanan and Brock (1989) term surrogate decision-makers and what others call ‘proxies’ (Chaboyer 2000). The question remains, however, of how these things can be decided in a morally sound and just way. This question becomes even more problematic when it is considered that patients deemed ‘rationally incompetent’ (or at least, cognitively impaired) can still be quite capable of making ‘reasonable’ self-interested choices, and, further, that the choices they make — even if ‘irrational’ — are not always harmful (Williams 2002).
Commenting on the moral standards which should be met when deciding whether to respect or override the expressed preferences of a patient deemed ‘incompetent’, Buchanan and Brock (1989) argue that it is important to be clear about what statements of competence refer to. Like Gert et al (1997), cited earlier, they argue that statements of competence (i.e. in clinical contexts) usually refer to a person’s competence to do something, in this instance, to choose and make decisions; by this view, competence is, therefore, ‘choice and decision-relative’. Given this, determining competence in health care contexts fundamentally involves determining a person’s ability to make particular choices and decisions under particular conditions (Buchanan & Brock 1989: 311–65; see also Mukherjee & Shah 2001).
An important problem particularly in psychiatric contexts is that severe mental illness can significantly affect the capacities needed for competent decision-making (for instance, understanding, reasoning and applying values), and hence the ability generally of severely mentally ill persons to make sound decisions about their own wellbeing — including the need for care and treatment (Buchanan & Brock 1989). For example, as Buchanan and Brock comment (p 318):
a person may persist in a fixed delusional belief that proffered medications are poison or are being used to control his or her mind. Such delusions or fixed false beliefs obviously may also impair a person’s capacity to reason about whether hospitalisation and treatment will on balance serve his or her wellbeing. Severe mental illness can also affect and seriously distort a person’s underlying and enduring aims and values, his or her conception of his or her own good, that one must use in evaluating hospitalisation and treatment for an illness.
It is precisely in situations such as these that attending health care professionals need a reliable framework within which to decide how best to act — notably: (1) whether to respect a patient’s preferences even though the patient is deemed ‘incompetent’, or (2) whether to override patients’ preferences in the interests of protecting or upholding what has been deemed by others to be in the patient’s overall ‘best interests’. Just what such a framework would — or indeed should — look like is, however, a matter of some controversy. Nevertheless, as Buchanan and Brock’s substantive work Deciding for others: the ethics of surrogate decision-making (1989) has shown, it is possible to devise at least a prima-facie working framework to guide professional ethical decision-making in this sensitive, complex and problematic area. Specifically, Buchanan and Brock (1989: 84–6) suggest that the whole issue hinges on:
1. setting and applying accurately standards of competency to choose and decide; and
2. achieving a balance between (i) protecting and promoting the patients’ wellbeing (human welfare), (ii) protecting and promoting the patients’ entitlement to and interest in exercising self-determining choices, and (iii) protecting others who could be harmed by patients exercising harm-causing choices.
In regard to setting and applying accurately standards of competency to choose and decide, Buchanan and Brock suggest that, among other things, ethical professional decision-making in this problematic area should be guided by the following considerations (1989: 85):
No single standard of competence is adequate for all decisions. The standard depends in large part on the risk involved, and varies along a range from low/minimal to high/maximal. The more serious the expected harm to the patient from acting on a choice, the higher should be the standard of decision-making capacity, and the greater should be the certainty that the standard is satisfied.
In other words, the extent to which an attending health care professional is bound morally to respect the choices of a person deemed ‘rationally incompetent’ depends primarily on the severity of the risks involved to the patient if her or his choices are permitted. The higher and more severe the risks involved, the higher and more rigorous should be the standards for determining the patient’s decision-making capacity, and the more certain attending health care professionals should be that the patient has met these standards. This framework is expressed diagrammatically in Figure 6.1.
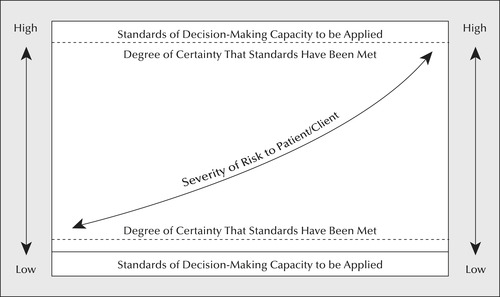
For example, if a patient with severe mental illness chooses to refuse hospitalisation, the extent to which an attending health professional is obliged morally to respect this choice will depend on how severe the risks to the patient are of not being hospitalised — for instance, whether a failure to hospitalise the patient will result in her or him suiciding, or will result only in her or him being left in a state of moderate, although not life-threatening, depression. In the case of suicide risk, the grounds for not honouring a patient’s choices do seem at least prima facie stronger than possible grounds for overriding the choices of a patient who is only moderately depressed. (Whether or not the risk of suicide does provide strong grounds for overriding a patient’s choices to refuse hospitalisation and treatment is another question, however, and one which is considered separately in Chapter 11 of this book.)
While Buchanan and Brock’s (1989) ‘sliding scale’ framework is useful, it is not free of difficulties. For instance, there remains the problem of how to determine what is a harm, what is a low/minimal and high/maximal risk of harm, and who properly should decide these things — the answers to which involve complex value judgments. Consider, for example, the following case (personal communication).
An involuntary psychiatric patient refuses to take the psychotropic medication he has been prescribed. In defence of his refusal, the patient argues ‘reasonably’ that the adverse side effects of the drugs he is being expected to take are intolerable, and that he would prefer the pain of his mental illness to the intolerable side effects of the drugs that have been prescribed to treat his mental illness. Staff on the ward in which he is an involuntary patient are divided about what they should do. The more experienced staff in this case insist that the patient should be given his medication forcibly by intramuscular injection. They argue in defence of this decision that the patient’s condition is deteriorating rapidly, and that if he does not receive the medication prescribed he will ‘spiral down into a psychiatric crisis’ (in other words a total exacerbation of his condition), which would be even more intolerable and harmful than the unpleasant side effects he has been experiencing as a result of taking the psychotropic drugs in question. They make the additional value judgment that it would be ‘better’ for the patient if his psychiatric condition was prevented from deteriorating, and that their decision to administer his prescribed medication forcibly against his will is justified on these grounds.
The less experienced staff on the ward disagree with this reasoning, however, and argue that, even though the patient’s psychiatric condition is deteriorating, and this is a preventable harm, the patient is nevertheless able to make an informed choice about this and therefore his wishes should be respected. In defence of their position, they argue that the patient’s complaints are justified — the adverse side effects of his psychotropic drugs have indeed been ‘awful’, and are commonly experienced by other patients as well; and that he has experienced a decline in his psychiatric condition before, and hence knows what to expect. Further, they argue, if he is given the medication against his will, an even greater harm will follow: specifically, he will trust the nursing staff even less than he does already, and will be even less willing to comply with his oral medication prescription than he is now.
In this case, the more experienced staff outnumbered the less experienced staff, and the patient was held down and forcibly given an intramuscular injection of the medication he had refused. Later, after recovering from this incident, the patient was, as predicted by the less experienced nursing staff, grossly mistrustful of the nursing staff on the ward, and even less willing to comply with his oral medication prescription. His requests for different and less drugs, and more counselling, went unheeded.
This case scenario demonstrates the difficulties that can be encountered when accepting/rejecting a patient’s ability to choose and decide care and treatment options, and deciding when and how to override a patient’s preferences. Not only is there the problem of how to determine accurately what a harm is and how a given harm should be weighted morally when evaluating whether a patient’s choices should be respected or overridden; there is the additional problem that attending health care professionals may disagree radically among themselves about how these things should be determined — to a point that may even cause rather than prevent harm to the patient, as happened in this case. What else then should health care professionals do?
One response is to insist on the development of reliable (research-based) criteria for deciding these sorts of problematic issues. The need to do this becomes even more acute when the problem of determining and weighting harms is considered in relation to the broader demand to achieve a balance between protecting and promoting the patient’s wellbeing, protecting and promoting the patient’s autonomy, and protecting others who could be harmed if a mentally ill person is left free to exercise harm-causing choices (as happened in the Tarasoff case, to be considered later in this chapter).
Just what these criteria should be, however, and how they should be applied, is an extremely complex matter, and one that requires much greater attention than it is possible to give here. Nevertheless, Buchanan and Brock (1989) provide an important starting point by identifying the following three factors which should be (and are already being) taken into consideration when deciding whether to override a mentally ill person’s choices, namely (1) whether the person is a danger to herself or himself, (2) whether the person is in need of care and treatment, and (3) whether the person is a danger to others. In regard to the consideration of being a danger to self, Buchanan and Brock (1989: 317–31) correctly argue that what is needed are stringent criteria of what constitutes a danger to self; in the case of the need for care and treatment, that what is needed are stringent criteria for ascertaining deterioration and distress; and in the case of harm to others, that what is needed are stringent criteria of what constitutes a danger to others. And while applying the criteria developed may inevitably result in a health care professional assuming the essentially paternalistic role of being a surrogate decision-maker for a given patient, this need not be problematic provided the model of surrogate decision-making used is patient centred — that is, committed to upholding the patient’s interests and concerns insofar as these can be ascertained (something which was not done in the case given above).
A patient-centred model of surrogate decision-making, in this instance, would have as its rationale preventing harm to patients, and would embrace an ethical framework which is structured ‘for deciding for patients for their benefit’ (Buchanan & Brock 1989: 327, 331). This is in contrast with a non-patient or ‘other’-centred decision-making model, which would have as its rationale preventing harm to others, and which embraces an ethical framework ‘for deciding about others for others’ benefits’ (pp 327, 331). It should be noted, however, that these two models are not necessarily mutually exclusive and indeed could, in some instances, be mutually supporting (a man contemplating a violent suicide involving others is not only a danger to himself but to the innocent others he plans to ‘take with him’). Just which model or models are appropriate, and under what circumstances they should be used, will, however, depend ultimately on the people involved (and the relationships between them), the moral interests at stake, the context in which these moral interests are at stake, the resources available (human and otherwise) to protect and promote the moral interests that are at risk of being harmed, and, finally, the accurate prediction of possibilities and probabilities in regard to the achievement of desirable and acceptable moral outcomes. This, in turn, will depend on the competence, experience, wisdom and moral integrity of the decision-makers, and the degree of commitment they have to: (1) ensuring the realisation of morally just outcomes, and (2) protecting and promoting the wellbeing and moral interests of those made vulnerable not just by their mental illnesses, but by the inability of their caregivers to respond to the manifestation of their illnesses in morally sensitive, humane, therapeutically effective and culturally appropriate ways.
Paternalism and informed consent
The word paternalism comes from the Latin pater meaning ‘father’, and literally means ‘in the manner of a father, especially in usurping individual responsibility and the liberty of choice’ ( Collins Australian Dictionary 2005). In the bioethics literature, paternalism has been defined in a variety of ways. Literature published in the early 1970s, for example, defined paternalism (construed as a principle viz the paternalistic principle [Beauchamp 1980: 98]) as:
… the interference with a person’s liberty of action justified by reasons referring exclusively to the welfare, good, happiness, needs, interests or value of the person being coerced.
(Dworkin 1972: 65)
Subsequently, paternalism was defined more specifically as:
… interference with a person’s freedom of action or freedom of information, or the deliberate dissemination of misinformation, where the alleged justification of interfering or misinforming is that it is for the good of the person who is interfered with or misinformed.
(Buchanan 1978: 372)
A further modification in definition resulted in the suggestion that for an act to be paternalistic:
There must be a violation of a person’s autonomy … There must be a [sic] usurpation of decision-making, either by preventing people from doing what they have decided or by interfering with the way in which they arrive at their decision.
(Dworkin 1988: 123)
A more recent definition of paternalism holds it to be:
… the intentional overriding of one person’s known preferences or actions by another person, where the person who overrides justifies the action by the goal of benefiting or avoiding harm to the person whose preferences or actions are overridden.
(Beauchamp & Childress 2001: 178)
Early literature on the subject distinguished between two types of paternalism: (1) harm paternalism, and (2) benefit paternalism (Beauchamp 1978a; Beauchamp & Childress 1994). Harm paternalism (underpinned by the principle of non-maleficence) was thought to be justified where it had as its objective protecting individuals from self-inflicted harm. In contrast, benefit paternalism (underpinned by the principle of beneficence) was thought to be justified where it had as its objective securing a good or a beneficence that an individual would not otherwise get — for example, because their liberty is limited. These two forms of paternalism were, in turn, categorised still further, with the following distinctions being made: (1) strong paternalism and (2) weak paternalism, considered below.
In the case of strong paternalism, it was thought to be ‘proper to protect or benefit a person by liberty-limiting measures even when his [or her] contrary choices are informed and voluntary (Beauchamp 1978a: 1197). An example of ‘strong paternalism’ would be where a consultant physician refuses to release a competent although seriously ill patient from hospital even though the patient has requested discharge and knows the potentially fatal consequences of his/her request.
Strong paternalism is in contradistinction to weak paternalism where interference with an individual’s conduct is only justified in cases where that person’s conduct is ‘substantially nonvoluntary or when temporary intervention is necessary to establish whether it is voluntary or not’ (Feinberg 1971: 113, 116). In short, where a person’s autonomy has been compromised in some way (e.g. as a result of pain, drug ingestion, psychogenic distress, physical trauma to the head that interferes with memory, and the like), it is acceptable to paternalistically override a person’s choices or restrain their liberty of conduct. This form of paternalism has been widely accepted in law, medicine and moral philosophy (Beauchamp 2004). An example of ‘weak paternalism’ would be where an attending health care professional attends the scene of a motor vehicle accident and picks up an injured, partially coherent victim and takes him/her to hospital even though the victim has refused an ambulance (Beauchamp 2004: 1985).
As a point of clarification, it should be noted that harm paternalism is thought to be easier to justify and uphold than benefit paternalism. One reason for this is that it was (and is) generally thought, controversially, that we have a greater duty to avoid harm than to promote good — which may not always be within our capacity in given contexts and thus not something for which we could be held morally responsible for not doing. If it was our duty to do or promote good — even where we lacked the resources to do so — this would risk us being condemned as ‘unethical’ for not doing something that we could not do anyway, which would be untenable.
However defined or conceptualised, it should be noted that paternalism remains morally controversial since it always entails the choices or actions of one person being overridden by another without consent. Even if a person’s stated preferences do not originate from a substantially autonomous and authentic choice, ‘overriding his or her preference can still be paternalistic’ (Beauchamp 2004: 1985). This is because, even in the case of ‘diminished autonomy’, persons (e.g. young children, the intellectually disabled and the mentally ill) can still be capable of exercising self-interested choices. It is against this backdrop then that a key question arises, namely: Is paternalism ever justified? and if so, under what conditions?
Is paternalism justified?
The literature reveals at least three possible answers to the question of whether paternalism is justified:
1. pro-paternalism (always justified)
2. anti-paternalism (never justified)
3. prima-facie paternalism (sometimes justified).
These three possible answers are discussed below.
Pro-paternalism (always justified)
Pro-paternalism positions hold that paternalism is always justified to ‘protect individuals against themselves’ (Hart 1963: 31). This position is supported by an appeal to either of the principles of human welfare, beneficence (e.g. as in the case of overriding the harmful choices of children) and/or ‘rational consent’ (meaning consent that ‘would otherwise have been given’); in this instance, paternalism is thought to be justified as a kind of ‘social insurance policy’ for our own protection (Beauchamp 2004: 1986). Further, it is held that sometimes an immediate act of paternalism may, paradoxically, protect a person’s ‘deeper autonomy’, for example, such as in the case of someone who is depressed and suicidal (Beauchamp 1980; 2004). Justificatory considerations for strong paternalism, include the following conditions:
▪ no acceptable alternative to the paternalistic action exists;
▪ risks to the person that are introduced by the paternalistic action itself are not substantial;
▪ projected benefits to the person outweigh risks to the person;
▪ any infringement of the principle of respect for autonomy is minimal.
(Beauchamp 2004: 1987)
Anti-paternalism (never justified)
Anti-paternalism positions hold that paternalism is never justified. This is because paternalism always involves a violation of moral rules, for example, that we ought to respect people’s choices even if we do not agree with them, provided they do not harm others; the individual is sovereign and any coercion or interference with their self-determining choices is morally unacceptable. Acts of paternalism also violate a person’s privacy and fail to treat them as the moral equals of others (Childress 1982, cited in Beauchamp 2004: 1986).
Prima-facie paternalism (sometimes justified)
Prima-facie paternalism (also known as ambivalent-paternalism) holds the position that paternalism is sometimes justified, though severely limited. Any action of coercion against or interference with another’s conduct carries a heavy burden of justification. Paternalism is only justified where:
1. the evils prevented from occurring to the person are greater than the evils (if any) caused by violating the moral rule;
2. it is universally justified under relevantly similar circumstances always to treat persons in this way.
(Gert & Culver 1976)
These three positions may be expressed diagrammatically as shown in Figure 6.2.
 |
| Figure 6.2 |
Despite the apparent differences between these three positions, however, there is some agreement between the positions of ‘weak paternalism’ and ‘anti-paternalism’. These are (Beauchamp 2004: 1986):
(i) it is justifiable to interfere in order to protect persons against harm from their own substantially non-autonomous decisions; and
(ii) it is unjustifiable to interfere in order to protect persons against harm from their own substantially autonomous decisions.
One reason for this closeness in position is that, as some contend, ‘weak paternalism’ is not really paternalism at all since it cannot be substantively distinguished from anti-paternalism. In the ultimate analysis both rest on the principles of beneficence and non-maleficence, and both reject strong paternalism (which justifies overriding strongly autonomous choices). However, when it is considered that even strong paternalism rests on the principles of beneficence and non-maleficence, the differences between all three positions may, in the end, be overstated.
Applying the ‘paternalistic principle’ in health care
Applying the ‘paternalistic principle’ in health care contexts is not clear-cut and indeed raises a number of important questions, such as: How are we to justify overriding another’s choices? What constitutes beneficial and harmful outcomes for the patient? What constitutes a patient’s ‘best interests’? How are we to measure the quality of another’s autonomy and autonomous choices? Do people have the right to refuse life-saving/enhancing treatment? What if treatments are ‘harmful’?
The abuses of paternalistic decision-making and the rise of individualism and ‘patients’ rights’ in the 1970s and 1980s saw a backlash against paternalism in health care. The past three decades have, however, seen a tempering of this rejection (see also Gert et al 1997; Beauchamp & Childress 2001). As Beauchamp concludes (2004: 1989):
Paternalism seems likely to continue to be a viewpoint that will gain or lose adherents as the issues and larger social context shift. We may never again see the concentrated flurry of scholarly interest in this subject that was exhibited from the mid-1970s to the mid-1980s, but paternalism is not likely to be an issue that will soon disappear.
One author has argued controversially that medical paternalism in health care contexts (which he states is often practised ‘covertly’) is not only here to stay, but is ‘essential’ to ethical practice and the promotion of patient autonomy; he writes:
Although patient autonomy is dominant in current ethical discussions, medical paternalism is not extinct. Indeed it cannot become so, for the exercise of paternalism is essential to the practice of medicine. After all, we are the medical experts, and we are required to recommend what is medically best for the patient. It is therefore arguable that some measure of paternalism is involved in most treatment decisions. This covert paternalism is not necessarily bad, provided it is recognised for what it is, and is used appropriately to guide and support patient autonomy rather than to override it.
(Tweeddale 2002: 236)
Informed consent and nurses
In light of what has been discussed thus far, there is considerable scope to suggest that nurses have much to contribute to the informed consent/decision-making debate. Further, it is clear that the nursing profession needs to pay much greater attention to the doctrine of informed consent and its moral implications for nurses — not least the duties it imposes on nurses to obtain patients’ informed consent to nursing care and procedures, and the issues it raises concerning ‘nursing paternalism’. It is perhaps important to emphasise that, although the doctrine of informed consent has traditionally been discussed primarily in regard to medical treatment and care, the underlying moral values, moral principles and moral requirements of this doctrine apply equally to other kinds of health care practices and procedures, including nursing care and procedures. This is because nurses are no less exempt than are any other health care professionals from the moral standards governing consent procedures, including the demands to:
▪ disclose all relevant information necessary for making an informed choice about proposed nursing cares and procedures
▪ ensure that the patient understands the information received and the implications of giving consent
▪ ensure that the consent is given voluntarily (that is, that nurses do not coerce or manipulate the patient into giving consent)
▪ ensure that the patient has the capacity to make an informed choice, and, if not, that any surrogate decision-making on the patient’s behalf is in accordance with rigorous moral standards.
Likewise the issue of paternalism. Although paternalism has primarily been discussed in regard to the profession of medicine (medical paternalism), the issues raised apply just as well to nursing (nursing paternalism). These issues both stand as fertile ground for further debate, research and scholarship.
T he right to confidentiality
The principle of confidentiality has long been recognised as an important and fundamental guide to action in — and even the cornerstone of — effective health professional–client relationships (McMahon 2006). This principle is reflected in law as well as in ethics. Insofar as the law is concerned, Forrester and Griffiths (2005: 74) explain health legislation at state, territory and Commonwealth levels ‘impose obligations on health professionals to protect client information from disclosure or unauthorised use in specified circumstances’. There are, however, notable exceptions to this duty, including:
▪ the patient (or his/her lawful representative) has consented to the disclosure
▪ there is the presumption of ‘implied consent’ for other health professionals to access patient information to enable the provision of continuous care
▪ disclosures are mandated by law (e.g. notification of known or suspected cases of child abuse/elder abuse, suspicious injuries, commission of serious offences, manifestation of ‘notifiable diseases’ — e.g. infectious and sexually transmitted diseases)
▪ disclosures are ‘in the public interest’ — that is, where the patient has been identified as posing a threat either to a third party or to themselves.
(adapted from Forrester & Griffiths 2005: 75–6)
There are widely divergent views among health professionals and patients/clients about the nature and ‘bindingness’ of confidentiality, and the degree to which it is, in practice upheld (Jansen & Friedman Ross 2000; McMahon 2006; Mulligan & Paterson 2003; Winslade 1995). Furthermore, whereas the professional duty to maintain patient confidentiality was once regarded as being absolute, growing dissatisfaction with this stance has seen a significant shift in both policy and practice in recent years, with most health professional codes and guidelines now recognising the duty to maintain confidentiality as being at best prima facie (discretionary), not absolute in nature (McMahon 2006). For example, whereas the 1983 version of the World Medical Association (WMA) International Code of Medical Ethics took an absolutist position on confidentiality, stating: ‘A physician shall preserve absolute confidentiality on all he [sic] knows about his [sic] patient even after the patient has died’ [emphasis added] (p 6), the 2006 version of the code takes a much more circumspect position. The 2006 version of the code states:
A physician shall respect a patient’s right to confidentiality. It is ethical to disclose confidential information when the patient consents to it or when there is a real and imminent threat of harm to the patient or to others and this threat can be only removed by a breach of confidentiality.
The Australian Medical Association’s Code of Ethics also recognises that ‘information may be divulged with the patient’s permission’ and that ‘exceptions may arise where the health of others is at risk or you [the doctor] are required by order of a court to breach patient confidentiality’.
Nursing codes and guidelines take a similar stance. The ICN Code of Ethics for Nurses, for example, states: ‘The nurse holds in confidence personal information and uses judgment in sharing this information’ (ICN 2006: 2). The ANMC (2008b) Code of ethics for nurses in Australia (Value Statement 7) in turn, states:
The ethical management of information entails respecting people’s privacy and confidentiality without compromising health or safety. This applies to all types of data, including clinical and research data, irrespective of the medium in which the information occurs or is stored, and includes oral, written, statistical and computerised data.
Confidentiality as an absolute principle
As briefly mentioned in the opening paragraphs of this section, there has been a significant shift in the way in which the duty of confidentiality is regarded and practised in health care contexts. Historically, the principle of confidentiality was interpreted as an absolute principle. In application it was (and still is in some contexts, e.g. the priest confessional) taken as demanding that information gained in a professional–client relationship must be kept secret, even when its disclosure might serve a greater public good. An example of the extent to which confidentiality was once regarded by professionals (especially doctors) as being absolute can be found in a 1904 case in which a physician refused to warn a prospective victim that her fiancé was a syphilitic, thereby risking both her and her offspring being exposed to the disease (Bok 1980). Commenting on the case, the physician wrote (p 147):
A single word […] would save her from this terrible fate, yet the physician is fettered hand and foot by his cast-iron code, his tongue is silenced, he cannot lift a finger or utter a word to prevent this catastrophe.
In another case, reported in the British Medical Journal (BMJ) in 1906, the duty of the doctor to maintain absolute confidentiality was again emphasised. The case involved a man who suffered from asthma and who sometimes became distressed and had even collapsed with his condition — although never while at work. Employed as the sole operator of a railway signal box, and fearing he would lose his job if his employer knew of his medical condition, the man refused to disclose his condition to his employer. Of this case, the editor of the BMJ commented:
The circumstances, extreme though they be, cannot be held to justify a breach of the law of professional secrecy […] the doctor ought not to write direct to the railway company without the patient’s consent, and unless he fully understands the nature of the communications to be made.
(BMJ 1906, cited in McMahon 2006: 567)
Over the past three decades, however, both real and hypothetical cases have exposed the inappropriateness and moral unacceptability of holding confidentiality as being an absolute principle (i.e. cannot be breached under any circumstances).
It is now widely recognised that in cases where innocent victims stand to be significantly harmed by a failure to disclose, the demand to breach confidentiality becomes morally compelling. This was the view taken in the noted US legal case Tarasoff v Regents of the University of California (1974). The case involved a university student, Prosenjit Poddar, who had met and became infatuated with a young woman, Tatiana Tarasoff. Unfortunately, Tarasoff did not share Poddar’s feelings, and told him so. Consequently, Poddar became very depressed and sought psychiatric help on a voluntary outpatient basis at the Cowell Memorial Hospital at the university. During a consultation with his psychologist, Dr Lawrence Moore, Poddar revealed that he seriously intended to kill Tarasoff. After receiving this information the psychologist wrote to the campus police and informed them that Poddar was ‘at this point a danger to the welfare of other people and himself’, also pointing out that Poddar had been threatening to kill an unnamed girl who he felt had ‘betrayed him’ and had ‘violated his honour’ (Daley 1983: 243). The psychologist then went on to ask the police for assistance in detaining Poddar for psychiatric assessment. Daley writes that the campus police detained Poddar ‘but released him when he appeared rational and promised to stay away from Tarasoff’ (p 235).
Following this, Poddar’s psychologist was directed by a superior to take no further action and to destroy his client’s records (a practice which is sometimes followed by psychologists, psychotherapists and psychiatrists in order to ensure confidentiality). Two months later, as he had threatened to his psychologist, Poddar carried out his intention and killed Tarasoff with a butcher’s knife.
Daley (1983) notes that neither the girl nor her parents were warned of Poddar’s threat. It seems that none of the psychotherapists involved considered it part of their professional morality to warn the victim. Even the California Supreme Court acknowledged recognition of the general rule that ‘there is ordinarily no duty to control the conduct of another or to warn those endangered by such conduct’ (p 235). However, the Supreme Court also recognised certain exceptions to the general rule, and its final decision in the Tarasoff case imposed a new duty to warn upon doctors and psychiatrists under its jurisdiction. The psychiatric profession ‘reacted with alarm’ to the California Supreme Court’s ruling, claiming that it would ‘cripple the use of psychotherapy by destroying the confidentiality vital to the psychiatrist–patient relationship’ (p 234).
In Australia, the duty to warn an intended victim at risk of harm by another became the subject of media commentary and controversy after a Sydney woman, who contracted HIV from her husband, ‘successfully sued the medical practice where the couple had received premarriage testing for sexually transmitted diseases’ (Lamont 2003: 1). The woman (who was in her late twenties) sued the practice for failing to tell her of her husband’s HIV-positive status. Damages of $727000 were awarded to the woman on the grounds that ‘the doctors had not adequately counselled either partner about their results’ ( The Age 2003: 14). The woman only learned about her husband’s HIV-positive status 15 months after they had both been tested when she found a laboratory report showing that her husband was HIV-positive; previously, the husband had shown her a falsified report declaring him to be HIV-negative. Although the court upheld the principle of doctor–patient confidentiality and affirmed that ‘doctors cannot be sued for damages by maintaining the confidential relationship’, it also affirmed that doctors ‘must safeguard patients through proper counselling protocols and, if necessary, notify the Director of General Health, who has the power to breach confidentiality and directly warn someone they are at risk of infection’ (Lamont 2003: 1). An editorial appearing in The Age, concluded (2003: 14):
Doctor–patient confidentiality is an important principle and policy-makers are right to do their utmost to uphold it. But human life is even more precious and doctors have a duty to do all they can to protect those whom they believe are at risk.
The Tarasoff case and others like it (such as the Sydney case, cited above) raise interesting and thought-provoking questions about the nature and force of the principle of confidentiality and the extent to which health professionals are obliged morally to uphold it.
In general the demand to keep secret information disclosed in a professional–client relationship is thought to derive from the broader moral principles of autonomy, non-maleficence, justice and the obligation to keep one’s promises. In the case of autonomy, it is held that individuals are entitled to choose who should have access to information about themselves, as well as what information should be disclosed, if any. Non-maleficence, on the other hand, demands that people are entitled to be protected from the harms that might flow from disclosure (which, as we know, can be both considerable and intolerable). And justice demands that a person, about whom ‘private’ information is known, deserves to be treated fairly. Promise-keeping, simply put, demands that ‘added respect is due for that which one has promised to keep secret’ (Bok 1980: 149), although it is generally recognised that a promise to do morally evil things is either not binding at all or ‘deficient in its binding power’ (Freedman 1978: 12).
In health care contexts, the supremacy of the principle of confidentiality is thought to be particularly justified on grounds that it is crucial to preserving the fiduciary (trust) nature of the health professional–patient relationship (Beauchamp & Childress 2001; Gert et al 1997). If patients/clients can trust their attending health professionals to keep secret certain information disclosed in the professional relationship, it is thought that patients/clients will be more likely to reveal information crucial for making a correct assessment/diagnosis, and thus a correct prescription of care and treatment.
Understandably, if it were common practice to breach confidentiality, patients/clients would probably lose their trust and confidence in their attending health care professionals, and would probably refrain from divulging critical information to them. Worse, they might not seek professional help at all — something which might have the undesirable consequence of individuals, groups and indeed the community at large, suffering a health status inferior to that which might otherwise be enjoyed.
The question remains, however, of whether the principle of confidentiality really is as binding as professionals seem to think it is. Where does it come from? And, as Bok (1980: 154) correctly asks: ‘Was it ever meant to stretch so far as to require lying?’; ‘Why is it so binding that it can protect those who have no right to impose their incompetence, their disease, their malevolence on ignorant and innocent victims?’
In answering these questions, it is important to understand the nature of the principle of confidentiality and why, up until recently, it has been problematic in health professional practice. If we examine its parent principles, that is, the broader moral principles from which it has been derived, we can soon see why an absolutist view of confidentiality is questionable and why the shift towards accepting it as being a prima-facie duty is more compelling.
Confidentiality as a prima-facie principle
On close analysis it can be seen that, at best, the principle of confidentiality is, and can only ever be, a prima-facie principle. Confidentiality has a special link to a person’s right to privacy, which may be loosely defined as the right to ‘have control over information about ourselves’ or ‘control over who can sense us’ (Parker 1974; McCloskey 1980; Thomson 1975). This in turn is connected with the principle of autonomy, which demands that people should be respected as autonomous choosers, and have the right to act on their choices provided these do not seriously impinge on the moral interests of others. Given this, it seems reasonable to hold that, where the maintenance of confidentiality results in the moral interests of others being violated, the principle can and must be overridden. This conclusion is also partially supported by the principles of non-maleficence and justice. Thus, in instances where keeping a confidence or a secret has the unhappy consequence of causing or failing to prevent an otherwise avoidable harm, and/or indeed results in an unequal distribution of harms over benefits, there is a very strong case supporting disclosure of the information being kept secret.
When subjected to the scrutiny of broader moral principles, it can be seen, first, that there are serious limits to the duty of secrecy and of maintaining confidentiality. Second, it is clear that, while in some instances the norm of confidentiality might justifiably extend to include lying, this does not hold unconditionally in all cases. (Given a consequentialist analysis, lying can only ever be justified on the grounds that it is necessary to prevent an otherwise avoidable harm from occurring, and where there is no other alternative action which can be taken to prevent the foreseen harm in question.) Third, it can be seen, given the competing demands of the moral principles of non-maleficence and justice, that the principle of confidentiality can never be used morally to protect those who would impose their incompetence, their diseases and their malevolence on to innocent and uninformed victims.
Unfortunately, the moral principle of confidentiality has sometimes been (ab)used to prevent the disclosure of unscrupulous practices. A poignant example of this can be found in the Chelmsford case referred to in Chapter 5. Of particular relevance to this discussion is the point that, after the 60 Minutes program in 1977, when some advice was sought by medical authorities on how to deal with the Chelmsford case, the principle of confidentiality was used to impose a duty of silence on the matter, or at least to delay its exposure. When, for example, an eminent professor of psychiatry at Cambridge University was approached about the matter, he advised:
The inhumanity and cruelty to which the patients appear to have been subjected is quite unique in my experience, and the Scientologists and other organisations will have obtained ammunition for decades to come. There is therefore a pressing need for maintaining strict confidentiality at this stage until one can set these unique barbarities in the context of contemporary practice in psychiatry in a carefully prepared statement that comes from colleges and other bodies concerned.
(Sir Martin Roth, cited in Bromberger & Fife-Yeomans 1991: 143)
This appeal to the principle of confidentiality is questionable, and stands as an example of how conventional ethical principles of conduct can be (ab)used to maintain and reinforce the status quo rather than to challenge it. Further, when more parochial interpretations and applications of the principle of confidentiality are considered, what emerges is not a respect for ethical conduct, but rather what Bok (1980) describes as ‘primeval tribal emotions: the loyalty to self, kin, clansmen, guild members as against … the unrelated, the outsiders, the barbarians’ (p 149). Bok (p 149) concludes by warning that the principle of confidentiality can sometimes serve little more than the drive for ‘self-preservation’ and ‘collective survival in an hostile environment’. The Chelmsford case is an example of this.
It is not being argued here that the principle of confidentiality ought not to be respected. On the contrary: confidentiality is an important moral requirement of any health care professional–patient/client relationship, and one that is crucial to ensuring the protection of a patient’s/client’s wellbeing and moral interests. Indiscriminate breaches of confidentiality can have morally undesirable and catastrophic consequences for patients/clients. For example, careless breaches of confidentiality concerning persons who are HIV-positive can result — and have resulted — in people being dismissed from their jobs, being evicted from their rented accommodation, and being subjected generally to a wide range of negative discrimination and abuse. Similarly, careless breaches of confidentiality concerning a person’s mental health status (including mild depression and grieving states) can also result — and have resulted — in harmful consequences, including persons losing their jobs or having their career prospects hampered (see also Johnstone 2001). It is crucial, therefore, that every effort is made to ensure that information disclosed in the professional–client relationship is kept secret. This is not to say, however, that there is not a need for the principle of confidentiality to be interpreted better and applied more justly than it has been in the past. Points of clarification which need to be particularly addressed are summarised as follows:
▪ confidentiality is at best only a prima-facie principle, not an absolute one, and thus is one which may be overridden by stronger moral considerations
▪ confidentiality should not be upheld in instances where doing so would result in otherwise avoidable harms occurring to innocent others
▪ while patients/clients as a general rule have an entitlement to have certain information about themselves kept secret, the entitlement is forfeited where it stands seriously to impinge on the moral interests of innocent others.
In light of the above, it can be seen that patients (and others) might not always be entitled to have certain information about themselves kept secret; and that disclosure, in some instances, might even be an overriding moral duty, particularly in cases where non-disclosure entails the probability of innocent others suffering unnecessary and avoidable harms (e.g. children as in the case of child abuse). As indicated earlier in this discussion, this second demand is also reflected in legal law, which requires health professionals to report certain notifiable diseases, suspected cases of child abuse (to be examined in depth in Chapter 8 of this work), and other activities ‘which [are] potentially or actually dangerous to the health of others’ (Wallace 1991: 303).
Whatever the situation at hand, nurses’ decisions to keep secret or to disclose certain information gained in a professional–client or other type of relationship (e.g. an employee–employer relationship) must always be based firmly on sound moral justifications and moral decision-making procedures. Nurses also need to remember that arbitrary disclosure is just as morally capricious as arbitrary non-disclosure, and may have just as many devastating consequences. As in any morally troubling situation, dilemmas posed by a controversial application of the principle of confidentiality must be resolved in a way which ensures the realisation of morally just outcomes.
T he right to be treated with dignity1
According to Article 1 of the Universal Declaration of Human Rights (1948) ‘All human beings are born free and equal in dignity and rights.’ The right to dignity as implied in this statement (and which encompasses the rights of people to uphold their own dignity as well as to be treated with dignity by others) and its implications for the health and wellbeing of people have, however, been poorly addressed in the health professional literature. Although the right to die with dignity has been widely considered in the bioethics and nursing literature (too voluminous to list here), and has gained popular usage in contemporary debates on the provision and limits of invasive medical treatment at the end stages of life, it is important to clarify that the right to dignity involves considerably more than merely the right to die with dignity. Furthermore, although the terms ‘dignity’ and ‘dying with dignity’ have been and are freely used in discussions and debates on end-of-life care, there is room to question whether those who use them have a clear understanding of what precisely they mean.
Another concern is that these terms have come to be used in a rather clichéd sense, and thus could have the undesirable consequence of a blanket definition of dignity being applied uncritically in all situations, regardless of their ethically significant differences, and in a way which could result in a serious distraction from (rather than a focus on) the moral issues at stake. For example, some speak of the removal of a life-support system, or the withdrawal of some other orthodox medical therapies, as tantamount to ‘letting a person die with dignity’ (Social Development Committee, Parliament of Victoria 1986, 1987). What such views presume, however, is that the terms ‘dignity’ and ‘dying with dignity’ in these contexts have a clear-cut, commonsense meaning and use, and, furthermore, implicitly justify the acts or omissions in relation to which they have been expressed. This usage also seems to treat the right to dignity as being synonymous with the right to die with dignity, which is wrong and misleading since the right to die with dignity is just one of several kinds of dignity rights claims that a person might exercise.
Two key questions arise here: What is dignity and what is meant by the right to be treated with dignity?, and What might be the implications of, given definitions of dignity, the right to be treated with dignity for members of the nursing profession?
What is dignity?
The word dignity comes from the Latin dignitas, meaning ‘merit’, and dignus, meaning ‘worthy’. Needless to say, there are as many definitions of ‘dignity’ as there are dictionaries. Collins Australian Dictionary, for example, defines dignity as:
[1]..a formal, stately, or grave bearing … [2]. the state or quality of being worthy of honour … [3]. relative importance; rank … [4]. sense of self importance …
According to the Oxford English Dictionary, dignity is:
[1]. the quality of being worthy or honourable; worthiness, worth, nobleness, excellence … [2]. Honourable or high estate, position, or estimation … [4]. Nobility or befitting elevation of aspect, manner, or style …
Webster’s Dictionary says dignity is:
[1] the quality or state of being worthy: intrinsic worth: EXCELLENCE …
[2] the quality or state of being honoured or esteemed: degree of esteem …
[5] formal reserve of manner, appearance, behaviour, or language: behaviour that accords with self-respect or with regard for the seriousness of occasion or purpose …
Interestingly, the unabridged international edition of Webster’s Dictionary also gives consideration of the word ‘decent’ (i.e. of the mind and character) as a definition of dignity. It is perhaps worth noting here that the term ‘decent’ comes from the Latin decens, meaning ‘suitable’, and from decere, meaning ‘to be fitting’.
The question of dignity has also been a topic of significant philosophical debate. For example, in 1651 the English philosopher Thomas Hobbes defined it as (1968: 52):
(T)he publique worth of a man [sic], which is the Value set on him [sic] by the Common-Wealth … And this Value of him [sic] by the commonwealth, is understood, by offices of Command, Judicature, public Employment; or by Names and Titles, introduced for distinction of such Value.
Later philosophers, however, rejected this ‘social worth’ view and sought to define dignity in more sophisticated moral terms. The German philosopher Immanuel Kant, for instance, defines dignity in quite different terms as ‘an intrinsic, unconditioned, incomparable worth or worthiness’ (1972: 35). Rejecting the ‘market value’ or ‘social worth’ interpretations of dignity, he goes on to assert that:
Morality or virtue — and humanity so far as it is capable of morality — alone has dignity. In this respect it cannot be compared with things that have economic value (a market price) or even with things that have an aesthetic value (a fancy price). The incomparable worth of a good man [sic] springs from his [sic] being a [moral] law making member in a kingdom of ends.
(Kant 1972: 35)
More recent definitions and interpretations have tended to capture the essence of Kant’s views. One philosopher, for example, argues that dignity is akin to ‘justified happiness’ (a happiness which is ‘interpenetrated with a sense of meaning, reason, and worth’) and the attainment of ‘just goals’; that is, morally valuable ends (Swenson 1981). The behaviourist B F Skinner (1973: 48–62) sees dignity and what he calls the ‘struggle for dignity’ as having many features in common with freedom and the ‘struggle for freedom’.
Some of the most revealing and instructive definitions of dignity, however, come from a group of first-year undergraduate nursing students from the former Phillip Institute of Technology (now RMIT University). Comments were sought from the students after their clinical placement at a residential care home for the elderly. The results are summarised as follows.
▪ ‘Dignity is concerned with self-respect, and how this is related to society — your social worth.’
▪ ‘Dignity is a feeling of pride … of feeling good about yourself.’
▪ ‘Dignity is having pride without shame.’
▪ ‘Dignity is being accepting of one’s self, and of what’s to come … the problem is, however, that a lot of people base their self-worth on what other people think of them.’
Dying with dignity, in turn, was described by the students in the following terms:
▪ ‘Dignity and dying with dignity is being happy with oneself, and what one has achieved in life.’
▪ ‘Dying with dignity is dying the way you want to die.’
▪ ‘Dignity and dying with dignity is maintaining self-value, self-respect and self-image …’
▪ ‘Dying with dignity is having no pain, no fear. Feeling valued, and having your opinions valued. Yes. That’s it! It involves having control and being valued.’
▪ ‘Dying with dignity is putting yourself above whatever is going on around you.’
In considering all these definitions, it soon becomes apparent that there may be as many definitions of ‘dignity’, and ‘dying with dignity’, as there are people trying to define it. The lesson to be learned from this is that nurses — and indeed health care professionals generally — must never take the notion of dignity (and its usage) for granted. They must also be cautious in treating these terms as if they had clear-cut, commonsense interpretations. What one person might consider ‘dignity’, another person might equally reject — and this has important implications for nursing care delivery in particular, and health care management generally.
Dignity and the right to dignity
Despite the variety of definitions and interpretations of the notion ‘dignity’, there are a number of common elements which may be encapsulated in a working definition of dignity. In summary, these include:
▪ that persons have intrinsic moral worth, and thus ought to be treated with respect (see discussion on the right to be treated with respect, below [pages 176-8])
▪ that persons should be respected as autonomous choosers, and thus as beings capable of exercising self-determining choice
▪ that persons should be facilitated and supported in the course of exercising their autonomous choices
▪ that persons should be facilitated and supported in their attempts to maintain their self-respect and self-esteem.
Taking these elements into account, the right to dignity (encompassing the rights to uphold one’s own dignity and to be treated with dignity by others) may, in turn, be taken to mean: a special interest that persons have in being treated as entities with intrinsic moral worth, whose autonomy and capacity for exercising self-determining choices ought to be respected, and who ought to be supported and facilitated in their attempts to maintain self-respect and self-esteem.
Dignity violations
Before concluding this discussion on the right to dignity, some comment on the notion of ‘dignity violations’ and its possible implications for the health and social wellbeing of people is warranted.
According to the late Jonathan Mann, Professor of Health and Human Rights at the Harvard School of Public Health, there exists a critical relationship between dignity — or rather ‘dignity violations’ — and the health and social wellbeing of people (Mann 1997: 11). Although conceding that a satisfactory definition of dignity is both complex and elusive, Mann is adamant that we can nonetheless know when our ‘dignity is violated or impugned’. Moreover, by undertaking an exploration of dignity (what it means and what forms violations of it might take) we may uncover new and important understandings of human suffering and progress the human effort that is needed to redress this suffering as a health and human rights issue (Mann 1997: 11). Mann’s thoughts on this are worth quoting in full; he states:
… it seems we all know when our dignity is violated or impugned. Perform the following experiment: recall, in detail, an incident from your own life in which your dignity was violated, for whatever reason. If you will immerse yourself in the memory, powerful feelings will likely arise — of anger, shame, powerlessness, despair. When you connect with the power of these feelings, it seems intuitively obvious that such feelings, particularly if evoked repetitively, could have deleterious impacts on health. Yet most of us are relatively privileged, we live in a generally dignity-affirming environment, and suffer only the occasional lapse of dignity. However, many people live constantly in a dignity-impugning environment, in which affirmations of dignity may be the exceptional occurrence. An exploration of the meanings of dignity and the forms of its violation — and the impact on physical, mental, and social well-being — may help uncover a new universe of human suffering, for which the biomedical language may be inapt and even inept.
(Mann 1997: 11–12)
For Mann, dignity is a fundamental precursor of the realisation of human rights that, in turn, is a linchpin to the realisation of the goals of health (Mann 1997; Mann et al 1994, 1999). Realising this connection, meanwhile, serves to also reveal ‘the rights-related responsibilities of physicians and other health care workers’ to make allies of public health and human rights and to push for a ‘new’ ethics of the public’s health (Mann 1997; Mann et al 1994, 1999).
Implications for nurses
Whatever nurses or allied health workers take dignity and its various applications to mean, it is important that they do not unfairly impose their interpretations on their patients. It is morally imperative that patients’ preferences (which might include them abdicating their autonomy to a surrogate decision-maker) are respected, even if others do not agree with these. This means that, where possible, and in a manner that is culturally appropriate, patients are morally entitled to participate in decision-making concerning their care, and are morally entitled to give a fully informed consent to the use and withdrawal of recommended medical or other therapies. If patients are not able to participate in decision-making concerning their care and treatment, every effort must be made to establish what their considered preferences might be. Either way, in the final analysis, what is to count as dignity — whatever the health care situation and context — must be decided from the patients’ (or their advocates’) point of view, not that of the health professionals.
Given this, nurses should not be asking ‘What is dignity?’, but ‘What is dignity for this or that person?’ The challenge to nursing is not just to allow patients the right to be treated with dignity or the maintenance of dignity, but actually to find out what the patient considers as being dignity, and ensuring that this is permitted and upheld on terms of what the patient wants, and not on what the nurse thinks the patient wants.
T he right to be treated with respect
Related to the right to be treated with dignity, is the right to be treated with respect. People (whatever their age, cultural backgrounds, sexuality, social position, and so forth) have a special interest in being treated with respect. Furthermore, there are significant moral reasons why this interest ought to be protected. Thus, the claim that people have a right to be treated with respect is a meaningful one.
Underpinning most moral claims (rights claims included) is the principle that people ought to be treated with respect. Otherwise referred to in moral philosophy as ‘respect for persons’, this principle is generally regarded as being of paramount importance to the establishment, development and maintenance of moral relationships between people, and to moral practice generally (Tadd 1998: 1–3).
The notion of ‘respect for persons’ is widely used, often without qualification, in the bioethics literature (its meaning more or less taken for granted), and, of significance to this discussion, it is widely used in codes of professional ethics. For instance, common to most nursing codes of ethics is a prescribed demand to ‘respect patients’ in the provision of nursing care. This demand tends to be interpreted in varying ways as including an obligation to treat with respect a patient’s needs, values, beliefs and culture. As well, nursing codes of ethics prescribe respect for patients’ rights. Consider the following examples.
The Preamble to the International Council of Nurses’ (2006) Code of Ethics for Nurses states:
Inherent in nursing is respect for human rights, including cultural rights, the right to life and choice, to dignity and to be treated with respect. Nursing care is respectful of and unrestricted by considerations of age, colour, creed, culture, disability or illness, gender, sexual orientation, nationality, politics, race or social status.
The Australian Nursing and Midwifery Council’s (2008b) Code of Ethics for Nurses in Australia takes a similar position. The introduction to the code states:
The nursing profession recognises the universal human rights of people, and the moral responsibility to safeguard the inherent dignity and equal worth of everyone. This includes recognising, respecting and, where able, protecting the wide range of civil, cultural, economic, political and social rights that apply to all human beings.
The Nursing Council of New Zealand’s Code of Conduct for Nurses (2005) also emphasises the respect for patients’ rights. Principle three of the code states: ‘The nurse respects the rights of patients/clients.’
Despite the term’s common use in the ethics literature and in codes of ethics, however, just what constitutes ‘respect’ and ‘respect for persons’ has received surprisingly little attention by authors. In the remainder of this chapter an attempt will be made to remedy this oversight. Specifically, brief attention will be given to exploring the nature and moral implications of ‘respect’ and ‘respect for persons’ — particularly as these pertain to the ethical practice of nursing and the promotion of patients’ rights generally.
Every culture has its own conception of respect and ‘its own norms of behaviour and ways of being that are considered respectful’ (Sugirtharjah 1994). Asian cultures, for example, tend to treat respect as a moral duty expressed through such concepts (tautologically) as: duty, respect and honour (Sugirtharjah 1994). Western cultures, however, tend to give greater primacy to respect as an individual moral right (Sugirtharjah 1994: 740).
Western conceptions of respect and, specifically, the principle of respect for persons has borrowed heavily from the work of the 18th century German philosopher, Immanuel Kant. In his celebrated work Fundamental principles of the metaphysics of ethics, Kant (1959: 56) prescribes the (now famous) practical imperative: ‘So act as to treat humanity, whether in thine own person or in that of any other, in every case as an end withal, never as means only.’ This practical imperative has been variously translated to mean that people should always be treated as ends in themselves, and never as mere means (for instance, as objects) to the ends of others. Although commonly accepted, this conception of ‘respect for persons’ is, however, demonstrably inadequate and requires expansion to enhance its usefulness as a guiding principle in health care domains. There is, for instance, considerable scope to suggest that respecting persons entails something far more than fulfilling the negative duty of not treating individuals as ‘mere means’ to the ends of others. It also involves the positive duty of treating people in a manner that is affirming of their personal identity as dignified human beings, that is, affirming of who they are.
In clarifying the nature and moral implications of rights claims involving respect in health care contexts, it is important first to draw a distinction between respecting persons per se, and respecting the rights of persons. While the latter is obviously a critical ingredient of the former, the two are nevertheless distinct. In regard to the latter, respecting the rights of persons means honouring a range of special interests (moral entitlements) that people might have, say, upon entering a health care domain; for example, the right to health care, to make informed choices, to have information about themselves treated as confidential, to be treated with dignity, to cultural liberty and to be treated with respect itself. Moral demands to treat persons with respect, in contrast, is fundamentally tied to enhancing the self-identity of persons and involves, in complex ways, acknowledging persons for who they are and responding to them in a manner that prima facie preserves the integrity of their self-identity and the promotion of moral goods that this preservation will facilitate. Let us explore this claim further.
Respect (from the Latin respicere, meaning ‘to look back, pay attention to’, from specere, meaning ‘to look’) is essentially a moral attitude that when translated into action is manifest as the showing of admiration, regard, esteem, and/or kindly consideration for another. In short, respect manifests as the ‘good’ treatment of people, and invariably results in their being ‘humanised’ (that is, enabled to experience their ‘beingness’ both as human persons and as moral entities, and/or characterised as having moral worth). Disrespect, in contrast, manifests as the ‘bad’ (or ill) treatment of people, and invariably results in them being ‘dehumanised’ (deprived of qualities that otherwise enables them — and others — to feel they are ‘human beings’ of moral worth). Or, to borrow from Asian thought, disrespecting another is to ‘take away’ that other’s ‘face’; to ‘lose face’, in turn, is to diminish that person’s very identity and dignity, and consequently to ‘pollute the web of relationship’ (Rivers 1996: 54–5). Respect, in contrast, keeps ‘the door of relationship’ open (Rivers 1996: 55).
What then are the ingredients of respectful health-professional (nurse–patient) interactions? In conclusion to this discussion on the right to be treated with respect, there is scope to suggest that minimally a nurse’s respectful interactions with patients, chosen carers and significant others must contain the following:
▪ acknowledgment of the moral worth and dignity of human beings
▪ an unconditional positive regard and valuing of persons for who they are as moral beings
▪ focused attention on persons (that is, being ‘fully present’ and being fully alert to another’s presence, viz not treating persons in a dismissive, belittling or marginalising manner)
▪ empathically attuned listening (taking seriously what another says and knows)
▪ supportive actions aimed at promoting another’s moral interests and wellbeing
▪ strategies aimed at ‘saving face’ and preserving the web of relationship.
T he right to cultural liberty
When in health care contexts, people have the right to cultural liberty, that is, the right to maintain their ‘ethnic, linguistic, and religious identities’ — otherwise referred to as ‘cultural rights’ (Fukuda-Parr 2004). Cultural rights claims entail a corresponding duty on the part of health professionals to respect cultural difference as an active component of human rights and development (Marks 2002). Central to the notion of cultural rights is the recognition that culture is not a static process encompassing a frozen set of values, beliefs and practices. Rather it is a process that is ‘constantly recreated as people question, adapt and redefine their values and practices to changing realities and exchanges of idea’ (Fukuda-Parr 2004: 4). Thus, claims to cultural liberty are not about ‘preserving values and practices as an end in itself with blind allegiance to tradition’; they are fundamentally concerned with expanding individual choice and the ‘capability of people to live and be what they choose, with adequate opportunity to consider other options’ (Fukuda-Parr 2004: 4).
The right to cultural liberty is inherently linked to dignity and the right to be treated with respect. And although policy texts overtly champion recognition of cultural rights in health care contexts (see Johnstone & Kanitsaki 2008a), the degree to which cultural liberty and cultural rights are actually respected in such contexts remains a moot point. As with the other patients’ rights discussed in this chapter, the right to cultural liberty is also a right that the nursing profession has a responsibility to protect and uphold. This responsibility is perhaps best articulated in the cultural competency and cultural safety literature, which has begun to burgeon in recent years due to the increasingly diverse and complex ethno-cultural and language profiles of patient populations in multicultural societies the world over (see Johnstone & Kanitsaki 2007a, 2007b, 2008a, 2008b).
C onclusion
The issue of patients’ rights to and in health care is an important one for members of the nursing profession. Although a patients’ rights approach to ethics in health care is not free of difficulties (as examples throughout this book show), it nevertheless serves a number of important functions. Among other things, discourse on patients’ rights helps to remind both health professionals and the laity alike: first, that upon entering health care domains for care and treatment, people have special interests and entitlements which ought to be recognised and protected; second, and related to this first claim, people (patients) are not — and never have been — obliged to be the passive recipients of unnegotiated care. Third, patients’ rights discourse helps to remind health professionals (nurses included) that their relationships with patients and their chosen carers are constrained by morally relevant considerations. Fourth, patients’ rights discourse highlights the vulnerability of people in health care contexts and the ‘special’ actions that are required by others (including nurses) to help reduce this vulnerability and to promote generally the significant moral interests of patients and their chosen carers. Finally, patients’ rights discourse helps to remind us that moral decision-making in health care is not just a matter of ‘working through normative hierarchies of values’, but is also ‘a matter of personal extension into the lives and values of other human beings’ which deserve respect (Thomasma 1990: 250).
Despite the enormous progress that has been made in recent years in regard to the whole issue of patients’ rights to and in health care, it is nevertheless evident that violations of patients’ rights continue to occur across the continuum of care. In light of this, it is morally imperative that the nursing profession takes a proactive stance on the matter of patients’ rights and continues to support and promote them, as and when the need arises.
Case scenario 1
A 20-year-old Jehovah’s Witness woman has given birth to her first child. Unfortunately, following the delivery of her child, she starts to bleed badly. Her attending doctors offer the woman and her husband a stark choice: ‘One hour to decide between a blood transfusion and a hysterectomy’, or else death (Magazanik 1998: 1). If the woman has a hysterectomy, this means that her first child will be her last. The blood transfusion, however, is not an option since it is against her religion. Her refusal to have a blood transfusion is expressed clearly and frequently (both verbally and in writing), has been formally documented, and is widely known by hospital staff. The woman is observed by her husband to be very ‘strong, confident and calm about the whole matter’ (p 2).
A hysterectomy is performed, but the woman continues to bleed and she is transferred to the intensive care unit of a major hospital for further care. She starts to drift in and out of consciousness, and her condition becomes poor. Worried that the woman could die, her attending doctors seek legal advice. The advice received is recorded as follows: ‘Continue supportive measures. Not for blood unless at direction of court.’ (p 2).
The woman’s condition continues to deteriorate and it is probable that, within an hour, she will suffer irreversible brain damage. Distraught at the prospect of his wife dying, the husband changes his mind about a blood transfusion and, upon seeking advice from hospital authorities, successfully obtains a court order giving him legal guardianship over his wife and hence the lawful authority to consent to a blood transfusion being given. The husband provides his consent to hospital authorities immediately and his wife is given a blood transfusion. The woman recovers quickly and is well enough to leave hospital 1 week later.
According to media reports, however, the husband feels ‘guilty’ about the transfusion and the woman is ‘furious’ that the blood was given to her against her wishes. According to a Supreme Court document, the woman stated:
I view the blood transfusion that was forced upon me at the [name of hospital deleted] as equivalent to rape. To me, it feels as if someone has forced an abortion on me while I was under sedation. I am angry about what has happened and I have cried about it a number of times.
(quoted in Magazanik 1998: 2)
The woman is also reported as stating that she ‘would have “screamed” and “fought” against the transfusion had she not been sedated’ and that she is ‘considering suing the hospital, doctors, nurses and lawyers involved in giving her blood’ (p 2). The Jehovah’s Witness organisation is reported to be deeply involved in the legal action that is being pursued, stressing its position that ‘We want to be certain that if people say “I do not want blood”, then that is respected.’ (p 2).
Case scenario 2
A patient who did not speak or understand English was admitted to hospital with a serious medical condition. Five days after he had been admitted an Ethnic Liaison Officer working at the hospital discovered that the man:
… had been in the system for five days and no one had got him an interpreter and explained his physical environment to him… He didn’t know he had access to a buzzer or what it was for and he ended up in a lot of pain. His condition deteriorated very severely overnight and he never rang his buzzer.
(Johnstone & Kanitsaki 2005: 147)
The Ethnic Liaison Officer further discovered that when the staff got to him the morning of his fifth day in hospital, ‘he was in a really bad way and that was a very poor outcome’. In disclosing this case to researchers, he further revealed:
The group that was involved defended themselves incredibly strongly … they think they tell people things but if people can’t understand them, then what is the point? Nothing really severe happened to them, but I think they’re certainly a bit more on their toes.
(p 147)
CRITICAL QUESTIONS
1. What patients’ rights have been violated in these two cases?
2. What were the moral duties of the nurses in these scenarios in regard to upholding and protecting the rights of the patients concerned?
3. How might the violations that occurred in these cases have been prevented?
4. What might be done to assist the patients in the cases whose rights have been violated to come to terms with the aftermath of their experiences?
Endnote
1. Section 4, ‘The right to dignity and dying with dignity’, is revised from Johnstone M-J (1989) ‘Dying with dignity’, New Zealand Nursing Journal 81(12): 34, 37.